Niacin for Schizophrenia and Mental Health — Orthomolecular Psychiatry
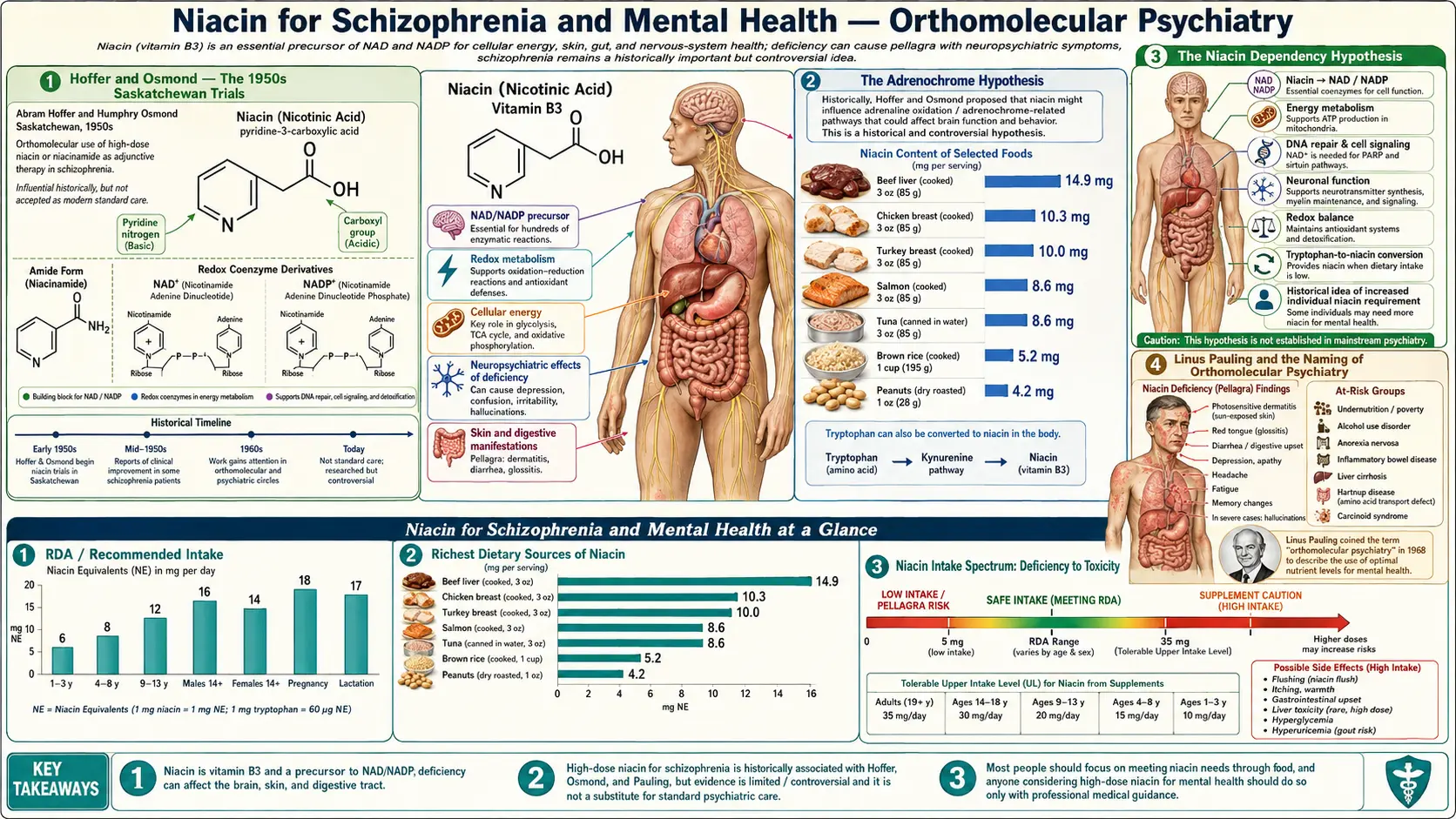
In the 1950s, Saskatchewan psychiatrists Abram Hoffer and Humphry Osmond hypothesized that schizophrenia was a niacin-dependency disorder — an inability to convert tryptophan to NAD+ at normal rates, leading to accumulation of psychotomimetic metabolites. They ran the first double-blind placebo-controlled trials in the history of psychiatry, and reported improved outcomes with 3-18 g/day niacin. Linus Pauling embraced their work in 1968 and coined the term "orthomolecular psychiatry." Later controlled trials in the 1970s by Wittenborn and others failed to replicate the dramatic effects, and mainstream psychiatry largely abandoned the approach by 1980. But the underlying biochemistry remained interesting: the niacin flush test (reduced or absent flush in ~40% of schizophrenia patients) is a real and replicated endophenotype, frank pellagra causes psychosis that fully reverses with niacin, and the tryptophan-kynurenine-quinolinic acid axis remains an active area of psychiatric research. This page walks the history honestly, separates the documented from the overstated, and locates the realistic modern place of high-dose B3 in psychiatry.
Table of Contents
- Hoffer and Osmond — The 1950s Saskatchewan Trials
- The Adrenochrome Hypothesis
- The Niacin Dependency Hypothesis
- Linus Pauling and the Naming of Orthomolecular Psychiatry
- The Niacin Flush Test — A Real Endophenotype
- Why Later Controlled Trials Disappointed
- The 1973 APA Task Force Verdict
- Pellagra Psychosis — The Genuine Niacin-Psychosis Link
- The Tryptophan-Kynurenine-Quinolinic Acid Axis
- Niacin in OCD, Anxiety, and Depression
- The Realistic Modern Place of High-Dose B3
- Cautions
- Key Research Papers
- Connections
- Featured Videos
Hoffer and Osmond — The 1950s Saskatchewan Trials
Abram Hoffer (a Canadian biochemist and psychiatrist, PhD in biochemistry from the University of Minnesota, MD from the University of Toronto) and Humphry Osmond (a British psychiatrist who coined the word "psychedelic" in correspondence with Aldous Huxley) worked together at the Saskatchewan Hospital in Weyburn starting in 1952. They were responsible for one of the most ambitious clinical research programs in the early history of biological psychiatry.
Their first published trial (Hoffer, Osmond, and Smythies, Journal of Mental Science, 1954) was one of the very first double-blind placebo-controlled trials in psychiatry — predating the modern RCT era. The design:
- 30 newly admitted acutely psychotic schizophrenia patients
- Randomized to nicotinic acid 3 g/day, nicotinamide 3 g/day, or placebo
- Outcomes assessed at 1 month, 1 year, and longer
Hoffer and Osmond reported a roughly doubled recovery rate in the niacin-treated arms compared to placebo at the 1-year mark, with sustained improvement in subsequent follow-up cohorts. They subsequently conducted larger non-randomized series in thousands of patients over the next two decades, consistently reporting that early intervention with high-dose niacin (3-18 g/day, often combined with vitamin C, vitamin B6, and zinc) significantly improved long-term outcomes.
Their work was an explicit challenge to the psychoanalytic establishment of the 1950s — which insisted schizophrenia was a disorder of childhood trauma and mother-blame — and predated the antipsychotic-receptor era by 20 years.
The Adrenochrome Hypothesis
Hoffer and Osmond's mechanistic hypothesis was based on chemistry that was state-of-the-art for the 1950s and remains chemically plausible (though clinically unconfirmed):
- Adrenaline oxidation product. Adrenochrome is the spontaneous oxidation product of adrenaline (epinephrine) — a pink-violet molecule formed when adrenaline encounters oxygen. Hoffer and Osmond proposed that schizophrenia patients had impaired ability to metabolize adrenaline normally, leading to accumulation of psychotomimetic adrenochrome and related quinone derivatives.
- Methylation defect. Normal adrenaline metabolism via catechol-O-methyltransferase (COMT) requires methyl-group donation. Hoffer and Osmond proposed that schizophrenia patients had a methylation defect, with adrenaline shunted into the oxidative pathway producing adrenochrome.
- Niacin as methyl sink. The hypothesis: niacin, being methylated to N1-methylnicotinamide before urinary excretion, acts as a "methyl sink" that draws methyl groups away from the adrenaline-oxidation pathway. This is paradoxical — normally we think of niacin supporting methylation, not depleting it — but the hypothesis was that B3 at gram-range doses competed with adrenaline for the available methylation capacity.
- Adrenochrome experiments. Hoffer, Osmond, and others reported that small doses of synthesized adrenochrome injected into healthy volunteers produced psychotomimetic effects resembling schizophrenia — supporting (though not proving) the hypothesis.
The adrenochrome hypothesis was never decisively confirmed or refuted. Later research showed that adrenochrome is much more chemically reactive than originally appreciated and is unlikely to accumulate in the bloodstream long enough to produce psychotomimetic effects in vivo. But the broader insight — that abnormal one-carbon metabolism might contribute to psychiatric disease — has been validated repeatedly in modern psychiatric biochemistry (folate, B12, MTHFR, homocysteine).
The Niacin Dependency Hypothesis
Hoffer's second hypothesis was more durable: that a subset of schizophrenia patients suffer from a partial niacin-dependency disorder — analogous to but milder than the inborn errors of B6 dependency or biotin dependency that pediatricians recognized. The argument:
- Pellagra causes psychosis. Severe niacin deficiency reliably produces psychiatric symptoms identical to many schizophrenia presentations — auditory hallucinations, delusions, paranoia, disorganized thinking, catatonia. This is documented across the southern pellagra epidemic.
- Subclinical niacin deficiency might cause subclinical psychosis. If frank pellagra causes frank psychosis, perhaps subclinical niacin insufficiency (or impaired NAD+ synthesis from tryptophan) causes subclinical psychotic-spectrum symptoms in genetically susceptible individuals.
- Pharmacological-dose niacin might saturate any partial conversion defect by providing massive amounts of substrate, bypassing the rate-limiting enzyme.
- The kynurenine pathway connection. Schizophrenia patients have well-documented abnormalities in tryptophan metabolism — elevated kynurenic acid in CSF, altered IDO activity in inflammation. These abnormalities are biochemically connected to NAD+ synthesis.
The niacin-dependency hypothesis remains compatible with modern findings about kynurenine pathway dysregulation in schizophrenia, even if the original clinical claims of dramatic recovery rates have not been replicated in controlled trials.
Linus Pauling and the Naming of Orthomolecular Psychiatry
Linus Pauling, the only person to win two unshared Nobel Prizes (Chemistry 1954, Peace 1962), encountered Hoffer's work in the 1960s and was sufficiently impressed to publish a programmatic paper in Science in 1968 titled "Orthomolecular Psychiatry." Pauling argued:
- Mental illness frequently involves "abnormal molecular environments of the brain" — abnormal concentrations of substances normally present (vitamins, minerals, amino acids, neurotransmitter precursors)
- Treatment should aim to restore the "right molecules" to the right concentrations — hence "ortho-molecular"
- This is a category of medicine distinct from pharmacological psychiatry (which uses drugs not normally present in the body) and from psychotherapy
- The high-dose niacin work of Hoffer and Osmond was the founding example of this approach
Pauling's intellectual sponsorship gave the orthomolecular movement enormous credibility and institutional momentum through the 1970s, including the founding of the Linus Pauling Institute and an entire alternative-medicine journal infrastructure (Journal of Orthomolecular Medicine). Pauling himself became increasingly associated with high-dose vitamin C megadosing, which somewhat tarnished the broader orthomolecular brand when his cold and cancer claims for vitamin C did not survive rigorous trial replication.
The deeper insight of orthomolecular psychiatry — that nutritional status influences brain chemistry and that some psychiatric patients have correctable nutritional deficiencies — has been substantially validated. Folate deficiency depression, B12 deficiency psychosis, thiamine-related Korsakoff syndrome, pellagra psychosis, and B6-related epilepsy are all clinically recognized. The narrower claim — that gram-range niacin specifically cures schizophrenia — has not been validated in modern controlled trials.
The Niacin Flush Test — A Real Endophenotype
The niacin flush test is one of the most replicated biochemical findings in schizophrenia research. The basic observation:
- Healthy individuals reliably flush when exposed to nicotinic acid (orally or topically as a methyl nicotinate patch) — the GPR109A-mediated prostaglandin D2 vasodilation discussed in the cardiovascular-benefits page.
- Approximately 30-40% of schizophrenia patients show a reduced or absent flush response to standardized niacin/methyl-nicotinate challenge.
- The blunted flush is most pronounced in first-episode psychosis patients and in unaffected first-degree relatives at increased genetic risk — suggesting it is a trait marker (endophenotype), not a state marker or medication artifact.
- The effect is independent of antipsychotic medication status, smoking, age, and sex.
The mechanism is thought to involve abnormalities in arachidonic acid metabolism, prostaglandin D2 synthesis, or GPR109A receptor signaling in Langerhans cells — possibly tied to broader essential fatty acid abnormalities documented in schizophrenia (low membrane arachidonic acid, low DHA, altered phospholipase A2 activity).
The clinical implications:
- The niacin flush test is a candidate biomarker for stratifying schizophrenia patients into biological subtypes — the "flush-blunted subgroup" may represent a more biologically distinct population than the broader schizophrenia diagnosis
- It does NOT mean these patients are niacin-deficient or that niacin supplementation will treat their psychosis — the flush abnormality reflects altered prostaglandin signaling, not B3 status per se
- It does support the broader idea that schizophrenia is biochemically heterogeneous and that biological subtypes might respond to different interventions
Why Later Controlled Trials Disappointed
The 1960s and 1970s saw multiple attempts to replicate Hoffer and Osmond's dramatic schizophrenia results in larger and more rigorously controlled trials. Most were negative or marginally positive:
- The Wittenborn trials (1973-1974) — conducted at Rutgers, did not find significant niacin benefit over placebo in well-controlled schizophrenia samples.
- The Ban et al. trials (1971) — multicenter Canadian replication attempts, mixed results overall not supporting Hoffer's original effect sizes.
- The Greenbaum et al. and Petrie et al. studies of the early 1970s — negative or marginally positive.
Several reasons emerged for the divergence between Hoffer/Osmond's original positive results and the later negative trials:
- Selection bias. Hoffer and Osmond's original patient population may have included a higher proportion of patients with acute-onset, treatment-naive presentations — the demographic most likely to remit spontaneously regardless of treatment. Later trials in chronic, treatment-refractory populations had less room for any intervention to show benefit.
- The rise of antipsychotic drugs. By the late 1960s, chlorpromazine and other dopamine receptor antagonists were established as effective treatments. The comparison condition for niacin was no longer "no treatment" but "no treatment plus first-generation antipsychotics" — a much higher bar.
- Dose and form variability. Trials used different doses, different forms (nicotinic acid vs nicotinamide), different cotreatments (B-vitamins, vitamin C, zinc, with vs without).
- Endpoint differences. Hoffer's "recovery" criteria emphasized social functioning, work return, and family relationships rather than symptom rating scales. Later trials used standardized symptom scales (BPRS, PANSS) which captured different aspects of outcome.
- Possible biological subtype effect. If only a niacin-dependent subset of schizophrenia patients responds to high-dose niacin — perhaps 20-30% of the population — an unstratified trial may show modest aggregate benefit that doesn't reach significance, even though within-subset benefit could be large. Hoffer himself argued this point repeatedly.
The 1973 APA Task Force Verdict
In 1973 the American Psychiatric Association convened a task force to evaluate megavitamin and orthomolecular therapy in psychiatry. Their report was sharply critical of Hoffer and Osmond's clinical claims, concluding that the rigorous controlled trials did not support the original effect sizes and that orthomolecular psychiatry should not be considered established clinical practice.
Hoffer responded angrily that the task force had cherry-picked negative trials and ignored methodological flaws in those trials, and that the task force chair had pre-existing biases against the orthomolecular approach. The exchange remains a classic episode in the history of clinical-research politics, with arguments on both sides.
The practical effect: by 1980, mainstream academic psychiatry had largely abandoned megadose niacin therapy. The orthomolecular movement continued in alternative medicine and in patient-advocate communities (the International Schizophrenia Foundation, the Journal of Orthomolecular Medicine) but largely disappeared from mainstream psychiatric training and practice. Hoffer continued treating patients with his protocols until his death in 2009 at age 91, maintaining that his original results were real and reproducible in clinical practice even if they had not been replicated in randomized trials.
Modern psychiatric researchers occasionally revisit the orthomolecular hypothesis with newer tools — the niacin flush test endophenotype work, kynurenine pathway imaging, and the recent interest in inflammation-based subtypes of schizophrenia — but no recent randomized trial has supported a return to gram-range niacin as first-line schizophrenia treatment.
Pellagra Psychosis — The Genuine Niacin-Psychosis Link
Setting aside the schizophrenia-treatment debate, one robust fact is established: severe niacin deficiency reliably causes psychosis. The psychiatric manifestations of pellagra (see also Pellagra & Skin) include:
- Irritability and anxiety (early)
- Depression and apathy
- Insomnia and fatigue
- Confusion, disorientation, memory loss
- Hallucinations (auditory and visual)
- Delusions and paranoid ideation
- Disorganized speech and behavior
- Frank dementia in end-stage disease
This is not "schizophrenia-like" — it is clinically indistinguishable from acute psychotic episodes in many cases. Historical southern asylums in the early 20th century were full of pellagra-psychosis patients who would have recovered fully with niacin replacement, had the cause been recognized.
Modern clinical implication: any patient presenting with new-onset psychosis who has risk factors for niacin deficiency — chronic alcoholism, malabsorption, Crohn's disease, carcinoid syndrome, isoniazid therapy, Hartnup disease, severe malnutrition, anorexia nervosa — should receive an empirical trial of niacin replacement (along with full B-complex) as part of the initial workup. The improvement, if niacin deficiency is the cause, is often dramatic over 24-72 hours and confirms the diagnosis better than any laboratory test.
The Tryptophan-Kynurenine-Quinolinic Acid Axis
One area where orthomolecular intuitions have been substantially validated by modern research is the tryptophan-kynurenine pathway in psychiatry. The basic biochemistry:
- Tryptophan can be metabolized through the serotonin pathway (tryptophan → 5-HTP → serotonin → melatonin) or through the kynurenine pathway (tryptophan → kynurenine → multiple branches including the de novo NAD+ synthesis route)
- Roughly 95% of tryptophan normally goes through the kynurenine pathway; only ~5% goes through serotonin synthesis
- The first step of the kynurenine pathway is catalyzed by IDO (indoleamine 2,3-dioxygenase) in immune cells and tissues, and by TDO (tryptophan 2,3-dioxygenase) in liver
- IDO is strongly induced by inflammatory cytokines — particularly interferon-gamma and TNF-α
In states of chronic inflammation (autoimmune disease, chronic infection, depression, schizophrenia), IDO induction shunts more tryptophan into the kynurenine pathway, with two consequences:
- Serotonin substrate depletion — less tryptophan available for serotonin synthesis, contributing to depression and sleep disturbance
- Accumulation of quinolinic acid — a downstream kynurenine metabolite that is a potent NMDA receptor agonist and neurotoxin, implicated in depression severity, suicidality, HIV-associated dementia, and possibly schizophrenia symptom severity
This is the modern biochemical basis for the "inflammatory hypothesis of depression" that has gained substantial empirical support over the past 20 years. The Hoffer/Pauling orthomolecular intuition — that abnormal tryptophan metabolism contributes to psychiatric disease — was directionally correct, even if the specific adrenochrome mechanism they proposed was not. Niacin supplementation in this context might reduce IDO induction (because adequate NAD+ provides feedback inhibition on the de novo pathway) and reduce quinolinic acid accumulation — though this is mechanistically plausible rather than rigorously demonstrated.
See Tryptophan for the broader tryptophan biochemistry.
Niacin in OCD, Anxiety, and Depression
Beyond schizophrenia, integrative and orthomolecular practitioners have used high-dose nicotinamide for other psychiatric indications. The evidence is weaker than for schizophrenia (which is itself contested) but the clinical rationale is:
Anxiety
- Benzodiazepine receptor interaction. Nicotinamide binds with low affinity to the benzodiazepine recognition site on the GABA-A receptor, producing modest anxiolytic effects without the addiction or sedation profile of true benzodiazepines.
- Typical orthomolecular protocols use 500-3000 mg/day of nicotinamide in divided doses for generalized anxiety, panic disorder, and situational anxiety.
- Modern controlled trial evidence is sparse; effect sizes appear modest at best.
OCD (Obsessive-Compulsive Disorder)
- Some orthomolecular protocols include nicotinamide 1000-3000 mg/day plus inositol and NAC for OCD.
- NAC and inositol have more controlled-trial support for OCD than nicotinamide.
- The rationale for nicotinamide is neurotransmitter modulation and possible glutamate/NMDA effects.
- See OCD for the broader integrative approach.
Depression
- Tryptophan-substrate preservation. When B3 status is adequate, less tryptophan needs to be diverted toward NAD+ synthesis, preserving substrate for serotonin production.
- Kynurenine pathway modulation. Adequate NAD+ feedback inhibits the de novo pathway, potentially reducing quinolinic acid accumulation in inflammatory depression.
- Insomnia component. Nicotinamide 1000-3000 mg at bedtime has been reported anecdotally to improve sleep onset and quality in depressed patients — possibly via benzodiazepine-receptor binding or via supporting melatonin synthesis (which requires serotonin, which requires preserved tryptophan).
- Controlled trial evidence is weak; B3 should be considered an adjunct to standard depression care, not a replacement for evidence-based interventions.
Cognitive aging and Alzheimer's disease
- Higher dietary niacin intake has been associated with reduced Alzheimer's disease risk in the Chicago Health and Aging Project cohort and other epidemiological studies.
- NAD+ decline is implicated in neurodegeneration — see NAD+ Precursor for the broader story.
- NAD+ precursor trials in mild cognitive impairment are ongoing but currently lack definitive outcomes data.
The Realistic Modern Place of High-Dose B3
Synthesizing the historical record with modern evidence:
- NOT a replacement for evidence-based psychiatric treatment. Schizophrenia, bipolar disorder, severe depression, and OCD require evidence-based treatment with appropriate antipsychotic, mood-stabilizer, antidepressant, or SSRI/SRI therapy plus psychotherapy. Substituting niacin for these treatments is dangerous and irresponsible.
- YES for empirical pellagra workup. Any new-onset psychosis in a patient with niacin-deficiency risk factors deserves an empirical niacin trial as part of the standard workup — cheap, safe, occasionally curative.
- YES as adjunctive support in many integrative-medicine protocols, particularly when patients have documented poor diet quality, malabsorption, or biochemical evidence of tryptophan pathway dysregulation. The risk-benefit at conservative doses (500-1000 mg/day NAM) is favorable.
- POSSIBLY for the flush-blunted schizophrenia subtype as a biomarker-guided clinical research direction — not as established treatment but as a hypothesis worth testing in modern stratified-trial designs.
- NOT at the multi-gram doses Hoffer used without active monitoring — gram-range nicotinamide carries hepatotoxicity risk and sirtuin product-inhibition concerns; gram-range nicotinic acid carries hepatotoxicity, glucose, gout, and ulcer risks.
For practical psychiatric use, a defensible orthomolecular-influenced protocol is:
- Nicotinamide 500-1000 mg/day (split into 2 doses with meals) as an adjunct to standard psychiatric care
- Co-administer a complete B-complex including B1, B2, B6, B12, folate
- Monitor liver enzymes if dose escalation is considered
- Combine with omega-3 fatty acids (EPA/DHA), magnesium glycinate, and zinc as the broader nutritional foundation
- Document any subjective or objective response after 8-12 weeks
- Discontinue if no benefit, no harm done; continue if benefit is durable
Cautions
- HEPATOTOXICITY — sustained-release nicotinic acid at >1 g/day. The same warning as for cardiovascular use applies in psychiatric protocols. If gram-range nicotinic acid is used, it MUST be immediate-release with liver enzyme monitoring at baseline, 6 weeks, 3 months, and then every 6 months. Discontinue at ALT > 3x ULN. Sustained-release at gram-range doses has caused fulminant hepatic failure.
- Sirtuin product inhibition — high-dose nicotinamide. Sustained NAM above 3000 mg/day can inhibit sirtuin enzymes (NAM is a product-feedback inhibitor of sirtuin reactions) — the opposite of the desired metabolic-support effect. Cap chronic NAM use at 2000 mg/day for psychiatric protocols.
- Drug interactions in psychiatric patients. Many antipsychotic medications (clozapine in particular) carry hepatotoxicity and metabolic risks of their own. Combining high-dose niacin with clozapine, olanzapine, or valproic acid adds liver and metabolic risk that requires careful monitoring.
- Hyperglycemia. Nicotinic acid raises blood glucose; many psychiatric patients are already at metabolic risk from atypical antipsychotic medications. Monitor glucose and HbA1c.
- Do not substitute for evidence-based treatment. A psychotic episode or severe depression requires standard psychiatric care. Using niacin as primary treatment for an acute psychotic break is dangerous — ineffective treatment may allow patient deterioration to a point requiring more aggressive intervention or hospitalization.
- Methylation concerns. Some integrative practitioners worry about gram-range nicotinamide depleting methyl groups (through N1-methylnicotinamide excretion) and stressing methylation-dependent functions (homocysteine, neurotransmitter synthesis, DNA methylation). At doses up to 1-2 g/day this concern is usually overstated, but co-supplementation with methylfolate, methylcobalamin, and TMG (trimethylglycine) is reasonable in patients with MTHFR variants.
- Suicidality screening. Patients with major depression, OCD, or schizophrenia require ongoing suicidality assessment regardless of niacin status. The orthomolecular community has occasionally minimized this need; modern integrative practice does not.
- Flush in nicotinic acid users. The vasodilatory flush can be alarming in anxious patients. Pre-counsel thoroughly; consider NAM instead of nicotinic acid for psychiatric indications where lipid effects are not needed.
Key Research Papers
- Hoffer A, Osmond H, Smythies J (1954). Schizophrenia: a new approach. II. Result of a year's research. J Ment Sci. — PubMed
- Hoffer A (1971). Megavitamin B-3 therapy for schizophrenia. Can Psychiatr Assoc J. — PubMed
- Pauling L (1968). Orthomolecular psychiatry. Science. — PubMed
- APA Task Force (1973). Megavitamin and orthomolecular therapy in psychiatry. American Psychiatric Association. — PubMed
- Niacin flush test in schizophrenia — PubMed
- Hudson C et al. on the niacin skin flush response as a schizophrenia endophenotype — PubMed
- Wittenborn JR et al. (1973). Niacin in the long-term treatment of schizophrenia. Arch Gen Psychiatry. — PubMed
- Tryptophan-kynurenine pathway in depression — PubMed
- Quinolinic acid in schizophrenia and depression — PubMed
- Niacin and Alzheimer's disease (Chicago Health and Aging Project) — PubMed
- Niacinamide and anxiety / benzodiazepine receptor binding — PubMed
- Pellagra psychosis case series — PubMed
- IDO induction by interferon and inflammation in psychiatric disease — PubMed
PubMed Topic Searches
- PubMed: orthomolecular psychiatry niacin
- PubMed: niacin schizophrenia
- PubMed: niacin flush endophenotype
- PubMed: kynurenine psychiatric
- PubMed: Hoffer Osmond Saskatchewan
- PubMed: nicotinamide psychiatric adjunct
Connections
- Vitamin B3 Overview
- B3 Benefits Hub
- B3 as NAD+ Precursor
- B3 for Cholesterol & Cardiovascular
- B3 for Pellagra & Skin
- Pellagra & Niacin Deficiency
- Schizophrenia
- OCD
- Depression
- Anxiety
- Dementia
- Alzheimer's Disease
- Tryptophan
- Niacin in Gerson Therapy
- NAD+ / NMN
- Vitamin B6 (Pyridoxine)
- Vitamin B12
- All Vitamins