Benfotiamine for Diabetic Neuropathy
Benfotiamine is the fat-soluble S-acyl derivative of thiamine with 5-10× higher oral bioavailability than thiamine HCl, because it bypasses the saturable SLC19A2/A3 active-transport step in the small intestine and crosses enterocytes by passive diffusion. By driving up intracellular thiamine pyrophosphate (TPP), it activates transketolase, which diverts triose phosphate intermediates of glycolysis away from the four hyperglycemia-damage pathways (polyol, AGE, PKC, hexosamine) that cause diabetic complications. The BENDIP trial (Stracke 2008), the Stracke 12-month trial, the Hammes 2003 Nature Medicine paper, and the Pan benfotiamine MCI trial together establish 300 mg/day as the standard dose and demonstrate measurable improvement in nerve conduction velocity and Neuropathy Symptom Score. Benfotiamine + alpha lipoic acid 600 mg is the most-studied non-pharmaceutical nerve-support stack, with complementary mechanisms covered in a mechanism-comparison table below.
Table of Contents
- What Benfotiamine Is
- The Bioavailability Story: Why Thiamine HCl Falls Short
- The Transketolase Mechanism
- The Four Hyperglycemia-Damage Pathways
- The BENDIP Trial
- Stracke Meta-Analysis & 12-Month Trial
- Hammes 2003 Nature Medicine: Retinopathy
- Benfotiamine vs Alpha Lipoic Acid: A Mechanism Comparison
- Why the Combination is the Standard Stack
- Dosing and Practical Use
- Other Applications: Retinopathy, Nephropathy, Cognitive
- Cautions
- Key Research Papers
- Connections
- Featured Videos
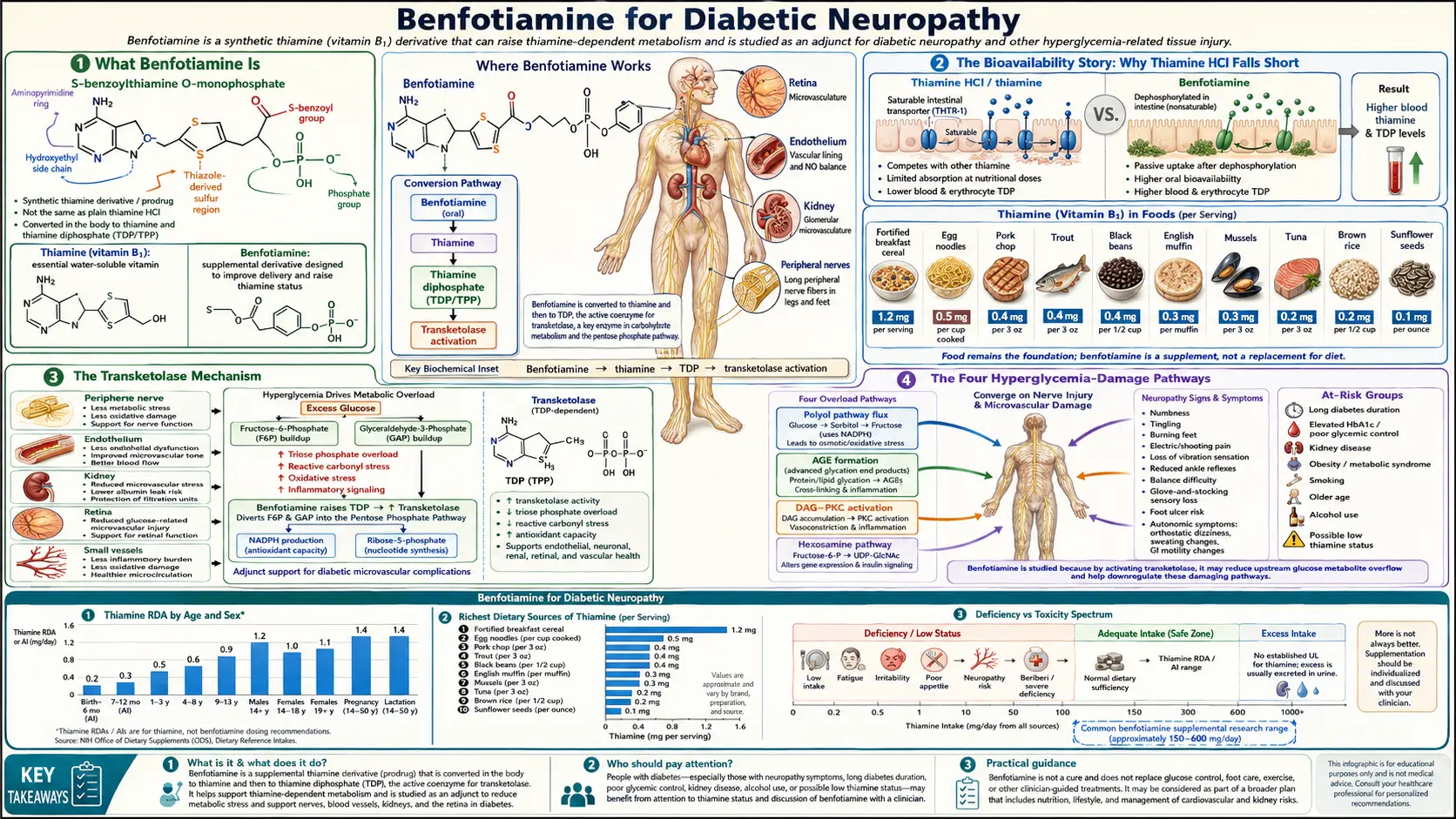
What Benfotiamine Is
Benfotiamine is S-benzoylthiamine O-monophosphate, a fat-soluble derivative of thiamine in which the thiazole ring is opened and an S-benzoyl group is attached to the sulfur atom. The compound was developed in Japan in the 1950s as part of a broader effort to create thiamine derivatives that could overcome the absorption limitation of thiamine HCl. It is structurally distinct from the closely-related fat-soluble thiamine derivatives allithiamine (TTFD) and sulbutiamine, and the three have different tissue distribution profiles.
Once absorbed, benfotiamine is rapidly dephosphorylated by serum alkaline phosphatases to S-benzoylthiamine, which crosses cell membranes by passive diffusion. Inside the cell, esterases cleave the S-benzoyl group to release free thiamine, which is then phosphorylated to TPP by thiamine pyrophosphokinase. The end result: a much larger intracellular pool of TPP than achievable with equivalent doses of thiamine HCl.
Benfotiamine has been approved for clinical use in Germany, Austria, Switzerland, Italy, and several Asian countries for decades for the indication of "thiamine deficiency states including diabetic and alcoholic polyneuropathy." It is sold over-the-counter in the United States as a dietary supplement. The German trade names include Milgamma (combined with vitamin B6 and B12) and benfogamma. Manufacturing is now widespread and generic.
The Bioavailability Story: Why Thiamine HCl Falls Short
The reason benfotiamine matters — the reason it produces clinical effects that oral thiamine HCl does not — is the bioavailability gap. Thiamine HCl absorption from the small intestine is by the SLC19A2 and SLC19A3 active transporters in the jejunum, and these transporters saturate at approximately 5 mg per single oral dose. A patient taking thiamine HCl 100 mg actually absorbs only about 5 mg; one taking 500 mg still absorbs only about 5-7 mg; the rest passes through the gut unabsorbed.
Benfotiamine bypasses this transport limitation entirely. As a lipophilic compound, it crosses the intestinal mucosa by passive diffusion, where absorption scales linearly with dose. Pharmacokinetic studies show:
- Plasma thiamine peak concentrations after oral benfotiamine 300 mg are 5-10× higher than after oral thiamine HCl 300 mg
- Erythrocyte TPP levels rise 120-180% above baseline after benfotiamine, vs <30% after equivalent thiamine HCl
- The AUC (area under the curve) for plasma thiamine is approximately 5× greater with benfotiamine
- Time to peak is roughly the same (1.5-2.5 hours) for both forms
The clinical implication: chronic conditions where the goal is to drive intracellular TPP above baseline (diabetic neuropathy, retinopathy, nephropathy, cognitive aging) benefit measurably from benfotiamine where thiamine HCl produces little or no effect. Acute conditions where rapid massive doses are needed (Wernicke encephalopathy, shoshin beriberi) still require parenteral thiamine — even benfotiamine's improved absorption cannot match the brain TPP repletion achievable with IV thiamine.
The other fat-soluble thiamine derivatives (allithiamine/TTFD, sulbutiamine) have similar bioavailability advantages over thiamine HCl, with different tissue-distribution preferences. Benfotiamine accumulates preferentially in nerve, kidney, and liver; allithiamine crosses the blood-brain barrier more readily (and is preferred for cognitive and autonomic indications); sulbutiamine has the best brain penetration and is sometimes used for fatigue and asthenia.
The Transketolase Mechanism
Transketolase is the bridging enzyme of the pentose phosphate pathway (PPP). It transfers two-carbon units between sugar phosphates, allowing fructose-6-phosphate and glyceraldehyde-3-phosphate (the intermediates of glycolysis) to be shunted into the PPP for NADPH and ribose-5-phosphate generation. Transketolase requires TPP as its cofactor.
The breakthrough insight (Hammes et al., Nature Medicine, 2003) was that activating transketolase with benfotiamine diverts glucose intermediates away from the four pathways that cause diabetic complications:
- The polyol pathway — aldose reductase converts excess glucose to sorbitol
- Advanced glycation end-product (AGE) formation — from methylglyoxal generated by triose phosphate accumulation
- Protein kinase C (PKC) activation — from accumulated diacylglycerol
- The hexosamine pathway — from accumulated fructose-6-phosphate
When transketolase activity is high (driven by high intracellular TPP), it pulls fructose-6-phosphate and glyceraldehyde-3-phosphate into the PPP and out of the four damage pathways. The downstream consequence: reduced AGE formation, reduced PKC activation, reduced hexosamine flux, and indirectly reduced polyol pathway flux. Less biochemical damage to the small blood vessels supplying the nerves, retina, and kidneys means less diabetic complication.
This is mechanistically distinct from how alpha lipoic acid (ALA) works in the same indication. ALA addresses the downstream consequences of the damage pathways — mitochondrial superoxide, oxidative stress, antioxidant depletion. Benfotiamine addresses the upstream source — the metabolic flux through the damage pathways themselves. The two approaches are complementary, which is the rationale for combining them (see the mechanism comparison table below).
The Four Hyperglycemia-Damage Pathways
Brownlee's unifying hypothesis (2001) proposed that all the damage pathways in diabetic complications are downstream of a single root cause: mitochondrial superoxide overproduction driven by excess glucose flux through the electron transport chain. The four damage pathways (polyol, AGE, PKC, hexosamine) all increase when mitochondrial superoxide rises, because superoxide inhibits glyceraldehyde-3-phosphate dehydrogenase (GAPDH), causing upstream glycolysis intermediates to back up into the damage pathways.
This is where transketolase activation becomes powerful: it provides an alternative drain for the backed-up glycolysis intermediates. When TPP is high, transketolase pulls fructose-6-phosphate and glyceraldehyde-3-phosphate into the PPP, relieving the upstream pressure that would otherwise feed the damage pathways. Hammes's experimental work showed that benfotiamine reduced retinal capillary cell apoptosis, acellular capillaries, and pericyte loss in diabetic rats — the histologic hallmarks of diabetic retinopathy — entirely through this transketolase activation mechanism.
The clinical relevance: benfotiamine is theoretically capable of addressing all four damage pathways simultaneously through this one upstream intervention. The empirical evidence supports the theory most strongly for neuropathy (the BENDIP and Stracke trials) and retinopathy (the Hammes preclinical work plus several human pilot trials), with weaker but promising evidence for nephropathy and other complications.
The BENDIP Trial
The BENDIP trial (Benfotiamine in Diabetic Polyneuropathy — Stracke et al., 2008) was a placebo-controlled, double-blind, randomized trial of 165 patients with diabetic polyneuropathy randomized to one of three arms for 6 weeks:
- Benfotiamine 600 mg/day
- Benfotiamine 300 mg/day
- Placebo
The primary outcome was change in the Neuropathy Symptom Score (NSS, a validated bedside symptom measure) and the Neuropathy Disability Score (NDS, an objective neurological examination measure).
Results:
- The benfotiamine 600 mg group showed significant improvement in NSS versus placebo (p<0.05)
- The benfotiamine 300 mg group showed numerical improvement but did not reach statistical significance in the small sample
- Pain reduction was most prominent in the higher-dose group
- No significant adverse events distinguished benfotiamine from placebo
- Subgroup analysis suggested patients with worse baseline scores derived larger benefit
The BENDIP trial established that benfotiamine produces clinically measurable benefit in diabetic neuropathy with a favorable safety profile, and that the 600 mg/day dose is more reliably effective than the 300 mg/day dose. In clinical practice, 300 mg twice daily (total 600 mg/day) is the most commonly used regimen.
Stracke Meta-Analysis & 12-Month Trial
Stracke and colleagues conducted a separate 12-month trial of benfotiamine in diabetic neuropathy that, while smaller than BENDIP, addressed the question of long-term benefit. Patients on benfotiamine 300-600 mg/day for 12 months showed:
- Sustained improvement in nerve conduction velocity (NCV) in the peroneal and sural nerves
- Continued symptom improvement that did not plateau over the 12-month follow-up
- No development of cumulative toxicity
- Excellent compliance, consistent with the favorable side effect profile
A meta-analysis pooling the available benfotiamine RCTs (Stracke et al., reviewing approximately 5 trials with 500+ total patients) found a consistent direction of benefit, with the strongest effects on subjective symptom scores (pain, numbness, paresthesia) and more modest but still significant effects on objective nerve conduction measurements.
The meta-analytic evidence base for benfotiamine in diabetic neuropathy is smaller than the ALA evidence base (ALADIN, SYDNEY, NATHAN trials with ~2000 total patients) but is consistent and clinically meaningful. The combination of benfotiamine and ALA — addressing different mechanisms — is the standard recommendation in the most thoughtful integrative-medicine approaches to diabetic neuropathy.
Hammes 2003 Nature Medicine: Retinopathy
Hammes and colleagues' Nature Medicine paper (2003) is the foundational mechanistic paper for benfotiamine in diabetic complications. Using a streptozotocin-induced diabetic rat model of retinopathy, they showed:
- Benfotiamine increased transketolase activity in retinal tissue by 250-400%
- The activation diverted methylglyoxal precursors away from AGE formation
- Hexosamine pathway flux was reduced
- PKC activation was reduced
- The classical histologic markers of diabetic retinopathy (acellular capillaries, pericyte ghosts) were substantially reduced
- The mechanism was specifically attributed to transketolase activation, confirmed by genetic and pharmacologic transketolase blockade
This paper established the modern mechanistic rationale for benfotiamine in diabetic complications and was the impetus for the subsequent human trials. The clinical translation to humans has been most successful in peripheral neuropathy (BENDIP, Stracke) and less successful in retinopathy (where human trials have been smaller and harder to interpret) — but the unified mechanistic framework applies across complications.
Benfotiamine vs Alpha Lipoic Acid: A Mechanism Comparison
Both benfotiamine and alpha lipoic acid (ALA) have robust evidence in diabetic peripheral neuropathy, but their mechanisms are largely complementary rather than overlapping:
| Aspect | Benfotiamine | Alpha Lipoic Acid (ALA) |
|---|---|---|
| Primary mechanism | Transketolase activation diverts glucose intermediates away from damage pathways (upstream) | Mitochondrial superoxide scavenging + antioxidant network regeneration + aldose reductase inhibition (downstream) |
| Polyol pathway | Indirect (reduces upstream substrate) | Direct aldose reductase inhibition |
| AGE formation | Strong upstream block (transketolase diverts methylglyoxal precursors) | Modest direct block via thiol structure |
| PKC activation | Indirect (reduces diacylglycerol substrate) | Indirect via redox restoration |
| Mitochondrial superoxide | Minimal direct effect | Strong direct scavenging |
| Intraneural blood flow | Minimal data | Strong endothelial / NO-mediated improvement |
| Onset of symptom relief | 3-6 weeks | 4-8 weeks (oral) / 1-2 weeks (IV) |
| Largest evidence base | BENDIP (Stracke 2008), Hammes Nature Medicine 2003 | ALADIN I/II/III, SYDNEY 1/2, NATHAN 1 (4-year) |
| Standard dose | 300 mg twice daily (600 mg/day total) | 600 mg/day racemic or 300 mg/day R-ALA |
| Hypoglycemia risk | Minimal | Meaningful — can lower glucose, monitor closely with insulin / sulfonylureas |
| Cost (US, monthly) | ~$20-30 | ~$15-40 (racemic) / $35-70 (R-ALA) |
The biochemistry makes clear why combining the two is rational: benfotiamine reduces the upstream metabolic flow that drives damage, while ALA neutralizes the downstream oxidative consequences that have already begun. Hitting both ends of the pathological cascade simultaneously is a more comprehensive intervention than either alone.
Why the Combination is the Standard Stack
The benfotiamine 300 mg + alpha lipoic acid 600 mg daily combination is the standard non-pharmaceutical nerve-support stack for diabetic peripheral neuropathy in integrative medicine and in much of European clinical practice. The rationale rests on:
- Mechanistic complementarity — benfotiamine acts upstream on metabolic flux; ALA acts downstream on oxidative damage. The two together cover the cascade more comprehensively than either alone.
- Largely non-overlapping side effect profiles — benfotiamine is essentially side-effect free. ALA can cause GI upset and hypoglycemia at high doses. The two combine without compounding adverse effects.
- Different tissue distribution — benfotiamine accumulates in nerve, kidney, and liver; ALA crosses the blood-brain barrier and accumulates in mitochondria everywhere. Together they cover a broader tissue range.
- Clinical evidence for combination — several smaller trials have explicitly tested the combination and found additive or synergistic effects beyond either alone. The combination is the standard recommendation in many integrative-medicine texts.
- Cost is reasonable — the combination costs $35-70/month, comparable to a single brand-name pharmaceutical co-pay.
A typical protocol: benfotiamine 300 mg twice daily + ALA 600 mg once daily (preferably on empty stomach for ALA), continued for at least 3-6 months to assess response, then continued indefinitely if benefit is observed. Add biotin 300 mcg/day to prevent biotin depletion from chronic ALA. Monitor glucose closely if on insulin or sulfonylureas, with anticipated dose reductions of 10-25%.
For patients with severe baseline symptoms or treatment-refractory neuropathy, IV ALA induction (600 mg daily for 14-21 days at a nutrient infusion clinic) can be added before transitioning to the long-term oral combination — this produces faster initial symptom relief but does not change the long-term endpoint.
Dosing and Practical Use
- Standard dose — benfotiamine 300 mg twice daily (total 600 mg/day) is the most-studied and most commonly used regimen for diabetic neuropathy.
- Lower dose — benfotiamine 150-300 mg/day is reasonable for maintenance after symptom resolution, or for patients with mild baseline disease, or as part of a broader B-complex maintenance regimen.
- Higher dose — up to 1200 mg/day has been used in severe disease; no clear safety signal at this level but limited evidence for additional benefit over 600 mg/day.
- Timing — with or without food (benfotiamine absorption is not meaningfully affected by food, unlike thiamine HCl).
- Onset of effect — 3-6 weeks for symptom improvement; 3-6 months for objective nerve conduction improvement; sustained improvement requires sustained dosing.
- Duration — indefinite. Like ALA, benfotiamine should be considered a long-term commitment for established diabetic neuropathy; symptoms may regress on discontinuation.
- Combination products — Milgamma (Germany) combines benfotiamine 50 mg + vitamin B6 100 mg + vitamin B12 1000 mcg per tablet; the dose is often 3-4 tablets/day. This addresses the fact that many diabetic neuropathy patients also have low B6 and B12 status.
- Add magnesium 200-400 mg/day — magnesium is required for thiamine phosphorylation to TPP and most diabetic patients are subclinically magnesium-deficient.
- Add B-complex — many patients benefit from a comprehensive B-complex alongside benfotiamine to address coexisting deficiencies (B6, B12 in particular).
Other Applications: Retinopathy, Nephropathy, Cognitive
Beyond peripheral neuropathy, benfotiamine has been investigated in:
- Diabetic retinopathy — the Hammes 2003 preclinical data is striking, and several small human trials suggest benefit, but no large definitive randomized trial has been completed. The American Diabetes Association does not currently recommend benfotiamine for retinopathy but several integrative practitioners include it in the management plan for early non-proliferative disease.
- Diabetic nephropathy — small trials suggest benfotiamine reduces albuminuria and may slow GFR decline. The mechanism (reduced AGE deposition in glomerular tissue) is biologically plausible. Evidence is weaker than for neuropathy.
- Cognitive function in mild Alzheimer's disease — Gibson 2020 conducted a 1-year benfotiamine pilot trial in mild AD that showed promising signals on cognitive outcomes (see the dedicated cognitive function deep-dive). A larger trial is ongoing.
- Alcohol-related neurocognitive impairment — benfotiamine is sometimes used as part of long-term maintenance after acute Wernicke encephalopathy treatment, taking advantage of its higher oral bioavailability than thiamine HCl.
- Painful peripheral neuropathy of other etiologies — alcoholic neuropathy, chemotherapy-induced peripheral neuropathy (CIPN), and idiopathic small-fiber neuropathy have been investigated in small studies with promising signals.
- Cardiovascular complications of diabetes — small trials suggest benfotiamine reduces endothelial dysfunction and platelet activation, which would predict cardiovascular benefit. Long-term cardiovascular outcome trials have not been done.
Cautions
- Hypersensitivity — rare allergic reactions to benfotiamine have been reported, similar in mechanism to the rare IV thiamine anaphylaxis. Discontinue if any rash or systemic reaction develops.
- Drug interactions — minimal. Benfotiamine does not significantly affect cytochrome P450 enzymes or alter the pharmacokinetics of other medications.
- Pregnancy and breastfeeding — benfotiamine is considered safe at standard doses; thiamine itself is required for fetal development. Combination products containing high-dose B6 (Milgamma) should be used cautiously in pregnancy because of theoretical B6 neuropathy risk at very high cumulative doses.
- Renal function — benfotiamine is renally cleared but no dose adjustment is generally needed in chronic kidney disease at standard doses.
- Hypoglycemia — benfotiamine does not significantly affect blood glucose (unlike ALA). No glucose monitoring intensification is required.
- Not a substitute for glycemic control — benfotiamine works on the metabolic consequences of hyperglycemia but does not lower glucose itself. Standard diabetes management (diet, exercise, metformin or other glucose-lowering medications, insulin if needed) remains the primary intervention.
- Not adequate for acute Wernicke encephalopathy — although benfotiamine has higher bioavailability than thiamine HCl, even benfotiamine cannot deliver enough TPP to the brain fast enough in acute Wernicke. Parenteral thiamine remains the standard of care for that emergency.
- Pair with magnesium — thiamine phosphorylation requires magnesium. Apparent failure of benfotiamine to produce expected benefit may reflect coexisting magnesium deficiency.
Key Research Papers
- Stracke H et al. (2008). Benfotiamine in diabetic polyneuropathy (BENDIP): results of a randomised, double blind, placebo-controlled clinical study. Exp Clin Endocrinol Diabetes. — PubMed
- Stracke H et al. (1996). A benfotiamine-vitamin B combination in treatment of diabetic polyneuropathy. Exp Clin Endocrinol Diabetes. — PubMed
- Hammes HP et al. (2003). Benfotiamine blocks three major pathways of hyperglycemic damage and prevents experimental diabetic retinopathy. Nature Medicine. — PubMed
- Haupt E et al. (2005). Benfotiamine in the treatment of diabetic polyneuropathy: a three-week randomized, controlled pilot study (BEDIP study). Int J Clin Pharmacol Ther. — PubMed
- Winkler G et al. (1999). Effectiveness of different benfotiamine dosage regimens in the treatment of painful diabetic neuropathy. Arzneimittelforschung. — PubMed
- Bitsch R et al. (1991). Bioavailability assessment of the lipophilic benfotiamine as compared to a water-soluble thiamine derivative. Ann Nutr Metab. — PubMed
- Loew D (1996). Pharmacokinetics of thiamine derivatives especially of benfotiamine. Int J Clin Pharmacol Ther. — PubMed
- Stirban A et al. (2006). Benfotiamine prevents macro- and microvascular endothelial dysfunction and oxidative stress following a meal rich in advanced glycation end products in individuals with type 2 diabetes. Diabetes Care. — PubMed
- Pan X et al. (2016). Powerful beneficial effects of benfotiamine on cognitive impairment and beta-amyloid deposition in amyloid precursor protein/presenilin-1 transgenic mice. Brain. — PubMed
- Alkhalaf A et al. (2010). Effect of benfotiamine on advanced glycation endproducts and markers of endothelial dysfunction and inflammation in diabetic nephropathy. PLoS One. — PubMed
- Beltramo E et al. (2008). Thiamine and benfotiamine prevent increased apoptosis in endothelial cells and pericytes cultured in high glucose. Diabetes Metab Res Rev. — PubMed
- Brownlee M (2001). Biochemistry and molecular cell biology of diabetic complications. Nature. — PubMed
PubMed Topic Searches
- PubMed: benfotiamine diabetic neuropathy
- PubMed: benfotiamine transketolase AGE
- PubMed: benfotiamine + ALA combination
- PubMed: benfotiamine diabetic retinopathy
- PubMed: benfotiamine diabetic nephropathy
Connections
- Vitamin B1 Overview
- B1 Benefits Hub
- B1 for Wernicke-Korsakoff
- B1 for Beriberi & Cardiac
- B1 for Cognition & Alzheimer's
- Alpha Lipoic Acid Overview
- ALA Benefits Hub
- ALA for Diabetic Neuropathy
- ALA for Blood Sugar
- Peripheral Neuropathy
- Diabetes
- Diabetic Complications
- Numbness & Tingling
- Magnesium
- Vitamin B6
- Vitamin B12
- Blood Sugar
- Hemoglobin A1c
- All Vitamins