Niacin and Cholesterol Management
Niacin (vitamin B3) has a long and distinguished history in lipid management, dating back to the 1950s when it became the first lipid-lowering agent shown to reduce cardiovascular events. Despite the rise of statins and other modern therapies, niacin remains one of the most effective agents for raising HDL cholesterol and continues to occupy an important, if debated, role in cardiovascular medicine.
Table of Contents
- Key Benefits at a Glance
- NAD+ and NADP+ Biochemistry
- HDL-Raising Mechanism
- LDL and Triglyceride Reduction
- The GPR109A Receptor and Niacin Flush
- Extended-Release vs. Immediate-Release Niacin
- Major Clinical Trials
- Current Clinical Recommendations
- Comparison with Statins
- Monitoring and Safety Considerations
- Research Papers
- Connections
- Featured Videos
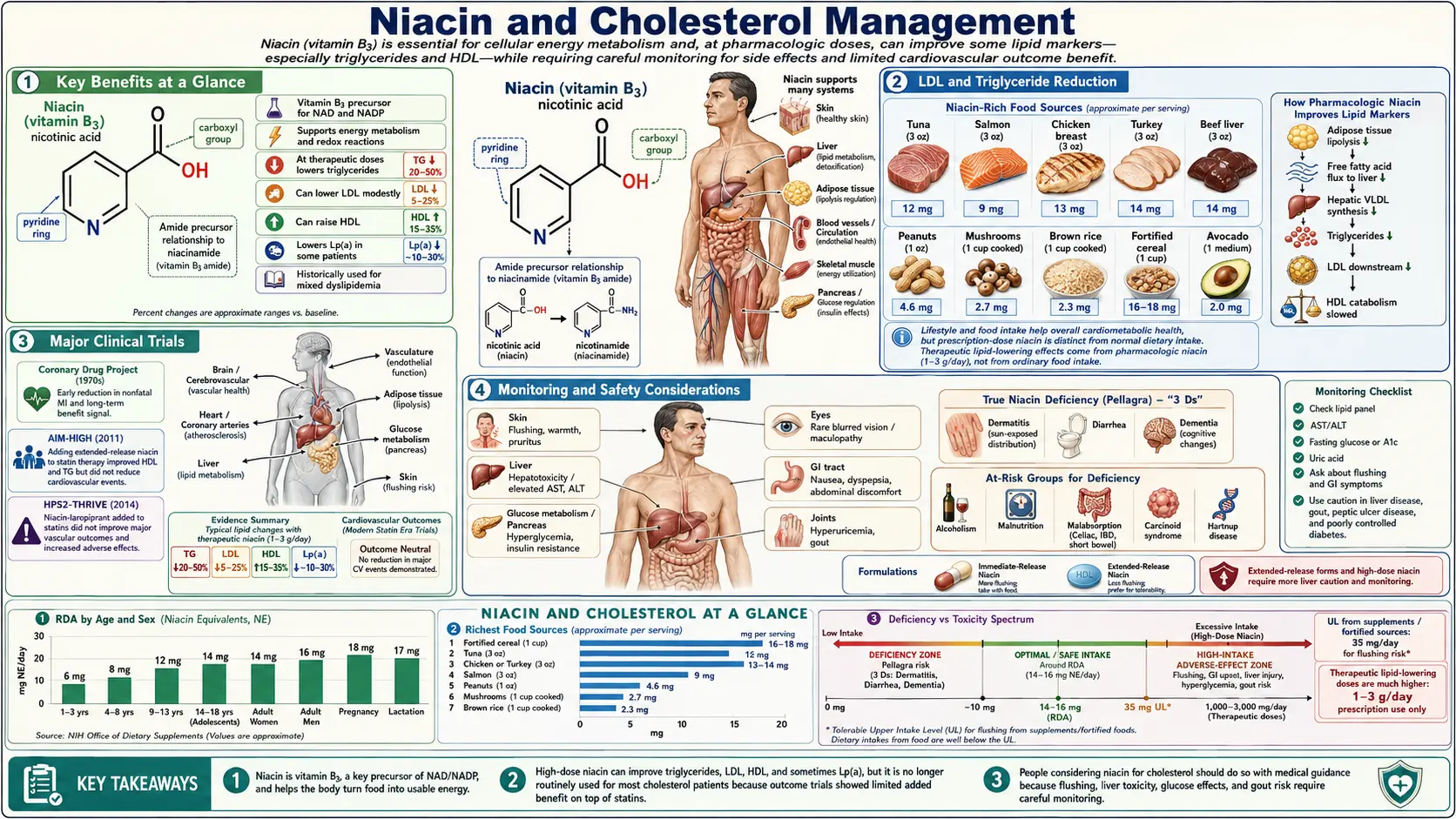
Key Benefits at a Glance
- Raises HDL cholesterol 15–35% — the largest HDL elevation achievable by any single agent.
- Lowers LDL cholesterol 5–25% via inhibition of hepatic DGAT2 and reduced VLDL output.
- Reduces triglycerides 20–50% through suppression of adipocyte lipolysis and hepatic VLDL assembly.
- Lowers lipoprotein(a) 10–30% — one of very few agents that meaningfully reduces this genetically determined risk factor.
- Shifts LDL to larger, less atherogenic particles improving overall lipoprotein profile.
- Long outcome history — the Coronary Drug Project (1975) showed 27% fewer nonfatal MIs and 11% lower 15-year mortality on immediate-release niacin.
- Cost-effective compared to newer PCSK9 inhibitors for select indications.
- Useful in statin-intolerant patients when alternative lipid-lowering therapy is required.
NAD+ and NADP+ Biochemistry
Niacin serves as the precursor to two essential coenzymes that drive hundreds of metabolic reactions throughout the body:
- Nicotinamide adenine dinucleotide (NAD+) — functions primarily as an electron carrier in catabolic (energy-releasing) reactions, including glycolysis, the citric acid cycle, and mitochondrial oxidative phosphorylation. NAD+ is also a critical substrate for sirtuins, poly(ADP-ribose) polymerases (PARPs), and CD38, linking niacin status to DNA repair, gene expression, and cellular aging.
- Nicotinamide adenine dinucleotide phosphate (NADP+) — the phosphorylated form participates in anabolic (biosynthetic) reactions, including fatty acid synthesis, cholesterol synthesis, and the regeneration of reduced glutathione, a key cellular antioxidant.
The dual roles of NAD+ and NADP+ in both energy metabolism and lipid biosynthesis explain why niacin status has far-reaching effects on cholesterol homeostasis. When pharmacological doses of niacin are administered, the surplus availability of these coenzymes shifts hepatic lipid metabolism in ways that produce measurable changes in circulating lipoproteins.
HDL-Raising Mechanism
Niacin is widely recognized as the most effective pharmacological agent for raising HDL cholesterol. At therapeutic doses (1,000 to 2,000 mg per day), niacin can increase HDL-C levels by 15 to 35 percent, surpassing the HDL-raising capacity of statins, fibrates, and CETP inhibitors.
The mechanisms by which niacin elevates HDL include:
- Reduced hepatic uptake of apolipoprotein A-I (apoA-I) — niacin decreases the clearance of apoA-I, the primary protein component of HDL particles, without affecting the synthetic rate. This results in longer circulating half-life of HDL particles.
- Inhibition of cholesteryl ester transfer protein (CETP) activity — niacin reduces the transfer of cholesteryl esters from HDL to VLDL and LDL, preserving cholesterol content within HDL particles.
- Increased ABCA1 expression — niacin upregulates the ATP-binding cassette transporter A1, promoting cholesterol efflux from peripheral tissues to nascent HDL particles, a critical step in reverse cholesterol transport.
LDL and Triglyceride Reduction
Beyond its HDL effects, niacin produces clinically meaningful reductions in atherogenic lipoproteins:
- LDL cholesterol reduction of 5 to 25 percent — niacin inhibits diacylglycerol acyltransferase 2 (DGAT2) in hepatocytes, reducing triglyceride synthesis and consequently decreasing the production of VLDL, the precursor to LDL.
- Triglyceride reduction of 20 to 50 percent — by inhibiting adipocyte lipolysis through the GPR109A receptor, niacin reduces the flux of free fatty acids to the liver, limiting the substrate available for hepatic triglyceride synthesis.
- Lipoprotein(a) reduction of 10 to 30 percent — niacin remains one of the very few agents capable of lowering Lp(a), an independent and genetically determined risk factor for atherosclerotic cardiovascular disease. The mechanism involves reduced hepatic synthesis of apolipoprotein(a).
The GPR109A Receptor and Niacin Flush
The GPR109A receptor (also known as HM74A or HCAR2) is a G-protein-coupled receptor expressed on adipocytes, immune cells, and dermal Langerhans cells. Niacin binds this receptor with high affinity, and this interaction mediates both therapeutic and adverse effects:
- Adipocyte effects — activation of GPR109A on fat cells inhibits hormone-sensitive lipase, reducing lipolysis and lowering circulating free fatty acid levels. This is a primary mechanism for triglyceride and VLDL reduction.
- Flush mechanism — activation of GPR109A on dermal Langerhans cells triggers the release of prostaglandin D2 (PGD2) and prostaglandin E2 (PGE2), which act on dermal blood vessels to cause vasodilation. This produces the characteristic niacin flush: warmth, redness, tingling, and itching of the skin, most prominent on the face, neck, and upper trunk.
Managing the Niacin Flush
The flush is the most common reason patients discontinue niacin therapy. Strategies to reduce flushing include:
- Aspirin pre-treatment — taking 325 mg of aspirin 30 minutes before niacin blocks prostaglandin synthesis and can reduce flush severity by 30 to 40 percent.
- Gradual dose titration — starting at 250 to 500 mg daily and increasing slowly over 4 to 8 weeks allows tachyphylaxis (tolerance) to develop.
- Taking niacin with food — consuming niacin with a meal, particularly one containing some fat, slows absorption and reduces peak plasma levels.
- Avoiding flush triggers — hot beverages, alcohol, and spicy foods can exacerbate flushing and should be avoided around dosing time.
- Extended-release formulations — these produce a more gradual rise in plasma niacin levels, reducing flush intensity compared to immediate-release forms.
Extended-Release vs. Immediate-Release Niacin
The formulation of niacin significantly affects both its efficacy profile and its side effect burden:
- Immediate-release (crystalline) niacin — produces rapid, high peak plasma levels that preferentially activate the GPR109A pathway. This formulation causes the most intense flushing but carries the lowest risk of hepatotoxicity. It is the form used in the Coronary Drug Project, the trial that first demonstrated cardiovascular benefit.
- Extended-release (ER) niacin — absorbed more slowly, producing lower peak levels and reduced flushing. Niaspan is the best-known prescription ER formulation. The slower absorption shifts metabolism toward the amidation pathway, which can increase the risk of hepatotoxicity at high doses.
- Sustained-release (SR) niacin — older over-the-counter formulations with very slow absorption. These carry the highest risk of hepatotoxicity and are generally not recommended for lipid management. Cases of fulminant hepatic failure have been reported, particularly when patients switch from IR to SR niacin at equivalent doses.
Major Clinical Trials
Coronary Drug Project (1975)
This landmark trial demonstrated that immediate-release niacin (3 g/day) reduced nonfatal myocardial infarction by 27 percent and, in 15-year follow-up, showed an 11 percent reduction in total mortality. It established niacin as a legitimate cardiovascular therapy decades before the statin era.
AIM-HIGH Trial (2011)
The Atherothrombosis Intervention in Metabolic Syndrome with Low HDL/High Triglycerides trial tested whether adding extended-release niacin (1,500 to 2,000 mg/day) to simvastatin in patients with established cardiovascular disease would reduce events. Despite significant improvements in HDL and triglycerides, the trial was stopped early for futility: niacin added no incremental benefit over statin therapy alone. Critics noted that the control group received a small dose of immediate-release niacin (50 mg) to mimic flushing, which may have confounded results.
HPS2-THRIVE Trial (2014)
The Heart Protection Study 2 – Treatment of HDL to Reduce the Incidence of Vascular Events enrolled over 25,000 patients and tested extended-release niacin combined with laropiprant (a prostaglandin D2 receptor antagonist to reduce flushing) added to statin therapy. The trial found no reduction in major vascular events and revealed increased risks of serious adverse events, including new-onset diabetes, gastrointestinal complications, bleeding, infections, and musculoskeletal problems. The role of laropiprant in these adverse effects remains debated.
Current Clinical Recommendations
In light of the AIM-HIGH and HPS2-THRIVE results, the role of niacin in lipid management has been substantially narrowed:
- Not recommended as first-line therapy — statins remain the cornerstone of lipid-lowering treatment for cardiovascular risk reduction.
- Limited add-on role — niacin may be considered in patients with persistent dyslipidemia despite maximally tolerated statin therapy, particularly those with low HDL, elevated triglycerides, or elevated Lp(a).
- Statin-intolerant patients — niacin may serve as an alternative in patients who cannot tolerate any statin, though newer agents such as PCSK9 inhibitors and bempedoic acid have largely supplanted this role.
- Lp(a) reduction — until specific Lp(a)-lowering therapies (such as antisense oligonucleotides) become widely available, niacin remains one of the few options for patients with markedly elevated Lp(a).
Comparison with Statins
Understanding the distinct profiles of niacin and statins helps clarify their respective roles:
- LDL reduction — statins are far superior, achieving 30 to 55 percent LDL reduction compared to niacin's 5 to 25 percent.
- HDL elevation — niacin is superior, raising HDL by 15 to 35 percent compared to statins' 5 to 15 percent.
- Triglyceride reduction — both are effective; niacin may achieve modestly greater reductions in patients with very high triglycerides.
- Lp(a) lowering — niacin lowers Lp(a) by 10 to 30 percent; statins have minimal or no effect and may slightly increase Lp(a) levels.
- Cardiovascular outcome evidence — statins have overwhelming outcome trial evidence supporting their use; niacin's outcome data are mixed, with early positive results (Coronary Drug Project) not confirmed in the modern statin-treated population.
- Safety profile — statins are generally well-tolerated with myalgia as the most common complaint; niacin carries risks of flushing, hepatotoxicity, hyperglycemia, hyperuricemia, and gastrointestinal disturbance.
Monitoring and Safety Considerations
Patients taking therapeutic doses of niacin require regular monitoring:
- Liver function tests — should be checked at baseline, after each dose increase, and every 6 to 12 months during maintenance therapy. Niacin should be discontinued if transaminases exceed three times the upper limit of normal.
- Fasting glucose and hemoglobin A1c — niacin can worsen insulin resistance and glycemic control, particularly in patients with diabetes or prediabetes.
- Uric acid levels — niacin competes with uric acid for renal tubular excretion, potentially precipitating gout in susceptible individuals.
- Lipid panel — should be checked 6 to 8 weeks after each dose adjustment to assess therapeutic response.
Research Papers
- Search PubMed
- Search PubMed
- AIM-HIGH Investigators. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med. 2011;365(24):2255-2267.
- HPS2-THRIVE Collaborative Group. Effects of extended-release niacin with laropiprant in high-risk patients. N Engl J Med. 2014;371(3):203-212.
- PubMed — Niacin HDL mechanism (topic search)
- PubMed — Niacin and Lipoprotein(a) (topic search)
- PubMed — GPR109A receptor and niacin flushing (topic search)
- PubMed — Niacin hepatotoxicity (topic search)
- NIH Office of Dietary Supplements — Niacin Fact Sheet for Health Professionals
- Linus Pauling Institute — Niacin
- Harvard T.H. Chan School of Public Health — Niacin (Vitamin B3)
Connections
- All Vitamins
- Vitamin B3
- Pellagra and Niacin Deficiency
- Cardiovascular Disease
- Vitamin E and Heart Health
- Vitamin K2 and Arterial Calcification
- Vitamin B6 and Homocysteine
- Magnesium and Heart Health
- Inflammatory Markers
- Lipid Panel
- Metabolic Syndrome
- Insulin Resistance
- Diabetes
- Fasting
- Uric Acid
- Gout