Niacin for Pellagra and Skin Health
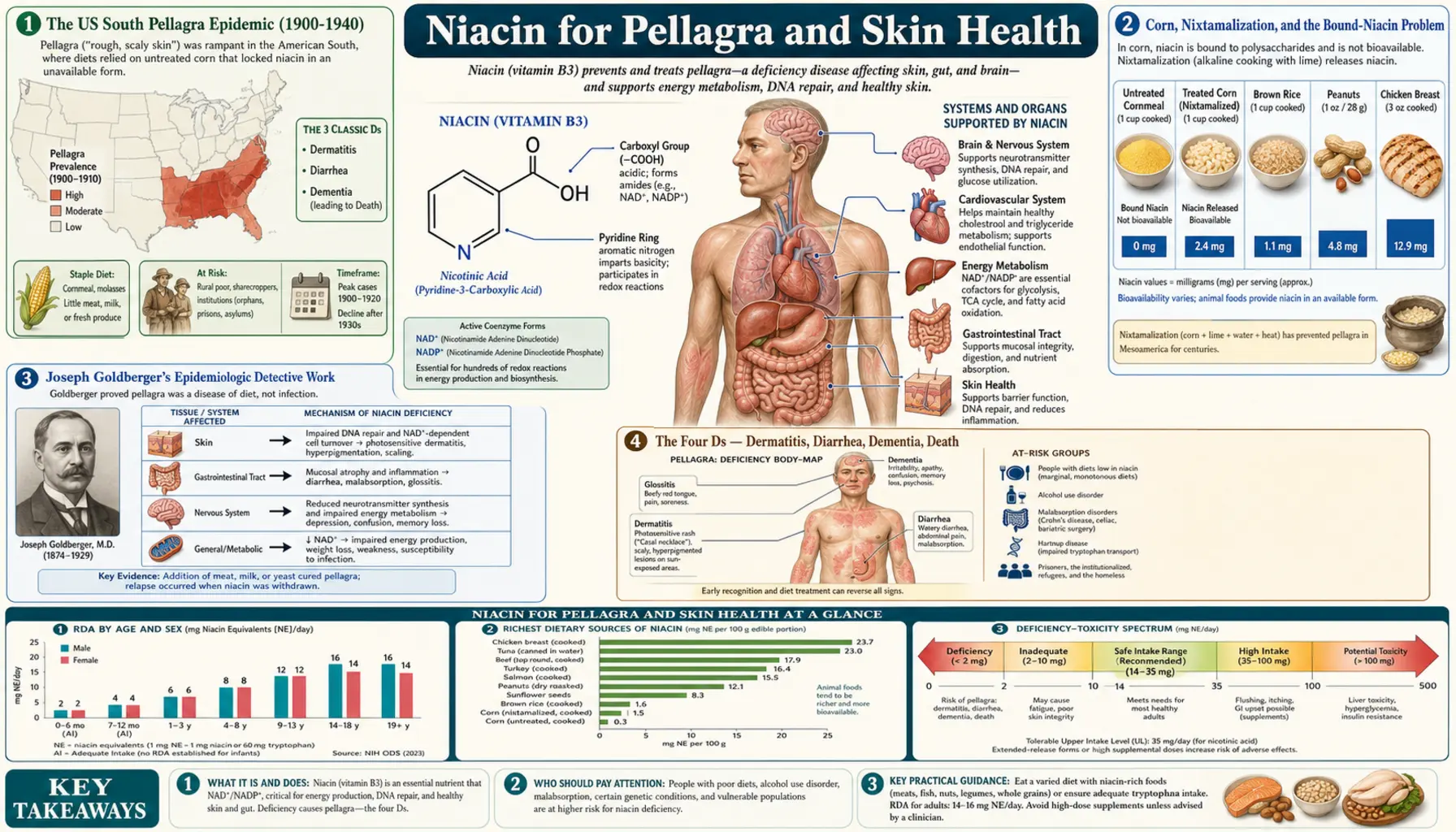
Pellagra was the largest nutritional-deficiency epidemic in US history. Between 1900 and 1940 it killed an estimated 100,000 Americans, mostly in the rural South, where a corn-based diet without nixtamalization left bound niacytin biologically inaccessible. Joseph Goldberger's brilliant 1914-1929 epidemiologic work proved pellagra was a dietary deficiency rather than an infection — against fierce political opposition — and his work led to the eventual discovery of niacin in 1937. Today, frank pellagra is rare in developed countries but hidden pellagra still appears in chronic alcoholism, Crohn's disease, carcinoid syndrome, isoniazid therapy, and Hartnup disease. Meanwhile, topical and oral niacinamide have become workhorse ingredients in modern dermatology, with the landmark ONTRAC trial showing 23% reduction in non-melanoma skin cancers at 500 mg twice daily.
Table of Contents
- The US South Pellagra Epidemic (1900-1940)
- Corn, Nixtamalization, and the Bound-Niacin Problem
- Joseph Goldberger's Epidemiologic Detective Work
- The Four Ds — Dermatitis, Diarrhea, Dementia, Death
- Casal's Necklace and the Pellagra Dermatitis Pattern
- Hidden Modern Pellagra — Alcoholism, Crohn's, Hartnup
- Secondary Pellagra — Carcinoid, Isoniazid, HIV
- Topical Niacinamide for Acne and Barrier Function
- Niacinamide for Hyperpigmentation
- The ONTRAC Trial — Skin Cancer Chemoprevention
- Niacinamide as a Skincare Ingredient (5-10%)
- Pellagra Treatment Protocol
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The US South Pellagra Epidemic (1900-1940)
Pellagra was first formally described in Spain by Gaspar Casal in 1735 (he called it "mal de la rosa" after the characteristic skin rash) and then in Italy in 1771 by Francesco Frapolli, who coined the name "pelle agra" — rough skin. For a century and a half, European pellagra remained largely confined to peasant populations in northern Italy and Spain dependent on corn-based polenta and tortas.
The American epidemic exploded between 1900 and 1940. By the 1910s pellagra was killing an estimated 6,000-7,000 Americans per year, with case counts in the tens of thousands. The geographic concentration was striking:
- South Carolina: over 30,000 cases reported in 1915 alone
- Mississippi, Alabama, Georgia, Tennessee: tens of thousands of cases through the 1920s-1930s
- Demographic concentration: impoverished tenant farmers, textile mill workers, prison populations, and orphanage residents — populations dependent on the "three M" diet of meal (cornmeal), meat (salt pork fat), and molasses
- Total US death toll: approximately 100,000 deaths from pellagra over the four decades of the epidemic, with many more suffering chronic disability
The cause was the rise of mechanized corn milling that removed the germ and bran, combined with the southern post-Reconstruction tenant-farming economy that left rural families dependent on cornmeal as the dominant staple. Unlike traditional Mesoamerican corn preparation (see next section), industrially milled American cornmeal was never alkali-treated — the niacin in the corn remained bound and biologically inaccessible.
Corn, Nixtamalization, and the Bound-Niacin Problem
Corn (maize) contains modest amounts of niacin — roughly 1.5 mg per 100 g of cornmeal — but almost all of it is in a chemically bound form called niacytin, in which nicotinic acid is covalently linked to peptides and polysaccharides in the grain matrix. Niacytin is not hydrolyzed by digestive enzymes and is therefore biologically inaccessible. The "niacin content" measured by laboratory assay drastically overstates what the body can actually use.
The traditional Mesoamerican solution — developed independently by Maya, Aztec, and other indigenous cultures over thousands of years — is nixtamalization:
- Soak dried corn kernels in an alkaline solution — traditionally lime water (calcium hydroxide, CaOH2) or wood ash lye, overnight or for several hours
- Rinse and grind into masa for tortillas, tamales, atole, or pozole
The alkaline treatment hydrolyzes the niacytin peptide bonds and releases bioavailable free nicotinic acid. It also improves the calcium content (the lime provides calcium), improves amino acid balance (frees up bound tryptophan), and softens the corn kernels for grinding. Cultures that consumed nixtamalized corn — the Maya, the Aztec, traditional Mexican and Central American populations — did not develop pellagra despite corn-dominated diets.
When Europeans adopted corn from the Americas in the 16th century, they took the crop but not the nixtamalization technique. Italian polenta, Spanish gachas, and eventually southern US cornmeal were all prepared without alkali treatment. The result: a thousand-year nutritional accident that caused pellagra epidemics on three continents.
The lesson generalizes: traditional food preparation methods often carry crucial nutritional information that pure ingredient analysis misses. The chemistry of niacytin hydrolysis was not understood until the 1940s, but the Maya solved the problem empirically by 1500 BCE.
Joseph Goldberger's Epidemiologic Detective Work
Joseph Goldberger was a Hungarian-born physician working at the US Public Health Service when he was assigned in 1914 to investigate the southern pellagra epidemic. The dominant medical hypothesis was that pellagra was an infectious disease — spread by mold contamination of corn (the "Zeist theory") or by an unknown insect vector. Goldberger's epidemiologic observations rapidly demolished both hypotheses:
- Goldberger's institutional observations. In orphanages, mental hospitals, and prisons where pellagra raged among inmates, the staff who worked in the same buildings and breathed the same air did not get pellagra — but they ate from different kitchens. The staff diets included fresh meat, milk, and eggs. The inmate diets were primarily cornmeal and salt pork.
- The Mississippi orphanage experiment (1914-1915). Goldberger arranged to add fresh milk, eggs, meat, and legumes to the diet of two orphanages with high pellagra rates. Within months, active pellagra disappeared from both institutions.
- The Rankin Prison Farm experiment (1915). Goldberger persuaded the Mississippi governor to commute the sentences of 11 prison volunteers in exchange for being deliberately fed the "three M" pellagra diet (cornmeal, salt pork, molasses, no fresh foods). After 5-6 months, 6 of the 11 prisoners developed unmistakable clinical pellagra. The "controls" eating a normal mixed diet remained healthy. The experiment definitively proved pellagra was a dietary deficiency.
- The "filth parties" (1916). To refute the infection hypothesis, Goldberger, his wife, and colleagues deliberately ingested capsules containing scabs, urine, feces, and nasal secretions from active pellagra patients. None developed pellagra. The infectious hypothesis was untenable.
- The seven textile mill communities study (1916-1918). Goldberger documented that pellagra incidence in cotton-mill villages correlated with household economic stress (which determined diet quality), not with infection vectors. Higher income meant access to fresh meat and dairy and lower pellagra rates.
Despite this overwhelming evidence, Southern politicians, agricultural interests, and traditionalists in medicine resisted Goldberger's conclusions because they implicated rural poverty and the southern economy. Goldberger published the seven-mill study in Public Health Reports in 1923 and continued working on pellagra until his death from cancer in 1929 — eight years before Conrad Elvehjem and colleagues finally isolated and identified nicotinic acid as the missing factor (1937, University of Wisconsin), and 14 years before flour fortification with niacin became national policy in 1942.
Goldberger never knew exactly what was missing from the southern diet, but he knew with certainty that it was something in fresh meat, eggs, and milk — and he had the moral courage to deliberately ingest pellagra patient secretions to disprove the infection hypothesis when politics tried to shame him into silence. The story is a classic in scientific epidemiology and political courage.
The Four Ds — Dermatitis, Diarrhea, Dementia, Death
The mnemonic "the four Ds" captures the natural history of untreated pellagra:
- Dermatitis — bilateral, symmetrical, photosensitive skin rash that begins as erythema on sun-exposed areas (face, neck, back of hands, dorsum of feet) and progresses through vesiculation, hyperpigmentation, thickening, scaling, and eventual cracking and ulceration. The rash is dramatic and pathognomonic. Casal's necklace (see next section) is the classic presentation.
- Diarrhea — inflammation of the entire GI tract: glossitis (smooth, painful, beefy-red tongue), angular stomatitis, esophagitis, gastritis, profuse watery diarrhea, and progressive malabsorption that worsens the underlying deficiency.
- Dementia — progressive neurological and psychiatric deterioration: irritability, anxiety, insomnia, then depression and apathy, then confusion, disorientation, hallucinations, delusions, and full-blown psychosis. The "pellagra psychosis" historically filled southern asylums in the early 20th century. End-stage pellagra produces severe dementia indistinguishable from late Alzheimer's disease.
- Death — without treatment, pellagra is fatal. Death typically follows from secondary infection in malnourished, immunocompromised patients with broken skin and severe malabsorption, or from cardiovascular collapse, or from accidents and suicide during the psychotic phase.
With niacin repletion, the symptoms reverse in a predictable order: psychiatric symptoms improve first (within 24-48 hours), then GI symptoms (over 1-2 weeks), then dermatitis (over weeks to months, with hyperpigmentation sometimes persisting). If treatment is delayed until end-stage dementia is established, some neurological damage may be irreversible.
Casal's Necklace and the Pellagra Dermatitis Pattern
Gaspar Casal, the 18th-century Spanish physician who first described pellagra, drew careful clinical illustrations of a band-like dermatitis around the neck — the rash extends down across the upper chest in the V-shape of an open-collared shirt, sparing the covered skin. This collar-line dermatitis became known as Casal's necklace (collar of Casal) and remains a pathognomonic finding.
The pattern reflects photosensitive damage. The pellagra rash appears specifically where:
- Skin is exposed to sunlight (UV-B in particular)
- Niacin/NAD+ deficiency impairs the cellular DNA-repair response to UV damage
- The skin's barrier function (which depends on NAD+-supported ceramide synthesis) is already compromised
Other classical pellagra dermatitis patterns:
- "Glove" pattern: sharply demarcated rash on the dorsum of the hands extending up to the wrist, sparing skin under long sleeves
- "Boot" pattern: similar pattern on the dorsum of the feet and ankles extending up to where socks or trouser cuffs covered the skin
- "Butterfly" pattern: across the bridge of the nose and cheeks (can resemble lupus malar rash, but pellagra extends to include the upper chest in Casal's necklace pattern, which lupus rarely does)
- "Goose foot" pattern (Patte d'oie): the rash on the back of the neck running into wrinkle lines
The bilateral symmetry and sharp demarcation along sun-exposure lines are highly characteristic. A photosensitive dermatitis in an alcoholic, a Crohn's patient, or anyone on isoniazid should always trigger consideration of pellagra.
Hidden Modern Pellagra — Alcoholism, Crohn's, Hartnup
Frank textbook pellagra is now rare in developed countries because of flour fortification with niacin (mandated in the US since 1942) and generally adequate protein intake. But hidden or subclinical pellagra still occurs and is frequently missed because clinicians no longer consider it.
Chronic alcoholism
The most common modern cause. Alcohol contributes multiple hits: (1) alcohol metabolism by alcohol dehydrogenase and aldehyde dehydrogenase consumes massive amounts of NAD+ in the liver, depleting hepatic stores; (2) chronic alcoholics frequently have poor diet quality with low protein and B-vitamin intake; (3) alcohol impairs intestinal absorption of multiple B vitamins; (4) alcoholic liver disease impairs the Preiss-Handler conversion of nicotinic acid to NAD+. Alcoholics frequently present with partial pellagra — photosensitive dermatitis, glossitis, irritability, and confusion that's attributed to alcohol itself rather than to niacin deficiency. Broad B-complex replacement (including pellagra-level niacin doses) should be standard in any malnourished alcoholic.
Crohn's disease and IBD
Active small-bowel Crohn's disease causes malabsorption of all B vitamins. Chronic intestinal inflammation also induces IDO (indoleamine 2,3-dioxygenase) which diverts tryptophan away from NAD+ synthesis toward kynurenine pathway metabolites. The combination of malabsorption plus increased tryptophan catabolism can produce secondary pellagra in poorly nourished Crohn's patients. Watch especially for combined photosensitive dermatitis and worsening cognitive symptoms in a Crohn's patient.
Hartnup disease
A rare autosomal recessive disorder caused by SLC6A19 gene mutations affecting the neutral amino acid transporter in the intestine and renal tubules. Patients cannot adequately absorb tryptophan from the gut or reabsorb it in the kidneys. Clinical presentation includes a pellagra-like photosensitive rash, episodic cerebellar ataxia, and psychiatric symptoms — usually presenting in childhood and triggered by sunlight exposure, fever, or stress. Treatment is high-dose nicotinamide (50-300 mg/day) plus a high-protein diet. Symptoms usually resolve completely with treatment though episodes can recur during stress.
Secondary Pellagra — Carcinoid, Isoniazid, HIV
Carcinoid syndrome
Serotonin-producing carcinoid tumors (originating from enterochromaffin cells, typically in the small intestine, appendix, or bronchus) divert up to 60% of dietary tryptophan into serotonin synthesis, depleting the substrate pool available for NAD+ biosynthesis. Pellagra is a classical late-stage carcinoid syndrome finding (alongside flushing, diarrhea, and right-sided valvular heart disease). Treatment requires both tumor control and high-dose niacin replacement.
Isoniazid (INH)
The tuberculosis drug isoniazid is a pyridoxine (B6) antagonist — it forms a covalent adduct with B6 and depletes the active cofactor. B6 is required for kynureninase in the de novo NAD+ synthesis pathway. INH-treated patients develop secondary pellagra-like symptoms (rash, neuropathy, psychiatric symptoms) that respond to combined B6 and niacin supplementation. Standard practice is to co-prescribe 25-50 mg/day pyridoxine with any isoniazid regimen.
HIV/AIDS
Chronic HIV infection induces sustained IDO expression in macrophages and dendritic cells, dramatically increasing tryptophan catabolism into the kynurenine pathway — producing neurotoxic quinolinic acid and depleting the substrate available for serotonin synthesis. The clinical manifestation includes pellagra-like dermatitis, neuropsychiatric symptoms (HIV-associated dementia), and depression. Niacin supplementation helps but does not fully reverse the underlying tryptophan diversion.
Other causes
- Anorexia nervosa and severe protein-calorie malnutrition
- Bariatric surgery (especially gastric bypass — reduced absorption surface)
- Prolonged parenteral nutrition without adequate niacin
- Drug-induced: 5-fluorouracil, 6-mercaptopurine, chloramphenicol
- Tryptophan-poor diets in some extreme vegan patterns without adequate planning
Topical Niacinamide for Acne and Barrier Function
Topical nicotinamide (niacinamide) has become one of the most widely used active ingredients in modern dermatology, supported by substantial clinical trial evidence:
Acne vulgaris
- 4% topical niacinamide gel has been compared head-to-head with 1% clindamycin gel and produced equivalent reductions in inflammatory acne lesion counts at 8 weeks — without contributing to antibiotic resistance and without disrupting the skin microbiome the way topical antibiotics do.
- Mechanisms include inhibition of inflammatory cytokine release (IL-1, IL-8, TNF-α), suppression of leukocyte chemotaxis to lesions, and reduction of sebum production.
- Niacinamide is particularly useful in inflammatory adult acne and rosacea where antibiotic stewardship is a concern.
Skin barrier function
- Niacinamide upregulates the synthesis of ceramides (especially ceramide 3), free fatty acids, and cholesterol — the three lipid components of the stratum corneum lamellae that constitute the skin barrier.
- Topical 2-5% niacinamide reduces transepidermal water loss (TEWL), improves stratum corneum hydration, and helps repair barrier function in atopic dermatitis, rosacea, and post-procedure skin.
- The mechanism is partly NAD+-dependent — ceramide synthesis requires sphingolipid pathway enzymes that depend on NAD/NADP cofactors.
Rosacea
Topical niacinamide 2% significantly reduces erythema and improves barrier function in rosacea, sometimes used as a steroid-sparing alternative or adjunct to azelaic acid and metronidazole.
Atopic dermatitis
Niacinamide in emollients reduces flare frequency and improves barrier function in pediatric and adult atopic dermatitis, often allowing reduced topical steroid use.
Niacinamide for Hyperpigmentation
Niacinamide reduces hyperpigmentation (melasma, post-inflammatory hyperpigmentation, age spots) through a mechanism distinct from hydroquinone or arbutin:
- Niacinamide does NOT inhibit tyrosinase (the rate-limiting enzyme of melanin synthesis) — melanin production itself is unaffected.
- Instead, niacinamide inhibits the transfer of melanosomes (pigment-containing organelles) from melanocytes to surrounding keratinocytes. The keratinocyte receives less pigment cargo.
- The effect is reversible and gentler than tyrosinase inhibitors — less risk of paradoxical post-inflammatory hyperpigmentation, no risk of exogenous ochronosis (which can occur with hydroquinone).
Topical niacinamide 4-5% over 8-12 weeks produces measurable reductions in melasma and post-inflammatory hyperpigmentation in clinical trials — not as dramatic as hydroquinone but with a much safer long-term profile, and effective in combination with sunscreen and azelaic acid in melasma protocols.
The ONTRAC Trial — Skin Cancer Chemoprevention
The ONTRAC trial (Oral Nicotinamide to Reduce Actinic Cancer), published by Chen et al. in the New England Journal of Medicine in 2015, is the landmark study establishing oral nicotinamide as evidence-based skin cancer chemoprevention.
Design
- 386 patients in Australia who had had at least two non-melanoma skin cancers (basal cell or squamous cell carcinoma) in the previous 5 years — a high-risk population
- Randomized to nicotinamide 500 mg twice daily or placebo
- 12 months of treatment
- Primary endpoint: number of new non-melanoma skin cancers
Results
- 23% reduction in new non-melanoma skin cancers (rate ratio 0.77, p = 0.02)
- 20% reduction in BCC, 30% reduction in SCC
- 11% reduction in actinic keratoses (precancerous lesions) at 3 months, rising to 20% at 12 months
- No serious adverse events; nicotinamide was as well-tolerated as placebo
- The benefit disappeared rapidly after discontinuation, indicating continuous use is required
Mechanism
UV radiation damages DNA via thymine dimer formation, depletes cellular NAD+ as PARPs are activated to repair the damage, and suppresses local immune surveillance (the "UV immunosuppression" that allows precancerous cells to escape destruction). Nicotinamide:
- Replenishes cellular NAD+, supporting continued PARP-mediated DNA repair after UV damage
- Provides energy for the ATP-dependent nucleotide excision repair pathway that removes thymine dimers
- Prevents UV-induced immunosuppression, allowing the immune system to clear damaged cells
Clinical implications
Oral nicotinamide 500 mg twice daily is now widely recommended by dermatologists for patients at high risk of non-melanoma skin cancer — particularly fair-skinned patients with extensive actinic damage, organ transplant recipients on immunosuppression, and patients with prior multiple BCCs or SCCs. The dose is well-tolerated, cheap (a few dollars per month), and the only common side effect is mild headache during the first week. Sustained use is required for sustained benefit.
Niacinamide as a Skincare Ingredient (5-10%)
Niacinamide has become a workhorse ingredient in modern skincare formulations, appearing in serums, moisturizers, sunscreens, and treatment products from drugstore through luxury brands:
- 2-5% concentration is the typical "general purpose" range — barrier support, mild brightening, anti-inflammatory effects, suitable for daily use including sensitive skin
- 5-10% concentration is the "active treatment" range — more pronounced effects on hyperpigmentation, acne, and pore size; some users experience mild irritation at this level requiring gradual introduction
- Above 10% rarely adds benefit and increases irritation risk; well-formulated 10% products at appropriate pH (slightly acidic) are usually the practical ceiling
Formulation considerations
- Stability: niacinamide is stable in a wide pH range and tolerates most other actives well. Unlike vitamin C, it does not require special anti-oxidant packaging.
- Combining with vitamin C: the old concern that niacinamide and ascorbic acid form niacin (the flush-causing form) only matters at very high temperatures and concentrations. At skincare-product concentrations and skin temperature, they are compatible. Modern dermatology generally considers them safe to use together or in sequence.
- Combining with retinoids: niacinamide reduces retinoid-induced barrier disruption and irritation, making it an excellent buffer ingredient in retinol/tretinoin routines.
- Combining with alpha-hydroxy acids and salicylic acid: generally well-tolerated; if irritation occurs, separate by time of day (acids morning, niacinamide evening).
Pellagra Treatment Protocol
For confirmed or strongly suspected pellagra (history, clinical picture, response to treatment):
Acute phase
- Nicotinamide 300-500 mg/day in 3 divided doses (use NAM not nicotinic acid — avoid the flush in an already-distressed patient; in severe cases injectable nicotinamide can be used)
- Co-administer a complete B-complex including B1 (thiamine, 100 mg/day — critical in alcoholics, MUST give before any carbohydrate refeeding to prevent Wernicke's encephalopathy), B2, B6, B12, folate
- Protein-rich diet as tolerated to provide tryptophan substrate (eggs, dairy, meat if available)
- Address underlying cause: alcohol cessation, Crohn's disease management, isoniazid co-prescription of B6, carcinoid tumor workup, etc.
Expected response
- 24-48 hours: psychiatric symptoms begin to improve — reduced confusion, better orientation, calmer affect
- 3-7 days: GI symptoms (diarrhea, glossitis) improve substantially
- Weeks to months: dermatitis resolves; hyperpigmentation may persist longer
- If no improvement in 1 week: reconsider the diagnosis or look for ongoing causative factors
Maintenance and prevention
- Long-term nicotinamide 100-300 mg/day plus B-complex in patients with permanent risk factors (chronic alcoholism, IBD, Hartnup disease, carcinoid syndrome on chronic INH therapy)
- Sustained dietary improvement and protein adequacy
- Address the root cause (sobriety, IBD remission, etc.) to allow eventual discontinuation when safe
For Hartnup disease specifically, lifelong nicotinamide 50-300 mg/day (titrated to symptom control) plus a high-protein diet is the standard approach. Most patients have a normal life expectancy with treatment.
Cautions
- HEPATOTOXICITY — sustained-release nicotinic acid at >1 g/day. Even in pellagra treatment, do not use SR-niacin at gram-range doses. Use immediate-release nicotinic acid, or preferably nicotinamide (NAM) which does not cause flushing and has minimal hepatotoxicity at typical doses.
- Wernicke's encephalopathy precaution in alcoholics. Always give thiamine 100 mg IV or IM BEFORE any glucose, carbohydrate refeeding, or even niacin in a malnourished alcoholic. Thiamine-deficient brain tissue can develop irreversible Wernicke's encephalopathy when carbohydrate metabolism is suddenly resumed without B1.
- Carcinoid syndrome work-up first. If you discover unexplained pellagra in an adult without alcohol or malabsorption, consider carcinoid syndrome — check serum chromogranin A, 24-hour urinary 5-HIAA. Niacin replacement is necessary but doesn't address the underlying tumor.
- Sustained NAM > 3 g/day. Chronic very-high-dose nicotinamide can cause sirtuin product inhibition and theoretical hepatotoxicity. Cap routine NAM use at 2 g/day; reserve higher doses for short-term pellagra treatment under monitoring.
- Topical niacinamide irritation. At concentrations > 5% some users experience mild stinging, redness, or flushing-like erythema (separate from the GPR109A flush of oral nicotinic acid). Introduce gradually; if irritation persists, drop to a lower concentration.
- Drug interactions: isoniazid (need B6 co-supplementation as noted); 5-fluorouracil and chemotherapy (consult oncology before adding high-dose NAM); levodopa (modest interaction).
- Diagnostic ambiguity. Photosensitive dermatitis in the modern era is more often lupus, drug photosensitivity, or porphyria than pellagra. A skin biopsy may be needed; an empirical trial of niacin replacement is often diagnostic if response is dramatic.
Key Research Papers
- Goldberger J et al. (1923). A study of the relation of diet to pellagra incidence in seven textile-mill communities of South Carolina. Public Health Reports. — PubMed
- Goldberger J, Wheeler GA (1915). Experimental pellagra in the human subject brought about by a restricted diet. Public Health Reports. — PubMed
- Elvehjem CA et al. (1937). Relation of nicotinic acid and nicotinic acid amide to canine black tongue. J Am Chem Soc. — PubMed
- Chen AC et al. (2015). A phase 3 randomized trial of nicotinamide for skin-cancer chemoprevention (ONTRAC). NEJM. — PubMed
- Hegyi J et al. (2004). Pellagra: dermatitis, dementia, and diarrhea. Int J Dermatol. — PubMed
- Wan P et al. on Hartnup disease and SLC6A19 — PubMed
- Topical niacinamide 4% vs clindamycin 1% for acne — PubMed
- Niacinamide and ceramide synthesis / barrier function — PubMed
- Niacinamide melanosome transfer inhibition / hyperpigmentation — PubMed
- Crohn's disease and secondary pellagra — PubMed
- Alcoholism and pellagra — PubMed
- Carcinoid syndrome and tryptophan diversion / pellagra — PubMed
- Isoniazid-induced pellagra — PubMed
PubMed Topic Searches
- PubMed: pellagra niacin deficiency
- PubMed: topical niacinamide dermatology
- PubMed: nicotinamide chemoprevention
- PubMed: nixtamalization niacin
- PubMed: Hartnup disease
Connections
- Vitamin B3 Overview
- B3 Benefits Hub
- B3 as NAD+ Precursor
- B3 for Cholesterol & Cardiovascular
- B3 for Schizophrenia & Mental Health
- Pellagra & Niacin Deficiency (Original Article)
- Tryptophan
- Niacin in Gerson Therapy
- Schizophrenia
- Dementia
- Vitamin B1 (Thiamine)
- Vitamin B6 (Pyridoxine)
- Vitamin B2 (Riboflavin)
- NAD+ / NMN
- All Vitamins