Schizophrenia
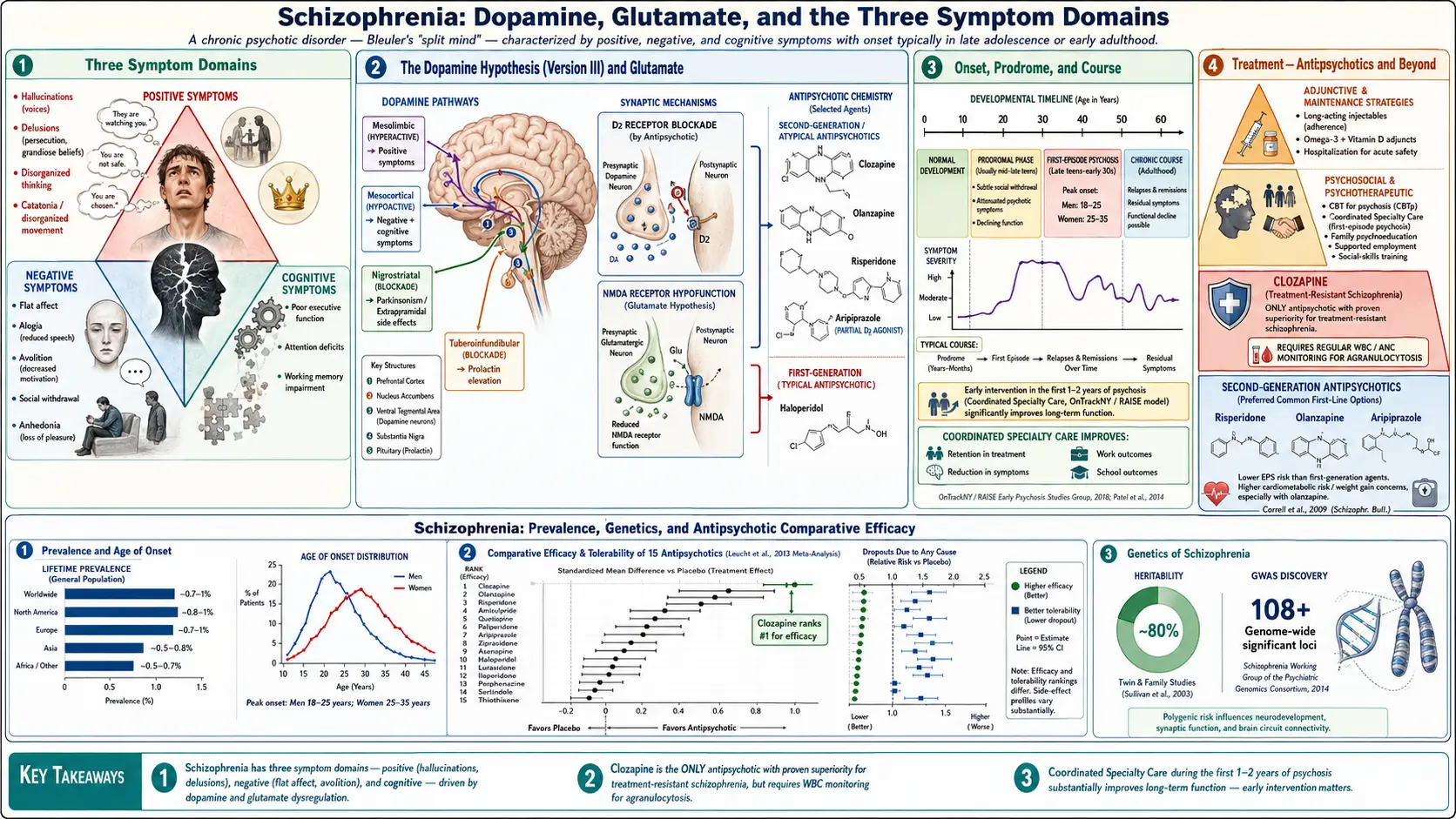
Table of Contents
- What is Schizophrenia?
- The Three Symptom Domains
- Epidemiology and Onset
- Neurobiology: Dopamine and Glutamate
- Diagnosis: DSM-5 Criteria
- First Episode Psychosis
- First-Generation Antipsychotics (FGAs)
- Second-Generation Antipsychotics (SGAs)
- Treatment-Resistant Schizophrenia
- Long-Acting Injectable Antipsychotics
- Psychosocial Treatments
- Comorbidities and Medical Burden
- Research Papers
- Connections
- Featured Videos
What is Schizophrenia?
Schizophrenia is a severe, chronic psychiatric disorder characterized by disturbances in thought, perception, emotion, and behavior that disrupt a person's ability to function. It is not a "split personality" — that is a common but entirely false misconception. Schizophrenia is a psychotic disorder in which reality-testing is fundamentally impaired, meaning the person cannot reliably distinguish what is real from what is not.
The name was coined by Swiss psychiatrist Eugen Bleuler in 1911 (from Greek: schizo = split, phren = mind), referring to a fragmentation of mental functions — not a split between two personalities. Bleuler also introduced the "Four As" as core features: Affective flattening, Associations (loosened), Autism (social withdrawal), and Ambivalence. Emil Kraepelin had earlier called it dementia praecox (early-onset dementia), though dementia is not a defining feature.
Schizophrenia ranks among the top causes of global disability. Without treatment, the course is typically one of progressive functional decline; with adequate treatment, roughly one-third of patients achieve good long-term outcomes, one-third have moderate impairment with relapses, and one-third have severe, ongoing disability. Early, sustained treatment dramatically improves prognosis.
The Three Symptom Domains
Modern psychiatry organizes schizophrenia symptoms into three broad domains: positive, negative, and cognitive. Understanding the difference matters enormously for treatment, because different drugs work — or fail — on different domains.
Positive Symptoms: What is Added
"Positive" does not mean good — it means symptoms that are added to normal experience, things that should not be present but are. These are the dramatic, visible symptoms that most people associate with psychosis.
- Hallucinations — Perceptions without an external stimulus. Auditory hallucinations are by far the most common, occurring in approximately 70% of patients with schizophrenia. Voices may be single or multiple, commenting on the person's behavior, arguing with each other, or issuing commands. Visual, tactile, olfactory, and gustatory hallucinations occur but are less characteristic and should prompt evaluation for underlying neurological or medical causes.
- Delusions — Fixed, false beliefs that are firmly held despite clear evidence to the contrary and are not culturally sanctioned. Common subtypes include:
- Persecutory (most common): "The FBI is monitoring my apartment."
- Referential: "The news anchor is sending me personal messages through the television."
- Grandiose: "I have been chosen to deliver a divine message."
- Bizarre (DSM-5 Criterion A alone): "Aliens have replaced my kidneys with radio transmitters." Bizarre delusions — those that are clearly impossible and not derived from ordinary life experience — carry particular diagnostic weight.
- Thought insertion/withdrawal/broadcasting: Beliefs that one's thoughts are being placed in or removed from one's mind by an outside force, or that others can read one's thoughts.
- Disorganized speech — Reflects disorganized thinking. Manifestations include loose associations (jumping between unrelated topics), tangentiality (responses that veer off topic and never return), circumstantiality (reaching the point only after lengthy irrelevant detail), word salad (complete incoherence), and neologisms (invented words).
- Disorganized or catatonic behavior — Unpredictable agitation, childlike silliness, inappropriate affect, or grossly disorganized actions that interfere with goal-directed activity. Catatonia exists on a spectrum: stupor, waxy flexibility, mutism, negativism (active resistance to instructions), posturing, stereotypies, and at the extreme, excited catatonia with dangerous purposeless motor activity.
Negative Symptoms: What is Taken Away
"Negative" means symptoms representing a diminution of normal function. Often described as the "Five As," these are frequently more disabling in the long run than positive symptoms because they undermine the person's ability to work, maintain relationships, and care for themselves — and they respond poorly to current antipsychotic medications.
- Affective flattening (Blunted affect) — Reduced range and intensity of emotional expression. The face appears immobile, voice is monotone, body language is minimal. This is not the same as depression; the person may not feel inwardly depressed.
- Alogia — Poverty of speech: brief, laconic replies; long pauses before responding; reduced spontaneous speech output. Reflects reduced thought generation, not hearing difficulty or willful silence.
- Avolition — Profound lack of motivation to initiate and sustain goal-directed activities. Basic tasks — showering, laundry, job-seeking — feel insurmountably effortful. This is not laziness; it reflects genuine neurobiological drive deficits.
- Anhedonia — Reduced ability to experience pleasure from activities formerly enjoyed, as well as reduced anticipatory pleasure (the sense of looking forward to things).
- Asociality — Decreased desire for social interaction and relationships; social withdrawal. Distinct from social anxiety; the person may not experience discomfort in social settings so much as simply no motivation to seek them out.
Cognitive Symptoms: The Hidden Deficit
Cognitive impairment in schizophrenia is now recognized as a core, not peripheral, feature of the illness — and critically, it is present before the first psychotic episode, even during childhood and adolescence. It persists throughout the illness course and is one of the strongest predictors of functional outcome.
- Working memory — Difficulty holding information in mind to use in reasoning and actions. Simple example: forgetting the beginning of a sentence before finishing it.
- Processing speed — Everything takes longer; reaction times are slower; mental work requires more effort per unit of output.
- Executive function — Planning, sequencing, cognitive flexibility, abstract reasoning, and problem-solving are impaired. This is primarily a prefrontal cortex deficit.
- Verbal learning and memory — Difficulty encoding and recalling verbal information, relevant to following conversations and instructions.
- Attention and vigilance — Sustained focus is impaired; distracted by irrelevant stimuli.
The average cognitive deficit in schizophrenia is roughly 1–2 standard deviations below population norms across most domains. No currently approved medication significantly improves cognition.
Epidemiology and Onset
Schizophrenia affects approximately 0.3–0.7% of the global population by strict DSM-5/ICD-11 criteria, though broader estimates incorporating the schizophrenia spectrum (including schizoaffective disorder, schizophreniform disorder, and schizotypal personality disorder) approach 1%. The condition is found in all cultures, ethnic groups, and societies studied, though rates may vary two- to threefold across sites, partly reflecting diagnostic and ascertainment differences.
Age of Onset
- Men: Onset typically in the early to mid-20s (peak 18–25). Onset before age 13 (very-early-onset) and after 40 (late-onset) are recognized but uncommon.
- Women: Onset is later — typically mid-20s to early 30s, with a second, smaller peak around menopause (age 45–50). Estrogen is thought to have antidopaminergic, neuroprotective properties that delay onset and moderate severity.
- Women generally have better premorbid functioning, more prominent affective symptoms, and somewhat better long-term outcomes than men.
Prodrome
The prodromal phase — the period before the first clear psychotic episode — may last months to years and is characterized by attenuated (subthreshold) psychotic symptoms, social withdrawal, decline in academic or work performance, oddities of speech and behavior, and mood disturbances. Early Psychosis Detection programs aim to identify individuals in the prodrome to initiate coordinated care before the first psychotic break.
Risk Factors
- Genetics: Heritability estimated at 64–80%. First-degree relatives have ~10% lifetime risk (vs ~1% general population); monozygotic twin concordance ~40–50%, showing substantial but incomplete genetic determination. Genome-wide association studies (GWAS) have identified over 100 independent genetic loci, but each confers small individual risk. Copy number variants — especially 22q11.2 deletion — carry substantial risk (~25% develop psychosis).
- Obstetric complications: Hypoxia, preterm birth, intrauterine infection, maternal nutritional deficiency (especially folic acid and vitamin D), and maternal stress during pregnancy all modestly increase risk.
- Urban birth and upbringing: Consistently associated with ~2x risk; mechanisms debated (social adversity, pollution, infection exposure, reduced vitamin D, social fragmentation).
- Migration: First- and second-generation migrants show elevated rates in several studies, potentially reflecting social defeat, isolation, and chronic stress.
- Cannabis use: Heavy adolescent cannabis use is associated with 2–4x increased risk of psychosis. High-THC products carry greater risk. THC acutely induces transient psychotic-like experiences in healthy individuals; regular use in those with genetic vulnerability appears to trigger earlier onset. This is likely a causal relationship, not only reverse causation.
- Neurodevelopmental insults: Winter/spring birth (consistent with prenatal influenza exposure), viral infections during second trimester, childhood trauma, and Toxoplasma gondii infection have each been associated with increased risk in epidemiological studies.
Neurobiology: Dopamine and Glutamate Hypotheses
No single brain lesion or biomarker defines schizophrenia, but decades of research have converged on two overlapping neurobiological frameworks: the dopamine hypothesis and the glutamate/NMDA receptor hypothesis. These are not competing theories but complementary perspectives that illuminate different symptom domains.
The Dopamine Hypothesis
The dopamine hypothesis has been refined across three versions since the 1960s. The current formulation (sometimes called "dopamine hypothesis version 3") distinguishes between mesolimbic and mesocortical dopamine pathways:
- Mesolimbic hyperactivity leads to positive symptoms. The mesolimbic pathway runs from the ventral tegmental area (VTA) to the nucleus accumbens, amygdala, and hippocampus. Excessive D2 receptor stimulation in this pathway is thought to underlie the aberrant salience that drives delusions and hallucinations — the brain assigns meaning and urgency to neutral perceptions and random internal thoughts. Evidence:
- All effective antipsychotics block D2 receptors; antipsychotic efficacy correlates with D2 occupancy (~65–80% optimal).
- Drugs that release dopamine (amphetamine, cocaine, L-DOPA) reliably induce or worsen psychotic symptoms.
- PET studies show elevated striatal dopamine synthesis capacity in schizophrenia, especially during acute psychosis.
- Mesocortical hypoactivity leads to negative and cognitive symptoms. The mesocortical pathway runs from the VTA to the prefrontal cortex (PFC). Insufficient dopamine signaling in the PFC — particularly at D1 receptors — impairs the "gating" function of the PFC, disrupting working memory, executive function, and motivational drive. This explains why simply increasing D2 blockade (as antipsychotics do) fails to improve and may even worsen negative and cognitive symptoms: you are further suppressing an already hypoactive cortical system.
The Glutamate / NMDA Receptor Hypothesis
The NMDA (N-methyl-D-aspartate) receptor hypofunction hypothesis emerged from the observation that NMDA receptor antagonists — ketamine and phencyclidine (PCP, "angel dust") — reproduce all three symptom domains of schizophrenia in healthy individuals: positive, negative, AND cognitive symptoms. This distinguishes the ketamine model from the dopamine (amphetamine) model, which reproduces mainly positive symptoms.
- NMDA receptor hypofunction on inhibitory GABAergic interneurons (particularly parvalbumin-positive fast-spiking interneurons) leads to disinhibition of downstream glutamate neurons, producing a paradoxical excess of excitatory glutamate transmission in some circuits.
- This framework predicts that positive glutamate modulation — at glycine sites, metabotropic glutamate receptors (mGluR2/3), or via AMPA potentiation — may be therapeutic. Multiple clinical trials are underway.
- The 2024 FDA approval of KarXT (xanomeline-trospium) — a muscarinic M1/M4 agonist — as a first-in-class antipsychotic without direct D2 blockade is partly informed by this model: muscarinic receptors modulate cortical glutamate circuitry.
Structural Brain Findings
Meta-analyses of neuroimaging consistently show modest but reliable structural differences in schizophrenia compared with controls: enlarged lateral ventricles, reduced total gray matter volume (particularly in prefrontal cortex, superior temporal gyrus, and hippocampus), and reduced cortical thickness. These changes are present at illness onset and are not simply medication effects, though antipsychotics — especially at high doses — may contribute to gray matter volume changes over time.
Diagnosis: DSM-5 Criteria
Schizophrenia is a clinical diagnosis — there is no blood test, imaging finding, or genetic marker that is diagnostic. A thorough psychiatric history, mental status examination, and collateral information from family are essential. The DSM-5 requires:
Criterion A: Core Symptoms
At least two of the following five symptoms, each present for a significant portion of a one-month period (or less if successfully treated). At least one must be delusions, hallucinations, or disorganized speech (items 1–3):
- Delusions
- Hallucinations
- Disorganized speech
- Grossly disorganized or catatonic behavior
- Negative symptoms
Note: A single bizarre delusion or Schneiderian first-rank symptom (e.g., auditory hallucinations with running commentary, thought insertion/withdrawal/broadcasting, made actions) previously required only one Criterion A symptom in DSM-IV. DSM-5 eliminated this shortcut and requires two symptoms regardless.
Criterion B: Social/Occupational Dysfunction
For a significant portion of time since onset, functioning in one or more major areas — work, interpersonal relations, self-care — is markedly below the level achieved before onset. In children/adolescents: failure to achieve expected level of development.
Criterion C: Duration
Continuous signs of disturbance persist for at least 6 months, including at least 1 month of Criterion A symptoms (or less with successful treatment). Prodromal or residual periods may include only attenuated symptoms (odd beliefs, unusual perceptual experiences, poverty of speech).
Differential Diagnosis
Several conditions must be ruled out before diagnosing schizophrenia:
- Schizoaffective disorder: Psychosis with concurrent mood episodes (mania or depression) present for a substantial portion of the illness.
- Brief psychotic disorder: Duration 1 day to 1 month, then full recovery.
- Schizophreniform disorder: Meets Criterion A but total duration 1–6 months.
- Bipolar disorder with psychotic features: Psychosis only during mood episodes.
- Substance-induced psychotic disorder: Direct physiological effect of a substance (cannabis, stimulants, hallucinogens, steroids).
- Medical conditions: Temporal lobe epilepsy, anti-NMDA receptor encephalitis (an autoimmune condition that is acutely treatable), Wilson's disease, thyroid disorders, CNS tumors, Huntington's disease, HIV-associated dementia, tertiary syphilis.
First Episode Psychosis
First Episode Psychosis (FEP) — the first clear break with reality — is a critical juncture in the illness. How it is handled in the first weeks and months can significantly influence the long-term trajectory.
Duration of Untreated Psychosis (DUP)
The Duration of Untreated Psychosis (DUP) is the time from onset of clear psychotic symptoms to initiation of antipsychotic treatment. A shorter DUP is consistently associated with:
- Faster and more complete response to treatment
- Lower risk of relapse
- Better long-term functional outcomes
- Less structural brain change
Despite this, the average DUP in most healthcare systems remains more than one year — a major public health failure. Early Psychosis Intervention (EPI) programs aim to reduce DUP to weeks rather than months.
Medical Baseline Before Starting Antipsychotics
Before initiating antipsychotic therapy, obtain a baseline metabolic and safety workup, because these medications carry significant metabolic risks:
- Weight and BMI
- Fasting blood glucose and HbA1c
- Fasting lipid panel (total cholesterol, LDL, HDL, triglycerides)
- Blood pressure and pulse
- Complete blood count (CBC) — essential before clozapine
- Liver function tests (LFTs) and renal function
- Prolactin level
- EKG (QTc interval, especially before medications that prolong QT)
- Thyroid function (TSH)
- Urine drug screen (to assess substance contribution)
- Anti-NMDA receptor antibodies if clinically indicated (young woman, rapid onset, fever, movement disorder)
Coordinated Specialty Care (CSC)
Evidence strongly supports intensive, team-based Coordinated Specialty Care for FEP — combining low-dose antipsychotic medication, individual and family therapy, supported employment/education, and case management. The NAVIGATE and RAISE trials demonstrated that CSC significantly outperforms usual care for functional recovery, not just symptom reduction. In the US, CSC programs are increasingly funded through state mental health authorities.
First-Generation Antipsychotics (FGAs)
First-generation antipsychotics — also called "typical" antipsychotics or conventional antipsychotics — were the first effective pharmacological treatments for psychosis, introduced in the 1950s. They work primarily through high-affinity D2 receptor blockade, which accounts for both their antipsychotic efficacy and their troublesome neurological side effects.
Common FGAs
- Haloperidol (Haldol) — High-potency; preferred in acute agitation; available as oral, IM, and depot (LAI). Minimal sedation and anticholinergic effects but high EPS risk.
- Chlorpromazine (Thorazine) — The first antipsychotic (1952); low-potency; more sedating and anticholinergic. Useful when sedation is desired.
- Fluphenazine, Perphenazine, Thiothixene, Loxapine — Intermediate to high potency; varying side-effect profiles.
- Thioridazine — Withdrawn from routine use due to QTc prolongation and retinal pigmentation risk; reserved for refractory cases.
Extrapyramidal Side Effects (EPS)
The nigrostriatal dopamine pathway controls motor function; blocking it with FGAs produces neurological side effects collectively called extrapyramidal symptoms:
- Akathisia — Subjective inner restlessness and compulsion to move; one of the most distressing and adherence-limiting side effects. Often misdiagnosed as anxiety or agitation, which may lead to dose escalation — the wrong response. Treatment: dose reduction, beta-blockers (propranolol), or benzodiazepines.
- Drug-induced parkinsonism — Tremor, rigidity, bradykinesia, masked facies; reversible with dose reduction or anticholinergics (benztropine, diphenhydramine).
- Acute dystonia — Sudden, painful sustained muscle contractions (neck, jaw, back, eyes); more common in young men and with high-potency drugs. Dramatic and frightening for patients. Treated rapidly with IM or IV benztropine or diphenhydramine.
- Tardive dyskinesia (TD) — Involuntary, repetitive movements typically involving the face, lips, tongue, and extremities that emerge after months to years of antipsychotic exposure. Caused by postsynaptic D2 receptor supersensitivity from chronic blockade. TD is irreversible in many patients; risk increases with cumulative dose and duration of treatment, older age, female sex, and prior EPS. Annual prevalence in patients on FGAs: ~5% per year of exposure. VMAT2 inhibitors — valbenazine (Ingrezza) and deutetrabenazine (Austedo) — are FDA-approved for TD and are effective, though expensive.
Neuroleptic Malignant Syndrome (NMS)
NMS is a rare (0.01–0.02%) but potentially fatal reaction to antipsychotics. The classic tetrad is: fever (often high-grade), muscle rigidity (lead-pipe), autonomic instability (labile blood pressure, tachycardia, diaphoresis), and altered consciousness. Elevated CK (often markedly, over 1,000 U/L), leukocytosis, and elevated LFTs support the diagnosis. Treatment: immediate discontinuation of the offending drug, supportive care, dantrolene (muscle relaxant), bromocriptine or amantadine (dopamine agonists to reverse blockade), cooling measures. Benzodiazepines for agitation. Mortality with appropriate treatment ~5–10% but was historically 25–30%.
Second-Generation Antipsychotics (SGAs)
Second-generation antipsychotics — also called "atypical" antipsychotics — differ from FGAs primarily in their combined D2 and serotonin 5-HT2A receptor antagonism (and varying activity at histamine, muscarinic, and alpha-adrenergic receptors), lower rates of EPS and tardive dyskinesia, and greater heterogeneity of mechanisms. They became first-line treatment in the 1990s.
The landmark CATIE trial (Clinical Antipsychotic Trials of Intervention Effectiveness, 2005; Lieberman et al., NEJM) was a sobering reality check: in an 18-month pragmatic real-world comparison, the FGA perphenazine performed comparably to most SGAs on the primary outcome (time to discontinuation for any cause, ~74% at 18 months for all drugs). Olanzapine lasted longest but with worse metabolic side effects. No SGA was clearly superior to perphenazine except in specific subgroups. The trial underscored that all antipsychotics are imperfect and that effectiveness (real-world outcomes) differs from efficacy (controlled trial performance).
Major SGAs
- Olanzapine (Zyprexa) — Highly effective for positive symptoms; significant metabolic side effects: average 4–10 kg weight gain, substantial risk of new-onset type 2 diabetes and hyperlipidemia. One of the most efficacious SGAs short of clozapine, but metabolic monitoring is mandatory.
- Risperidone (Risperdal) — Effective; EPS risk is dose-dependent (lower at doses 6 mg/day or less, higher at doses approaching FGA-like range); prolactin elevation is prominent (hyperprolactinemia, galactorrhea, sexual dysfunction, osteoporosis risk long-term); available as LAI (Risperdal Consta, Perseris).
- Quetiapine (Seroquel) — Highly sedating; widely used for insomnia and anxiety comorbidities; low EPS and prolactin; moderate metabolic risk; weaker antipsychotic at doses typically used in clinical practice for sleep.
- Aripiprazole (Abilify) — Unique mechanism: partial D2 agonist (stabilizes dopamine activity — agonist where dopamine is low, antagonist where high); also partial 5-HT1A agonist; relatively weight-neutral; activating (may cause akathisia and insomnia); available as LAI (Maintena, Aristada).
- Ziprasidone (Geodon) — Weight-neutral; must be taken with food (requires 500 kcal for adequate absorption); QTc prolongation risk; avoid in combination with other QTc-prolonging agents.
- Paliperidone (Invega) — Active metabolite of risperidone; similar profile; widely used as LAI (Sustenna monthly, Trinza quarterly, Hafyera twice-yearly).
- Lurasidone (Latuda) — Effective; minimal weight gain and metabolic effects; must be taken with food (350 kcal or more); FDA-approved for schizophrenia and bipolar depression.
- Cariprazine (Vraylar) — Partial D2/D3 agonist with preferential D3 affinity; evidence for negative symptom efficacy over risperidone in trials; activating.
- KarXT (Cobenfy, xanomeline-trospium, approved 2024) — First antipsychotic approved that does not act directly on dopamine D2 receptors. Xanomeline is a muscarinic M1/M4 agonist; trospium (a peripheral muscarinic antagonist) is added to reduce the peripheral cholinergic side effects of xanomeline. Phase 3 trials showed significant improvement in positive and negative symptoms vs placebo. Represents a new mechanistic class with potential for better cognitive outcomes.
A Note on Negative Symptoms
All currently available antipsychotics — both FGA and SGA — provide limited benefit for negative symptoms. SGAs may have a modest advantage, particularly via secondary negative symptom improvement (by reducing EPS and depression that masquerade as primary negative symptoms), but primary negative symptoms remain the major unmet therapeutic need in schizophrenia. KarXT and several investigational muscarinic and glutamate-modulating agents are being studied specifically for this indication.
Treatment-Resistant Schizophrenia and Clozapine
Approximately 30% of patients with schizophrenia fail to achieve adequate symptom control despite two or more adequate antipsychotic trials — each at an adequate dose (typically 600 mg/day or more chlorpromazine equivalents) for an adequate duration (6–8 weeks). This is called Treatment-Resistant Schizophrenia (TRS).
Clozapine: The Gold Standard for TRS
Clozapine was introduced in the early 1970s and remains the only antipsychotic with proven superiority for TRS — meaning it works when nothing else does. The landmark Kane et al. 1988 trial (Archives of General Psychiatry) demonstrated clozapine's superiority over chlorpromazine in treatment-resistant patients. Subsequent trials confirmed that clozapine also uniquely reduces suicide risk (FDA-approved for suicidality in schizophrenia and schizoaffective disorder), a finding unique among antipsychotics.
Clozapine's mechanism is complex: low D2 affinity (which explains the absence of EPS), combined with antagonism at 5-HT2A, 5-HT2C, H1, M1, M2, M4, alpha-1, and alpha-2 receptors. The exact mechanism of its superior antipsychotic efficacy in TRS remains unclear but likely involves this multi-receptor profile.
Why Clozapine Is Underused
Despite its proven efficacy, clozapine is dramatically underutilized globally. The main barrier is its serious side-effect profile, which requires intensive monitoring:
- Agranulocytosis — Potentially fatal loss of granulocytes (white blood cells essential for fighting infection), occurring in approximately 1–2% of patients, most commonly in the first 6 months. This is why clozapine requires enrollment in the CLOZARIL REMS (Risk Evaluation and Mitigation Strategy) program in the US. CBC with differential must be obtained weekly for the first 6 months, then every 2 weeks for 6 months, then monthly. Clozapine is withheld if the ANC falls below 1,000/uL and discontinued if it falls below 500/uL.
- Metabolic side effects — Among the highest of all antipsychotics: weight gain (average 4–10 kg), insulin resistance, type 2 diabetes, hyperlipidemia. Metformin and lifestyle intervention are often co-prescribed.
- Seizures — Dose-dependent risk (~5% at doses above 600 mg/day). Often treated with valproate (note: valproate raises clozapine levels; monitor).
- Myocarditis — Rare but serious inflammatory cardiac complication in the first 4 weeks of initiation; baseline troponin and CRP monitoring is recommended in some protocols.
- Sialorrhea (hypersalivation) — Problematic and embarrassing; treated with anticholinergics or glycopyrrolate.
- Sedation, constipation, orthostatic hypotension — Common, manageable side effects.
Despite these challenges, clozapine's efficacy advantage for TRS is so substantial that most guidelines recommend not waiting to try it when two antipsychotic trials have failed. Delaying clozapine costs years of unnecessary suffering.
Long-Acting Injectable Antipsychotics (LAIs)
Medication non-adherence is the single largest driver of relapse in schizophrenia — and it is the rule rather than the exception. Studies show that 40–60% of outpatients with schizophrenia are partially or fully non-adherent to oral antipsychotics within the first year of treatment.
Long-acting injectable (LAI) antipsychotics — also called depot antipsychotics — are formulations that are injected once every 2, 4, 8, or even 24 weeks, providing sustained drug delivery with no daily pill-taking required. When patients cannot or do not reliably take daily medication (due to cognitive impairment, insight problems, disorganization, or simply disliking the medication experience), LAIs can be life-changing.
Available LAIs
- Paliperidone palmitate — Invega Sustenna (monthly), Invega Trinza (quarterly), Invega Hafyera (twice-yearly). The longest-acting LAI formulation available.
- Aripiprazole — Abilify Maintena (monthly), Aristada (monthly/6-weekly), Aristada Initio (one-time initiation dose).
- Risperidone — Risperdal Consta (every 2 weeks), Perseris (monthly subcutaneous).
- Olanzapine pamoate — Zyprexa Relprevv (every 2–4 weeks); requires 3-hour post-injection monitoring in a healthcare facility due to rare but serious post-injection delirium/sedation syndrome.
- Haloperidol decanoate, fluphenazine decanoate — Older FGA-based LAIs; still widely used globally due to cost.
Evidence Base
Meta-analyses (including Correll et al. 2016) consistently demonstrate that LAIs reduce relapse rates by approximately 30–50% compared to equivalent oral formulations in real-world settings, driven primarily by adherence improvement. The benefit is largest in patients with prior non-adherence, substance comorbidities, and lack of insight. Many clinicians offer LAIs earlier in the illness course — not just for the "difficult" patient — to prevent the accumulating harm of repeated relapses.
Psychosocial Treatments
Medication manages symptoms; psychosocial interventions rebuild life. The evidence base for several psychosocial treatments is now robust enough that they are recommended in all major guidelines as integral to treatment, not optional add-ons.
Cognitive Remediation Therapy (CRT)
CRT uses repeated, computerized or paper-based exercises to improve specific cognitive domains — attention, memory, executive function, processing speed — combined with a therapist's support for "bridging" gains to real-world tasks. Meta-analyses (McGurk et al., Wykes et al.) show modest but real improvements in cognition (effect sizes ~0.4–0.5 SD) and, importantly, in functional outcomes when CRT is combined with psychiatric rehabilitation. Cognitive Enhancement Therapy (CET) is the most evidence-based manualized program, originally developed by Hogarty and Greenwald.
Individual Placement and Support (IPS)
The IPS model of supported employment is based on the principle that people with severe mental illness can and want to work, and that competitive employment in real-world jobs is both achievable and therapeutic. IPS places people directly in competitive jobs with ongoing job-coach support, rather than first providing prevocational training. Multiple randomized trials show IPS produces competitive employment rates of 50–60% versus ~25% for traditional vocational rehabilitation. Work — any work — is associated with improved symptoms, self-esteem, and quality of life.
Family Psychoeducation
Family psychoeducation programs — providing structured information about schizophrenia, reducing expressed emotion (criticism, hostility, overinvolvement), and teaching communication and problem-solving skills — reduce relapse rates by approximately 20% compared to treatment as usual. They are most effective when delivered over at least 9 months. Families are not causes of schizophrenia (the "refrigerator mother" hypothesis was wrong and harmful) but they are powerful allies in recovery.
Cognitive Behavioral Therapy for Psychosis (CBTp)
CBT adapted for psychosis addresses the meaning patients attach to psychotic experiences, reality-testing of delusional beliefs, distress reduction from voices, and behavioral avoidance. It does not eliminate psychotic symptoms but reduces distress and improves coping. UK NICE guidelines recommend CBTp for all people with schizophrenia.
Social Skills Training
Structured training in interpersonal skills (conversation, assertiveness, conflict resolution, medication management) shows consistent improvements in social functioning, though generalization to real-world settings requires ongoing practice and support.
Comorbidities and Medical Burden
People with schizophrenia die on average 15–25 years earlier than the general population. The majority of this excess mortality is not from suicide — it is from cardiovascular disease, diabetes, infection, and respiratory disease. This life expectancy gap has not narrowed, and may have widened, over recent decades, reflecting the combined burden of illness-related lifestyle factors, antipsychotic metabolic effects, and systematic healthcare disparities.
- Metabolic syndrome: Occurs in approximately 3 times the general population rate. Driven by antipsychotic-induced weight gain, sedentary lifestyle (from negative symptoms and side effects), poor diet, and illness-related metabolic dysregulation. Regular monitoring — weight, glucose, lipids, blood pressure — at every clinical contact is the standard of care, but is rarely achieved in practice.
- Smoking: 60–80% of people with schizophrenia smoke cigarettes, compared to ~15% of the general adult population. Nicotine acutely reduces some symptoms (stimulates nicotinic receptors, improving attention and sensory gating) but long-term health consequences are devastating. Smoking also dramatically lowers antipsychotic blood levels by inducing CYP1A2 (relevant particularly for clozapine and olanzapine). Smoking cessation with varenicline (Chantix) is safe and effective in schizophrenia and is strongly recommended.
- Substance use disorders (SUD): Affect approximately 50% of people with schizophrenia over the lifetime (alcohol, cannabis, stimulants). SUD dramatically worsens outcomes — increases positive symptoms, reduces medication adherence, drives homelessness and incarceration. Clozapine has some evidence for reducing comorbid substance use.
- Depression: Present in up to 50% of patients at some point; may be difficult to distinguish from negative symptoms, medication-induced dysphoria, or grief about the illness.
- Suicide: Lifetime risk of suicide in schizophrenia is approximately 5–10% — roughly 20–50 times the general population rate. Suicide risk is highest early in the illness course, during insight-gaining phases, during depressive episodes within the illness, and following hospital discharge. Risk factors: younger age, male sex, higher IQ and education (more awareness of functional loss), depression, command hallucinations, hopelessness, prior attempts, substance use. Clozapine is the only antipsychotic proven to reduce suicide risk.
- Tardive dyskinesia: Affects 20–30% of patients on long-term antipsychotics; severely impacts quality of life and stigma.
- Vitamin D deficiency: Highly prevalent due to reduced sun exposure, smoking, and institutionalization; may exacerbate cognitive symptoms.
Research Papers
Historical Context
The modern pharmacological era of schizophrenia began with chlorpromazine in 1952, discovered serendipitously during surgical anesthesia research by Henri Laborit and first used psychiatrically by Jean Delay and Pierre Deniker in Paris. The dopamine hypothesis crystallized in the 1960s–70s through work by Arvid Carlsson (Nobel Prize 2000) and Philip Seeman. Clozapine's landmark TRS trial by Kane et al. in 1988 established the concept of treatment-resistant schizophrenia as a distinct clinical entity requiring a distinct treatment approach.
Key Research Papers
- Howes OD, Kapur S. The dopamine hypothesis of schizophrenia: version III — the final common pathway. Schizophrenia Bulletin. 2009;35(3):549-562. PMID 19325164.
- Kane J, et al. Clozapine for the treatment-resistant schizophrenic: a double-blind comparison with chlorpromazine. Archives of General Psychiatry. 1988;45(9):789-796. PMID 3046553.
- Lieberman JA, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia (CATIE Trial). New England Journal of Medicine. 2005;353(12):1209-1223. PMID 16172203.
- Correll CU, et al. Comparison of early-intervention services vs treatment-as-usual for early-phase psychosis. JAMA Psychiatry. 2018;75(6):555-565. PMID 29800949.
- Kay SR, et al. The Positive and Negative Syndrome Scale (PANSS) for schizophrenia. Schizophrenia Bulletin. 1987;13(2):261-276. PMID 3616518.
- McGurk SR, et al. A meta-analysis of cognitive remediation in schizophrenia. American Journal of Psychiatry. 2007;164(12):1791-1802. PMID 18056233.
- Laursen TM, et al. Life expectancy and cardiovascular mortality in persons with schizophrenia. Current Opinion in Psychiatry. 2012;25(2):83-88. PMID 22249081.
- Insel TR. Rethinking schizophrenia. Nature. 2010;468(7321):187-193. PMID 21068826.
- Mueser KT, McGurk SR. Schizophrenia. The Lancet. 2004;363(9426):2063-2072. PMID 15207959.
- Howes OD, et al. Midbrain dopamine function in schizophrenia and depression. Brain. 2009;132(Pt 11):2997-3005. PMID 18772223.
- Stahl SM, et al. KarXT (xanomeline-trospium) for schizophrenia: Phase 3 EMERGENT-2 trial. American Journal of Psychiatry. PubMed: KarXT EMERGENT schizophrenia trials.
- Correll CU, et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness. World Psychiatry. 2017;16(2):163-180. PMID 28498599.
PubMed Topic Searches
- PubMed: schizophrenia dopamine hypothesis
- PubMed: schizophrenia NMDA glutamate
- PubMed: clozapine treatment-resistant schizophrenia
- PubMed: schizophrenia negative symptoms treatment
- PubMed: schizophrenia cognitive impairment remediation
- PubMed: schizophrenia LAI antipsychotic relapse
- PubMed: tardive dyskinesia antipsychotic prevalence
- PubMed: first episode psychosis early intervention
- PubMed: schizophrenia metabolic syndrome mortality
- PubMed: schizophrenia genetics GWAS
- PubMed: schizophrenia suicide risk
- PubMed: schizophrenia cannabis risk psychosis
Connections
- Psychiatry
- Bipolar Disorder
- Depression
- ADHD
- Addiction
- Dementia
- Anxiety
- Vitamin D3
- Omega-3 Fatty Acids
- Magnesium
- Zinc
- NAC and Mental Health
- Sleep Hygiene
- Insomnia
- Stress Management
- Vitamin B12
- Postpartum Depression
- Tryptophan and Cognitive Function