PFAS: The “Forever Chemicals” in Your Water, Food, and Blood
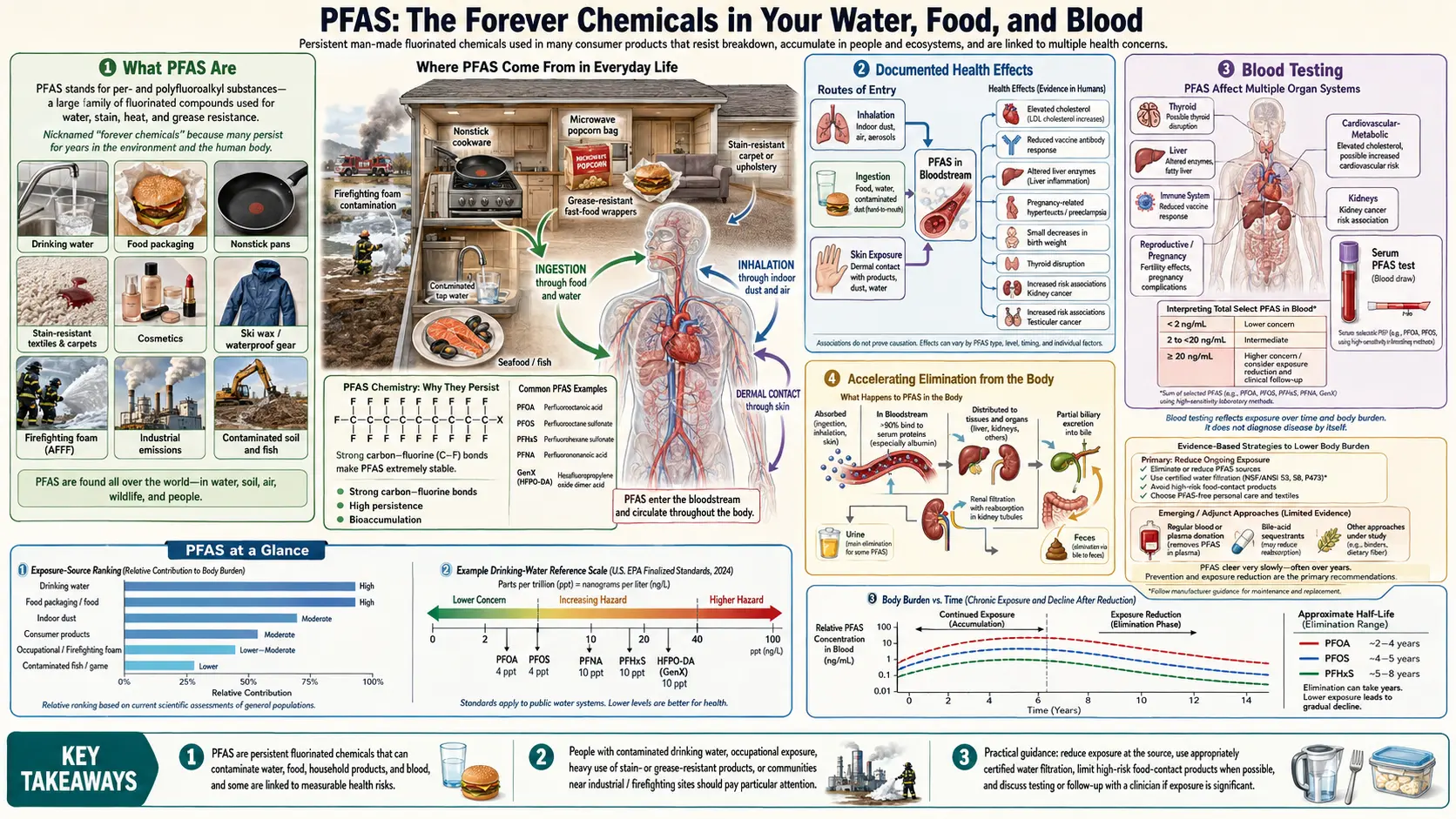


Per- and polyfluoroalkyl substances (PFAS) are a family of more than 14,000 synthetic chemicals defined by extraordinarily stable carbon-fluorine bonds — the strongest single covalent bond in organic chemistry. That stability is what gives non-stick cookware its non-stick, waterproof jackets their repellency, food packaging its grease resistance, and firefighting foams their effectiveness. It also means these chemicals essentially do not break down in the environment or the body, earning them the nickname forever chemicals. PFAS have now been detected in drinking water serving roughly 200 million Americans, in virtually every rainfall sampled worldwide, and in the blood of more than 98 percent of people tested in the United States.
Substantial epidemiological evidence links PFAS exposure to cancer, thyroid disease, liver injury, cholesterol elevation, reduced vaccine response, pregnancy complications, and developmental effects in children. Regulatory response has accelerated sharply since 2023. This article lays out what PFAS are, where they come from, what we know about their health effects, how to test, and practical steps to reduce ongoing exposure.
Table of Contents
- What PFAS Are
- Major Exposure Sources
- Documented Health Effects
- Regulatory Developments
- Blood Testing
- How to Reduce Exposure
- Accelerating Elimination from the Body
- Connections
- Featured Videos
What PFAS Are
PFAS share a structural backbone of carbon atoms fully substituted with fluorine atoms. The best-studied members are PFOA (perfluorooctanoic acid, formerly used in Teflon production) and PFOS (perfluorooctanesulfonic acid, formerly used in Scotchgard and firefighting foam). Both have been phased out of U.S. production but remain in the environment indefinitely. Newer “short-chain” replacements like GenX, ADONA, and F-53B were developed as substitutes but many have shown similar or even greater toxicity and persistence.
Major Exposure Sources
- Drinking water — public-water supplies near military bases, airports (firefighting foam), and manufacturing facilities often have the highest levels. Private wells in affected regions can have dramatically higher levels.
- Non-stick cookware (older or degraded).
- Greaseproof food packaging — microwave popcorn bags, fast-food wrappers, pizza boxes, compostable tableware.
- Waterproof and stain-resistant fabrics — treated outdoor gear, carpets, upholstery.
- Cosmetics — particularly long-wear foundation, mascara, and lipstick.
- Dental floss — some PTFE-coated varieties.
- Fish from contaminated waters — PFAS bioaccumulate up the food chain.
- Dairy and meat from exposed livestock.
Documented Health Effects
A 2022 National Academies consensus report identified strong or moderate evidence linking PFAS exposure to:
- Kidney and testicular cancer. PFOA is classified as a Group 1 human carcinogen by IARC.
- Thyroid disease. Both hyperthyroidism and hypothyroidism, and altered TSH across populations.
- Elevated cholesterol. PFOA/PFOS clearly raise total and LDL cholesterol.
- Decreased antibody response to vaccines in children.
- Pregnancy complications — pregnancy-induced hypertension, preeclampsia, reduced birth weight.
- Liver injury. Elevated ALT and enhanced fatty liver.
- Ulcerative colitis.
- Reduced fertility.
Additional associations with diabetes, cardiovascular disease, immune dysregulation, and neurodevelopmental effects are actively being investigated.
Regulatory Developments
In 2024 the U.S. EPA finalized drinking-water limits for six PFAS with a PFOA and PFOS maximum of 4 parts per trillion, among the lowest allowable limits for any regulated contaminant. European regulatory bodies and individual U.S. states (Maine, Vermont, Michigan) have moved to ban or restrict PFAS in food packaging, cosmetics, firefighting foam, and consumer products. Class-action litigation against manufacturers has produced multi-billion-dollar settlements.
Blood Testing
A clinical-grade blood PFAS panel typically measures 10–40 PFAS species and costs $200–500 out of pocket. The National Academies has published a clinical framework that suggests specific follow-up actions based on total PFAS concentration: routine care at <2 ng/mL, modest intensification of screening (lipids, thyroid, liver) at 2–20 ng/mL, and enhanced screening with additional cancer surveillance above 20 ng/mL. Not every clinician is familiar; a print-out of the NASEM guidance can help navigate.
How to Reduce Exposure
- Test and treat your drinking water. Reverse-osmosis and certain activated-carbon-block filters remove most PFAS. Carbon pitchers alone are variable; look for NSF/ANSI 53 or 58 certification specifically for PFOA/PFOS.
- Replace non-stick cookware with cast iron, stainless steel, ceramic, or glass when older pans show wear.
- Avoid greaseproof food packaging — compostable tableware, microwave popcorn bags, and fast-food wrappers are common sources.
- Skip Teflon-coated dental floss. Choose PTFE-free alternatives.
- Check personal-care products at the Environmental Working Group (EWG) Skin Deep database. Avoid “PFAS-free” claim-washing by checking ingredient lists for “fluoro-” prefixes.
- Minimize freshwater fish from known contaminated waters. Check state PFAS advisories.
- Request low-PFAS water from your utility and support strengthened local standards.
Accelerating Elimination from the Body
PFAS half-lives in humans are measured in years. Biological elimination is slow. Strategies with some evidence of accelerating clearance:
- Bile-binding fiber. Daily cholestyramine (a bile-acid sequestrant) has been studied and shown to accelerate PFAS elimination. Soluble fibers such as psyllium, beta-glucan, and pectin may provide a weaker but safer natural analog.
- Blood donation and therapeutic phlebotomy. A 2022 randomized trial in firefighters showed that regular blood donation measurably reduced blood PFAS levels.
- Weight stability. Rapid weight loss mobilizes PFAS from fat stores; loss should be gradual.
- Breastfeeding does transfer PFAS to infants but is still net-beneficial in most assessments.
Connections
- Cancer
- Heavy Metals
- Detox Protocols
- BPA and Plastics
- Pesticides
- Thyroid Panel
- Lipid Panel
- Liver Cleansing
- GGT
- Microplastics
- Cardiovascular Disease
- Diabetes
- Ulcerative Colitis
- Hypertension
- Iron
- Household Chemicals