 — April 14, 2026
· The Xylitol Paradox
— April 14, 2026
· The Xylitol Paradox
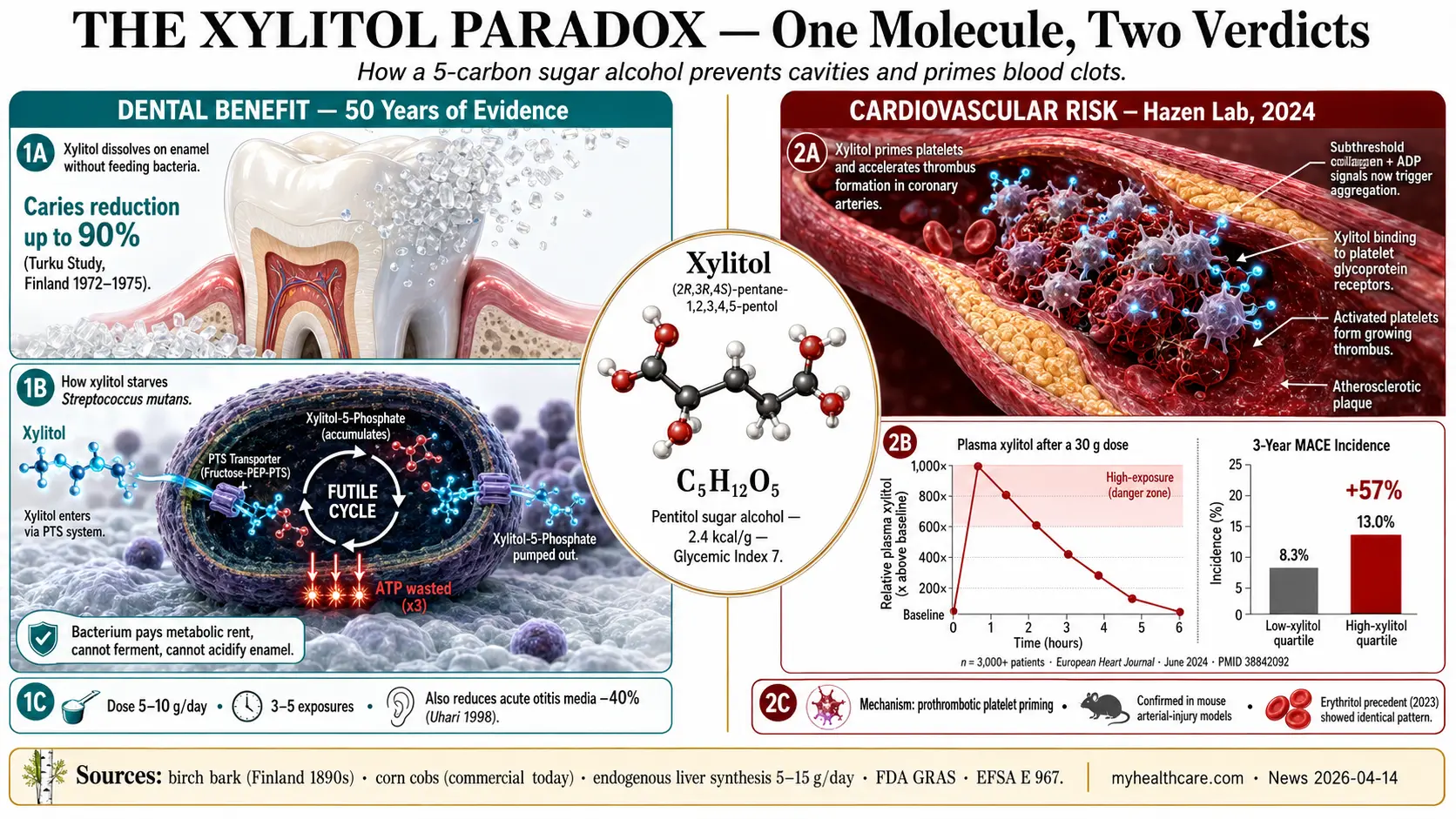

Table of Contents
- The Xylitol Paradox
- What Xylitol Is and Where It Comes From
- 1. The Dental Story — A Sugar That Stops Cavities
- 2. The Mechanism in Streptococcus mutans
- 3. Dose, Frequency, and Real-World Dental Outcomes
- 4. Beyond Cavities — Otitis Media, Sinus, Oral Microbiome
- 5. The 2024 Cleveland Clinic Cardiovascular Paper
- 6. How Xylitol Activates Platelets — The Mechanism
- 7. The Erythritol Precedent (Same Lab, 2023)
- 8. “Prothrombotic, Not a Blood Thinner” — The Distinction That Matters
- 9. Dose and Exposure — Chewing Gum vs Baking Bulk
- 10. Pet Toxicity — A Separate, Serious Warning
- 11. GI Tolerance and Other Adverse Effects
- Practical Synthesis — Who Should and Shouldn’t Use Xylitol
- References & Further Reading
- Related Articles on MyHealthcare.com
- Featured Videos
The Xylitol Paradox
Xylitol is one of the most genuinely interesting molecules on the supplement shelf. For roughly four decades, the dental literature has documented its ability to reduce dental caries, lower Streptococcus mutans counts in plaque and saliva, and even cut the incidence of acute otitis media in young children. Pediatric dentistry guidelines on three continents include it. Dentists hand out xylitol mints to parents. Sugar-free gum brands market the “100% xylitol” label like a badge of honor. In a category — non-nutritive sweeteners — where the public-health story is mostly negative, xylitol has been the exception that earned grudging respect.
And then, in June 2024, a research group at the Cleveland Clinic led by Dr. Stanley Hazen published a paper in the European Heart Journal that changed the conversation. Using the same methodology that had previously implicated erythritol — another sugar alcohol marketed as “safe” — in cardiovascular event risk, the Hazen group reported that elevated plasma xylitol was associated with a roughly 57 percent higher incidence of major adverse cardiovascular events (MACE) over three years, in a cohort of more than 3,000 patients. They went further: they fed healthy volunteers a single 30-gram xylitol drink (the amount in a typical “keto” baked good), measured plasma xylitol rising roughly a thousand-fold above baseline, and watched circulating platelets become primed to clump in response to triggers they would normally have ignored. They reproduced the effect in mouse arterial-injury models. They proposed a mechanism. And they used a precise word for what they had found: not “blood thinner,” but prothrombotic — pro-clotting.
Today’s edition is an attempt to hold both halves of this story honestly. The dental benefit is real and well documented. The cardiovascular signal is new, biologically plausible, mechanistically substantiated in human and animal models, and not yet definitively proven by randomized trial. The right way to think about xylitol in 2026 is not as a hero or a villain but as a tool — one whose risk-benefit calculation depends almost entirely on the dose, the form, and the user’s background cardiovascular risk. A peri-menopausal woman on aspirin for secondary prevention should think about xylitol differently than a healthy child whose pediatric dentist recommends a mint after lunch. This edition pulls together the dental literature, the Cleveland Clinic platelet papers, the older mechanistic studies, the FDA / EFSA safety positions, and the practical synthesis.
What Xylitol Is and Where It Comes From
Xylitol (chemical formula C5H12O5, IUPAC name (2R,3R,4S)-pentane-1,2,3,4,5-pentol) is a five-carbon sugar alcohol — a “pentitol”. Its sweetness on the human tongue is roughly equal to sucrose (table sugar), but it contributes only about 2.4 kilocalories per gram versus sucrose’s 4.0, and it carries a glycemic index of approximately 7 versus sucrose’s 65, meaning it raises blood glucose only minimally. These three properties — the sweetness, the lower calorie load, and the negligible glycemic effect — explain its commercial appeal in diabetic, ketogenic, and dental-product applications.
Naturally, xylitol occurs in small amounts in birch bark (the original 1890s isolation source, a Finnish discovery during World War II sugar shortages that drove the first commercial production), in corn cobs and corn husks (the dominant commercial source today, via acid hydrolysis of xylan-rich hemicellulose followed by hydrogenation), and in trace amounts in plums, strawberries, raspberries, mushrooms, cauliflower, and oats. The human body itself produces xylitol endogenously through the pentose phosphate pathway as an intermediate of glucuronate metabolism — an adult liver synthesizes roughly 5 to 15 grams per day even on a xylitol-free diet, which is why basal plasma levels are detectable in everyone and not just supplement users.
Industrial xylitol production proceeds in two main routes. The traditional chemical route hydrolyzes xylan-rich plant material (corn cob, birch wood) to D-xylose, then hydrogenates the D-xylose to xylitol using a nickel catalyst at high pressure. The newer biotechnological route uses yeasts (typically Candida tropicalis or engineered Saccharomyces cerevisiae) to ferment xylose to xylitol with higher selectivity and lower energy input. Both routes yield a pharmacopoeial-grade crystalline product; the choice between them is a manufacturing-economics question with no clinical consequence for the consumer.
Xylitol’s regulatory status is firmly “Generally Recognized as Safe” (GRAS) under the U.S. FDA framework, with European Food Safety Authority (EFSA) approval under E-number E 967. The acceptable daily intake (ADI) has not been formally set because of xylitol’s favorable acute toxicology profile in humans; the practical limit is set by gastrointestinal tolerance, not by toxicity. As we will see, the 2024 cardiovascular data complicate that “no upper limit” framing — not because xylitol is acutely toxic, but because habitual high exposure has now been associated with an outcome that the GRAS framework was never designed to evaluate.
1. The Dental Story — A Sugar That Stops Cavities
The xylitol-and-cavities story begins in Turku, Finland in 1972–1975, with a now-classic two-year study led by Kauko Mäkinen at the University of Turku. The trial randomized 125 adult volunteers to consume virtually all dietary sugar as either sucrose, fructose, or xylitol; participants in the xylitol arm developed essentially no new caries over the two years (formally, a 90 percent reduction in caries increment versus the sucrose arm). Subsequent reanalysis tempered the magnitude but not the direction of the effect, and the “Turku study” entered the dental textbooks as the foundational human evidence that xylitol substitution prevents tooth decay.
The subsequent half-century built on that scaffold. A series of randomized trials in Finland (Isokangas, Alanen, Tiekso, Mäkinen) and in the United States, Canada, and Belize examined xylitol gum, lozenges, syrups, dentifrices, and chewable tablets in adults, in schoolchildren, in preschoolers, and in pregnant women. The most-cited summary remains the 2015 Cochrane systematic review by Riley and colleagues (PMID 25809586), which evaluated 10 trials with roughly 5,900 participants and concluded that fluoride toothpaste containing 10 percent xylitol reduced caries increment by approximately 13 percent compared with fluoride toothpaste alone — a modest but statistically meaningful effect — while finding the evidence for xylitol-containing lozenges, gum, and candies to be of low quality and inconsistent magnitude. The Cochrane group did not say “xylitol doesn’t work.” They said the trial evidence is heterogeneous in dose, delivery, and population, and that more rigorous large trials are needed.
Other systematic reviews have been more enthusiastic. The 2012 Mickenautsch and Yengopal meta-analysis (International Dental Journal, PMID 22251031) compared xylitol against fluoride and found xylitol non-inferior or slightly superior for caries prevention in several trials. The American Academy of Pediatric Dentistry (AAPD) formally endorses xylitol as an adjunct to fluoride for caries-risk reduction in children with documented high S. mutans burden, recommending 3 to 8 grams per day delivered in at least three separate exposures (gum or lozenges). The European Academy of Paediatric Dentistry (EAPD) maintains a similar position. The American Dental Association (ADA) takes a slightly more cautious stance — acknowledging the evidence as “promising but not definitive” — while still endorsing xylitol products bearing the ADA Seal of Acceptance.
Three findings stand out across the body of dental research and explain why xylitol’s reputation in pediatric dentistry has remained durable even as the Cochrane group remains cautious. First, xylitol works prophylactically in caregivers: a randomized Finnish trial (Söderling et al., Journal of Dental Research, 2000) showed that mothers who chewed xylitol gum during their child’s first two years cut the rate of mother-to-child S. mutans transmission roughly in half, with persisting effects on the children’s caries rates years later. Second, xylitol reduces salivary and plaque counts of cariogenic bacteria — the bacteriologic endpoint is consistent across studies even when the clinical caries endpoint is variable. Third, xylitol gum’s benefits derive at least partly from the chewing itself, which increases salivary flow, buffers plaque acid, and bathes enamel in remineralizing calcium and phosphate. This last mechanism is non-specific and applies to any sugar-free gum, but xylitol has the additional property of being non-fermentable by S. mutans — the next section’s subject.
2. The Mechanism in Streptococcus mutans
To understand why xylitol uniquely targets cavity-causing bacteria, you have to understand the bacterium first. Streptococcus mutans is a Gram-positive coccus that colonizes the human tooth surface in the first 18 to 30 months of life (typically transmitted from a primary caregiver) and persists in dental biofilm for decades thereafter. It is the dominant initiator of dental caries because it does three things exceptionally well: it adheres tenaciously to enamel via glucan polymers it synthesizes from dietary sucrose, it ferments dietary sugars (sucrose, glucose, fructose, lactose) to lactic acid, and it survives and continues fermenting at the resulting low pH that would kill most competitor species. The acid demineralizes tooth enamel; the demineralized enamel becomes a cavity.
What xylitol does to S. mutans is a textbook example of a futile metabolic cycle. S. mutans expresses a fructose-specific phosphoenolpyruvate phosphotransferase system (PTS) that promiscuously imports xylitol along with fructose; once inside the cell, the PTS phosphorylates xylitol to xylitol-5-phosphate, expending one molecule of phosphoenolpyruvate (and therefore one molecule of ATP) per molecule imported. But unlike fructose-6-phosphate, xylitol-5-phosphate cannot enter glycolysis. The bacterium has imported a substrate it cannot metabolize, paid the energetic cost of the import, and is now stuck with a phosphorylated dead-end metabolite that mildly poisons several downstream enzymes (including phosphofructokinase and pyruvate kinase). To survive, the cell expels the xylitol-5-phosphate, dephosphorylating it back to free xylitol in the process — and then promptly re-imports it, paying another ATP. The cycle repeats. The bacterium runs in place metabolically while paying ATP rent.
The result, documented in classic in vitro work by L. Trahan and others (International Dental Journal, 1995; PMID 7607739), is that S. mutans exposed chronically to xylitol shows reduced growth rates, depressed acid production, diminished glucan-mediated adhesion to enamel, and selection pressure for “xylitol-resistant” mutants — mutants that have lost the offending PTS transporter and therefore can no longer import xylitol, but which are also less virulent because the same transporter is involved in normal fructose uptake. In other words, the bacterium can either keep taking up xylitol (and pay the metabolic tax) or it can escape by mutation (and become less cariogenic in the process). Either path reduces the bacterium’s ability to cause cavities.
This mechanism is essentially unique to xylitol among common sweeteners. Sucralose, aspartame, saccharin, and stevia are not metabolized by oral bacteria at all — they are neutral, neither feeding nor inhibiting S. mutans. Sorbitol and mannitol can be slowly fermented by some oral bacteria over weeks of chronic exposure, producing low-grade acid. Erythritol shares some of xylitol’s anti-caries effect (the 2015 Honkala et al. trial in Caries Research reported erythritol superior to xylitol on certain endpoints), but operates through partly different transport and metabolic pathways. Xylitol’s combination of active import, futile phosphorylation, and metabolic dead-ending remains the best-characterized antibacterial mechanism in the dental literature.
One important corollary: the mechanism requires contact between xylitol and oral bacteria. Xylitol baked into a cookie or dissolved into coffee passes through the mouth in seconds and provides essentially no dental benefit. The same xylitol delivered in a chewing gum, lozenge, mint, or oral rinse held in the mouth for 5 to 10 minutes, three to five times per day, delivers the dose where the bacteria live. This frequency-not-just-dose finding is the basis of the AAPD’s “three exposures per day” recommendation.
3. Dose, Frequency, and Real-World Dental Outcomes
The practical dosing literature converges on three numbers. Total daily intake for caries prevention: approximately 5 to 10 grams of xylitol per day, with diminishing returns beyond that and rising gastrointestinal cost beyond about 30 grams. Frequency of exposure: at least three, preferably five, separate exposures distributed across the day, with each exposure ideally following a meal or snack when oral bacteria are most active. Per-exposure dose: roughly 1 to 2 grams of xylitol delivered slowly over 5 to 10 minutes — the duration that a piece of gum or a slowly dissolving mint will typically remain in the mouth.
Concrete examples. A standard piece of 100 percent xylitol-sweetened chewing gum (e.g., Spry, Xlear, EpicDental) contains roughly 1.0 to 1.5 grams of xylitol per piece; five pieces per day delivers 5 to 7.5 grams across five exposures, hitting both the dose and the frequency targets. A xylitol mint or lozenge typically contains 0.5 to 1.0 grams per piece; six to ten pieces per day, distributed across meals and snacks, achieves the same. Xylitol nasal sprays, oral rinses, and toothpastes deliver smaller per-use doses (typically 0.1 to 0.5 grams) but are useful for specific indications — recurrent sinusitis (see Section 4), dry mouth, or as adjuncts to a fluoride toothpaste regimen.
The frequency requirement is the part patients most often miss. A single 8-gram morning dose of xylitol — the entire day’s allotment swallowed at once — does almost nothing for dental caries (and risks GI upset) because the oral bacteria spend the rest of the day in xylitol-free conditions, recover their metabolic momentum, and resume acid production after the next sugar exposure. The same 8-gram total split into five 1.5-gram chewing-gum exposures across the day delivers a five-times-greater functional benefit because the cariogenic bacteria never get a metabolic break.
A useful real-world data point: the Belize Children’s Study (Mäkinen et al., 1995, Journal of Dental Research) randomized 1,277 schoolchildren to xylitol gum, xylitol/sorbitol mixtures, sorbitol-only gum, or no gum for 40 months. Children in the high-frequency xylitol arm developed 62 to 73 percent fewer new cavities than the no-gum control group — one of the largest effect sizes ever reported in a caries-prevention trial. The Belize trial’s strength came partly from its long duration, partly from the dose (~10 g/day in five exposures), and partly from the high baseline caries risk in the population. The same intervention in a low-caries-risk Western adult would be expected to show a much smaller absolute benefit (you can’t prevent cavities the patient was never going to develop), which partly explains why some Cochrane-reviewed trials in adults showed equivocal results.
The takeaway: xylitol works best in high-risk populations (young children with documented elevated S. mutans, caries-prone adults, post-radiation xerostomia patients) when delivered as gum or lozenges several times per day, alongside — not instead of — standard fluoride toothpaste. In low-risk adults practicing good oral hygiene already, the marginal benefit is small.
4. Beyond Cavities — Otitis Media, Sinus, Oral Microbiome
The dental literature is the deepest, but it is not the only literature in which xylitol shows benefit. Three secondary indications have accumulated supporting evidence.
Acute otitis media (AOM) prevention. A landmark Finnish randomized trial by Uhari, Kontiokari, and colleagues (Pediatrics, 1998; PMID 9755259) enrolled 857 day-care children and randomized them to xylitol chewing gum (8.4 g/day in five exposures), xylitol syrup, xylitol lozenges, or controls. The xylitol gum arm showed a 40 percent reduction in the incidence of acute otitis media over the three-month respiratory-illness season, and a corresponding reduction in antibiotic prescriptions. The proposed mechanism: xylitol inhibits Streptococcus pneumoniae growth and adhesion to nasopharyngeal epithelial cells (the same pneumococcus that often migrates up the Eustachian tube to cause middle-ear infection), via a mechanism analogous to its effect on S. mutans. A follow-up Cochrane review (Azarpazhooh et al., 2016) concluded that the AOM-prevention effect is real for healthy day-care children but inconsistent in children with recurrent AOM or those on prophylactic antibiotics. Xylitol gum and lozenges are not recommended below age 2 because of choking risk; xylitol syrup is acceptable in that age group but the AOM benefit is smaller for syrup than for gum.
Chronic rhinosinusitis and sinus rinses. Xylitol nasal sprays and saline-xylitol sinus rinses (Xlear is the dominant US brand) have a smaller but growing evidence base in chronic rhinosinusitis (CRS). The mechanistic premise is two-pronged: xylitol lowers the airway-surface-liquid osmolarity, mobilizing innate antimicrobial peptides (defensins, cathelicidins) that work best in low-salt environments, and it directly inhibits bacterial adhesion to sinonasal epithelium. A 2011 randomized crossover study by Weissman et al. (Otolaryngology — Head and Neck Surgery) reported symptom improvement in CRS patients using xylitol-containing nasal irrigation versus saline-only. The clinical guideline position (American Rhinologic Society 2021) lists xylitol nasal irrigation as a reasonable adjunct in selected CRS patients but not as first-line therapy.
Oral microbiome modulation. Beyond S. mutans, xylitol exposure has been shown to shift the overall composition of the oral microbiome (see the Oral Microbiome hub for the broader systemic-health context). Chronic xylitol gum users show reduced S. mutans, reduced Lactobacillus species, and relative preservation of commensal streptococci (S. sanguinis, S. mitis, S. salivarius) and Veillonella species. This selective pressure favors a less-cariogenic, less-inflammatory plaque ecology — relevant not only to dental caries but to gingivitis, periodontitis, and (the increasingly documented) gut-mouth-brain axis in which oral pathobionts contribute to systemic inflammation and even Alzheimer’s pathogenesis.
Dry mouth (xerostomia) symptomatic relief. Patients with post-radiation xerostomia, Sjögren’s syndrome, or medication-induced dry mouth often report subjective benefit from xylitol lozenges, sprays, and toothpastes. The benefit is partly mechanical (sucking and chewing increase residual salivary flow), partly anti-cariogenic (these patients are at sharply elevated cavity risk because saliva normally buffers acid and remineralizes enamel), and partly comfort-related (xylitol has a mild cooling sensation as it dissolves due to its negative heat of solution).
5. The 2024 Cleveland Clinic Cardiovascular Paper
On June 6, 2024, the European Heart Journal published online a paper titled simply “Xylitol is prothrombotic and associated with cardiovascular risk”, by Marco Witkowski, Ina Nemet, Xinmin S. Li, and colleagues in Stanley L. Hazen’s group at the Cleveland Clinic Lerner Research Institute (PMID 38842092; DOI 10.1093/eurheartj/ehae244). The paper has three distinct components that should be evaluated separately.
The observational cohort. The authors measured fasting plasma xylitol in 3,306 stable U.S. adults presenting for elective cardiac evaluation, then followed them prospectively for incident major adverse cardiovascular events (MACE: nonfatal myocardial infarction, nonfatal stroke, or cardiovascular death) over three years. Patients in the highest quartile of plasma xylitol had a roughly 57 percent higher incidence of MACE compared to the lowest quartile after adjustment for traditional cardiovascular risk factors (hazard ratio 1.57, 95% confidence interval 1.12 to 2.21). The association replicated in a separate European validation cohort. This is an associational signal, not a causal one — high plasma xylitol could be a consequence of cardiovascular disease, a marker of an unmeasured shared cause, or a contributor to cardiovascular disease. The cohort cannot distinguish those possibilities.
The interventional human experiment. To address the causal-or-marker question, the authors enrolled 10 healthy volunteers and gave each a single oral 30-gram xylitol drink — an amount approximating the xylitol load in a single large “keto” baked good, two large servings of sugar-free ice cream, or roughly a half-cup of bulk xylitol used in home baking. Plasma xylitol concentrations rose approximately 1,000-fold above baseline within 30 minutes, peaked at one to two hours, and remained substantially elevated for more than four hours. During this elevated-xylitol window, the volunteers’ circulating platelets showed measurable increases in ex vivo activation markers and in their tendency to aggregate in response to physiologically relevant agonists (collagen, ADP, thrombin) at sub-threshold doses that ordinarily would have produced little response. The platelet effect was present in every subject — there were no nonresponders — and resolved as plasma xylitol returned toward baseline. This is the strongest piece of the paper, because it demonstrates a direct dose-response link between an acute xylitol load and a clinically relevant prothrombotic phenotype in humans.
The mouse model. To establish biological plausibility for the long-term cardiovascular endpoint, the authors used a standard mouse arterial-injury model in which the carotid artery is briefly damaged with ferric chloride (which exposes subendothelial collagen and triggers platelet adhesion) and the time to vessel occlusion is measured. Mice pretreated with xylitol developed arterial thrombosis significantly faster than vehicle-treated controls. The effect was abolished by aspirin, consistent with the prothrombotic mechanism acting through the platelet pathway. The mouse model is not perfect — mouse plasma xylitol levels differ from human, and the ferric chloride injury is not literally an atherosclerotic plaque rupture — but it adds a layer of mechanistic confidence that the human findings are not artifactual.
Taken together, the three components mean: xylitol exposure at a single 30-gram dose primes human platelets to clump in response to subthreshold triggers; high habitual plasma xylitol is associated with a 57 percent higher rate of major cardiovascular events over three years; and the platelet-priming effect produces measurable thrombosis in animal models. The chain of evidence is not complete — only a long-term randomized trial of xylitol versus placebo on incident cardiovascular events would close it — but the chain is substantially more rigorous than a typical “observational study suggests” headline.
6. How Xylitol Activates Platelets — The Mechanism
The Hazen group has been working on small molecules that prime platelet activation since at least 2017, when they reported a similar phenotype for choline-derived trimethylamine-N-oxide (TMAO), the gut-microbiome metabolite that arises from dietary choline, L-carnitine, and phosphatidylcholine. The xylitol mechanism appears to be related but mechanistically distinct.
Direct platelet membrane interaction. The 2024 paper’s in vitro experiments show that xylitol added to washed human platelets at concentrations corresponding to the post-30-gram-dose plasma peak produces a small but reproducible baseline shift toward an “activatable” state — the platelets are not aggregated, but they have lowered their threshold for aggregation in response to canonical agonists. The effect appears to involve a direct interaction between xylitol and platelet-surface receptors, possibly the same family of carbohydrate-sensing receptors (Siglecs, C-type lectin receptors) that recognize sugar moieties on bacterial surfaces in normal immune surveillance. The receptor target has not yet been definitively identified.
Subthreshold agonist amplification. The clinically important phenotype is not that xylitol alone causes platelets to aggregate — it doesn’t. It is that xylitol amplifies the response to physiologically present clotting stimuli. Collagen exposed during minor endothelial injury, ADP released from injured red blood cells, thrombin generated by tissue factor exposure — these signals are present constantly at low levels in any human circulation. A primed platelet population responds to these subthreshold signals when an unprimed population would not, and the result is more frequent micro-aggregates, more frequent minor thrombi, and ultimately (the cohort data suggest) more frequent macroscopic thrombotic events.
Time course. The platelet-priming effect is acute, dose-dependent, and reversible. It rises within 30 minutes of an oral xylitol load, peaks at 1 to 2 hours, and resolves over 4 to 8 hours as plasma xylitol returns to baseline. This time course matches the urinary excretion of xylitol in humans (xylitol is excreted unchanged in urine to a substantial extent, with the rest metabolized via the pentose phosphate pathway primarily in the liver). The implication: a single occasional xylitol exposure produces a transient prothrombotic window of a few hours’ duration; chronic high-frequency exposure would maintain plasma xylitol at moderately elevated levels and could produce a sustained prothrombotic state.
Why this matters clinically. Most clinical cardiovascular events do not happen because a healthy person spontaneously generates a giant clot. They happen because an atherosclerotic plaque ruptures or erodes, exposing subendothelial collagen and tissue factor to circulating platelets at a moment when those platelets are either primed or unprimed for response. A primed platelet population that responds vigorously to the rupture produces an occlusive thrombus; an unprimed population that responds slowly may allow the lesion to heal without occlusion. The xylitol mechanism, in other words, doesn’t cause heart attacks — it tilts the playing field by which an existing atherosclerotic lesion does or doesn’t become an occlusive event. This is precisely the kind of mechanism in which population-level exposure (millions of people drinking xylitol-sweetened products) could produce a measurable population-level signal in MACE incidence without any individual user being able to point to xylitol as “the cause” of their event.
7. The Erythritol Precedent (Same Lab, 2023)
The xylitol paper does not stand alone. In February 2023, the same Hazen group published in Nature Medicine (PMID 36849732; DOI 10.1038/s41591-023-02223-9) a methodologically nearly identical study of erythritol — another sugar alcohol, even more aggressively marketed than xylitol as “safe” and “zero glycemic.” The erythritol paper used the same three-component design: a large observational cohort showing association between high plasma erythritol and incident MACE; an acute oral 30-gram intervention in healthy volunteers showing plasma erythritol rising massively above baseline and remaining elevated for hours; and ex vivo and in vivo evidence that erythritol primes platelets for activation. The erythritol cardiovascular signal was, if anything, slightly stronger than the subsequent xylitol signal.
The 2023 erythritol paper was met with the predictable reactions. Industry groups and several academic critics pointed out that erythritol is produced endogenously by the body in modest amounts, so elevated plasma erythritol might be a marker of metabolic dysregulation (specifically of pentose phosphate pathway flux) rather than a consequence of dietary intake — the “reverse causation” objection. The Hazen group’s response was that the interventional 30-gram dose unambiguously demonstrated that exogenous erythritol produces the platelet phenotype, so reverse causation cannot fully explain the cohort findings. The same objection-and-response pattern is now playing out for xylitol.
The pattern of two structurally related sugar alcohols, studied by the same lab with the same methodology, producing the same prothrombotic signal in independent cohorts and the same platelet phenotype after an acute intervention, is the most important contextual fact in evaluating the xylitol findings. This is not a one-off observation. It is a class effect emerging across sugar alcohols, and the implication is that the marketing claim “safer than sugar” is being challenged not because xylitol or erythritol are toxic in any conventional sense, but because their cardiovascular effects appear to operate through a pathway that traditional safety evaluation (acute toxicity, organ damage, carcinogenicity) was not designed to detect.
Two important nuances limit how broadly this pattern should be extrapolated. First, not every non-nutritive sweetener has been shown to share the platelet phenotype. The Hazen group has not yet published comparable data on sorbitol, mannitol, maltitol, allulose, sucralose, aspartame, saccharin, or stevia; in the absence of that data, the prothrombotic concern should not be projected across the entire sweetener category. Second, the magnitude matters. The dietary xylitol exposures associated with elevated MACE in the cohort were in the upper range of habitual consumption (heavy users of xylitol baked goods, ice cream, gum, and beverages). A handful of pieces of xylitol gum per day — the dose the dental literature recommends — produces a much smaller plasma xylitol excursion than a 30-gram bolus, and the cardiovascular implications at that dose level are not well characterized.
8. “Prothrombotic, Not a Blood Thinner” — The Distinction That Matters
The language of cardiovascular pharmacology is precise for good reason, and one of the most common public-facing misunderstandings about the 2024 xylitol paper is the assumption that xylitol acts as a “blood thinner.” It does not. The Hazen paper’s conclusion is the opposite. The word that appears in the title and throughout the paper is prothrombotic, which is the technical antonym of antithrombotic. Understanding the distinction is essential for any patient or clinician thinking about xylitol exposure.
Antithrombotic drugs reduce the body’s ability to form a clot. They come in two categories: anticoagulants (warfarin, the direct oral anticoagulants apixaban, rivaroxaban, edoxaban, dabigatran, and parenteral heparins) that inhibit the coagulation cascade by blocking specific clotting factors; and antiplatelet agents (aspirin, clopidogrel, ticagrelor, prasugrel) that prevent platelets from aggregating. Both categories reduce the formation of clots and are prescribed to patients at elevated risk of thrombotic events (atrial fibrillation, post-myocardial-infarction, post-stent, mechanical heart valves, venous thromboembolism). They carry a corresponding risk of bleeding — the inevitable trade-off of reduced clotting capacity.
Prothrombotic exposures, by contrast, increase the body’s clotting tendency. Estrogen-containing contraceptives, certain cancer chemotherapies, smoking, immobilization, dehydration, surgery, and now — the 2024 data suggest — high-dose xylitol exposure all sit in this category. None of these is acutely dangerous in a typical person. All of them shift the balance of clot formation and clot dissolution toward formation, and the clinical consequences emerge in populations rather than individuals: more clots per 100,000 people per year, more myocardial infarctions per 100,000 person-years of exposure, more strokes.
The clinical implications of the distinction are large. A patient taking aspirin or clopidogrel for cardiovascular secondary prevention is already on a daily antiplatelet drug. Adding a prothrombotic dietary exposure (high-dose xylitol) does not directly negate the antiplatelet drug, but it does work against it — the same way that smoking works against antihypertensive therapy. A patient with established atrial fibrillation on an anticoagulant is not in the population the xylitol study examined, but the underlying logic suggests prudent caution. A patient with no cardiovascular history, no atherosclerotic disease, and no risk factors who chews a few pieces of xylitol gum per day is at the lower-exposure, lower-risk end of the curve and is probably not in the population whose MACE risk was elevated 57 percent in the Hazen cohort.
The framing that xylitol acts as a blood thinner — sometimes promoted on social media in the wake of confused early reporting on the 2024 paper — is therefore not just wrong, it is dangerously inverted. The actual finding is that xylitol promotes clotting, not that it prevents it. Patients should not use xylitol as a substitute for prescribed antithrombotic therapy under any circumstances, and the casual addition of high-dose xylitol to the diet of a patient with significant cardiovascular risk is, on current evidence, prudent to avoid.
9. Dose and Exposure — Chewing Gum vs Baking Bulk
The single most important variable in deciding whether the 2024 cardiovascular data should change a person’s xylitol behavior is the dose. The Hazen interventional protocol used 30 grams of xylitol in a single drink. This produced an approximate thousand-fold rise in plasma xylitol concentration sustained for hours. The dental-prevention dose recommended by the AAPD — 5 to 10 grams per day distributed across five exposures of 1 to 2 grams each — produces a substantially smaller and more transient plasma excursion. The question of whether the platelet-priming effect is meaningful at the dental dose remains open.
To make this concrete, here are typical xylitol doses in common products:
- One piece of 100% xylitol chewing gum: approximately 1.0–1.5 g xylitol. Five pieces/day = 5–7.5 g/day in five exposures.
- One xylitol mint or lozenge: approximately 0.5–1.0 g xylitol. Eight pieces/day = 4–8 g/day distributed.
- One serving of “keto” baked good sweetened with xylitol: 5–15 g xylitol per serving (highly variable by recipe).
- One half-cup of sugar-free ice cream sweetened with xylitol: 15–25 g xylitol.
- One scoop of bulk xylitol used as a 1:1 sugar replacement in coffee/tea: 4–6 g xylitol per typical “teaspoon” (xylitol is denser than sugar).
- One full home-baking cup of bulk xylitol distributed across a recipe yielding 8 servings: approximately 25–30 g xylitol per serving — the same as the Hazen intervention dose, in a single eating occasion.
The exposure pattern of a person who chews 4 pieces of xylitol gum per day after meals is fundamentally different from the exposure pattern of a person who eats a daily slice of xylitol-sweetened keto bread alongside a xylitol-sweetened ice cream and a xylitol-sweetened coffee creamer. The first person is operating in the dose range the dental literature studied. The second person is operating in the dose range the Hazen cardiovascular paper studied. Both might be true to themselves as “moderate xylitol users,” but their plasma xylitol exposures are an order of magnitude apart.
For readers trying to translate the 2024 data into a personal practice, the rough guidance that emerges is: treat dental xylitol (gum, mints, lozenges, toothpaste, nasal/sinus rinses) as a low-exposure category with established dental benefits and as-yet-unclear long-term cardiovascular implications. Treat bulk xylitol used in baking, sugar-free beverages, and large servings of low-carbohydrate desserts as a high-exposure category with established cardiovascular concern. Until a randomized long-term trial settles the question, this dose-stratified approach is the most defensible synthesis of the evidence.
10. Pet Toxicity — A Separate, Serious Warning
One xylitol-related health risk is not subtle, not controversial, and not dose-stratified: xylitol is acutely and severely toxic to dogs, and toxic at lower severity to ferrets and some other species. The toxicity mechanism is entirely different from the human cardiovascular concern and stems from a species difference in pancreatic islet response to xylitol.
In humans, ingested xylitol produces only a minimal insulin response — this is the entire basis of its “low glycemic” reputation. In dogs, the same xylitol produces an enormous, rapid, and dose-dependent insulin release, three to seven times the insulin response to an equivalent glucose load. The resulting hypoglycemia can be severe and rapidly fatal. A dose as small as 0.1 g per kilogram of body weight can produce clinically significant hypoglycemia in dogs. A dose above 0.5 g/kg can additionally produce acute hepatic failure via a mechanism that is not fully understood but appears to involve overwhelming oxidative stress in hepatocytes and ATP depletion.
To make this concrete: a 20-pound (9 kg) dog that consumes a single 1.5-gram piece of xylitol chewing gum has reached approximately 0.17 g/kg — into the severe-hypoglycemia range. Two pieces and the same dog is into the hepatotoxicity range. A typical pack of xylitol gum contains 10 to 15 pieces; the entire pack is a probably-fatal exposure for that dog. Smaller dogs are at correspondingly higher per-piece risk. The ASPCA Animal Poison Control Center receives several thousand xylitol exposure calls per year, with sugar-free gum, sugar-free peanut butter (some brands now contain xylitol), and home-baked goods using bulk xylitol as the most common sources.
The clinical course in dogs: hypoglycemia within 30 minutes to several hours of ingestion (vomiting, weakness, ataxia, seizures, coma, death); delayed acute liver failure 12 to 72 hours after ingestion, sometimes occurring despite apparently successful initial hypoglycemia management. Treatment in a veterinary emergency setting is dextrose infusion, hepatoprotective therapy (N-acetylcysteine, S-adenosylmethionine), and supportive care. Survival is the rule with prompt veterinary intervention; death is the rule without it.
The two practical implications: households with dogs should treat xylitol products as they would treat prescription medications — stored above counter level, never left on bedside tables or in handbags accessible to a curious dog. Sugar-free peanut butter is a particular hazard because peanut butter is the standard pill-hiding food for dogs and the bait-of-choice in food puzzles; reading the label every time is essential, as several major brands have quietly reformulated with xylitol in recent years. Cats are less susceptible (their islet cells respond differently) but ferrets are highly susceptible; rabbits, rodents, and birds are variable.
11. GI Tolerance and Other Adverse Effects
The most common acute adverse effect of human xylitol consumption is gastrointestinal upset — bloating, abdominal cramping, flatulence, and osmotic diarrhea. The mechanism: xylitol is incompletely absorbed in the small intestine, so a substantial fraction reaches the colon, where it draws water osmotically and where colonic bacteria slowly ferment it to short-chain fatty acids, methane, and hydrogen. The result is the classic “sugar alcohol gut” symptom complex.
Individual GI tolerance varies enormously. Some people tolerate 40 g/day with no symptoms; others develop diarrhea at 10 g/day. The typical dose-response threshold for symptoms is around 30 to 50 g/day in a single sitting, or 50 to 100 g/day distributed; tolerance generally improves over two to four weeks of regular consumption as the colonic microbiome adapts. Children are generally more sensitive than adults on a per-kilogram basis. Patients with irritable bowel syndrome, particularly the FODMAP-sensitive subtype, are markedly more sensitive and often cannot tolerate even small doses of xylitol — one reason xylitol is excluded from the low-FODMAP diet.
Beyond GI tolerance, the adverse-effect literature is short. Allergic reactions are rare but documented; isolated case reports of urticaria and angioedema after xylitol exposure exist but the cumulative incidence is very low. Drug interactions are minimal; xylitol does not significantly affect hepatic cytochrome P450 enzymes and has no established interaction with antiplatelet, anticoagulant, statin, or antihypertensive medications. Pregnancy and breastfeeding data are limited; xylitol crosses the placenta at small concentrations and is present in breast milk at low levels with no documented adverse infant outcomes. The American College of Obstetricians and Gynecologists does not warn against modest xylitol use in pregnancy.
The cardiovascular concern from the 2024 Hazen paper is, in this context, the most clinically significant adverse-effect signal in xylitol’s 40-year history of widespread human use — not because it is acutely dangerous, but because it operates at chronic high-exposure levels in ways that the prior safety literature was not powered to detect. The standard GRAS framework asks “is this acutely toxic?” The xylitol cardiovascular data ask “does chronic exposure shift population-level event rates?” Different question, different answer.
Practical Synthesis — Who Should and Shouldn’t Use Xylitol
Pulling the dental and cardiovascular literatures together, the following risk-stratified synthesis is the most defensible practical position in light of the 2024 evidence.
Probably a net benefit at recommended dental doses (~5 to 10 g/day in 3 to 5 exposures via gum, mints, lozenges, or oral rinses):
- Children age 2+ with documented high caries risk or elevated S. mutans burden, particularly those whose parents or siblings have significant caries history.
- Pregnant women planning to reduce mother-to-child S. mutans transmission to their newborns.
- Day-care-age children at elevated risk of recurrent acute otitis media (Uhari indication).
- Adults with caries-prone dentition, post-radiation xerostomia, Sjögren’s syndrome, or medication-induced dry mouth.
- Patients undergoing orthodontic treatment with fixed appliances, which dramatically increase caries risk by trapping food and plaque.
Probably a net concern at high bulk-baking and beverage doses (~25 to 50+ g/day via bulk xylitol in baking, sugar-free ice cream/desserts, “keto” foods, sweetened beverages):
- Adults with established atherosclerotic cardiovascular disease, prior myocardial infarction, prior stroke, peripheral artery disease, or carotid disease.
- Adults with multiple unmodified cardiovascular risk factors (diabetes, hypertension, dyslipidemia, smoking history, family history of premature cardiovascular disease).
- Patients with atrial fibrillation, mechanical heart valves, or prior venous thromboembolism — not because xylitol is contraindicated by drug interaction with their anticoagulant, but because shifting the thrombotic balance in either direction warrants caution in this population.
- Patients in the perioperative period (any surgery within 30 days), where transient prothrombotic states already elevate baseline thrombotic risk.
Probably an absolute warning:
- Households with dogs, ferrets, or other susceptible pets — xylitol products should be stored well out of reach, and sugar-free peanut butter and similar pet-bait foods should be label-checked.
- Patients with significant IBS-FODMAP intolerance — the GI burden typically outweighs any benefit.
The middle case — healthy adult without significant cardiovascular risk, using xylitol gum or mints at recommended dental doses — is the one in which the current evidence is most ambiguous. The dental benefit is real. The cardiovascular concern at this exposure level is unproven (it has been demonstrated at the 30-gram acute dose, but not specifically excluded or confirmed at the 5-to-10-gram divided daily dose). Reasonable clinicians and informed patients can disagree about how to weigh the two.
The most important framing — and the one most often missed in popular discussion of the 2024 paper — is that this is a dose-response question, not a binary safe/unsafe question. The dental dose and the cardiovascular dose are an order of magnitude apart, and conflating them produces both unwarranted alarm (patients abandoning a useful dental tool) and unwarranted complacency (patients consuming bulk xylitol in baking without considering the cardiovascular signal). Treat them separately. Read the label. Know how much you’re actually consuming.
References & Further Reading
Primary Cardiovascular Studies (Hazen Group)
- Witkowski M, Nemet I, Li XS, et al. Xylitol Is Prothrombotic and Associated with Cardiovascular Risk. European Heart Journal. 2024;45(27):2439–2452. PMID 38842092. doi:10.1093/eurheartj/ehae244
- Witkowski M, Nemet I, Alamri H, et al. The Artificial Sweetener Erythritol and Cardiovascular Event Risk. Nature Medicine. 2023;29(3):710–718. PMID 36849732. doi:10.1038/s41591-023-02223-9
- Zhu W, Gregory JC, Org E, et al. Gut Microbial Metabolite TMAO Enhances Platelet Hyperreactivity and Thrombosis Risk. Cell. 2016;165(1):111–124. PMID 26972052. doi:10.1016/j.cell.2016.02.011 (the Hazen group’s earlier mechanistic paper on small-molecule platelet priming — methodologic ancestor of the xylitol and erythritol studies).
Dental and Caries-Prevention Literature
- Riley P, Moore D, Ahmed F, et al. Xylitol-Containing Products for Preventing Dental Caries in Children and Adults. Cochrane Database of Systematic Reviews. 2015;(3):CD010743. PMID 25809586. doi:10.1002/14651858.CD010743.pub2
- Mickenautsch S, Yengopal V. Anticariogenic Effect of Xylitol Versus Fluoride — A Quantitative Systematic Review of Clinical Trials. International Dental Journal. 2012;62(1):6–20. — Search PubMed. doi:10.1111/j.1875-595X.2011.00086.x
- Mäkinen KK. Sugar Alcohols, Caries Incidence, and Remineralization of Caries Lesions: A Literature Review. International Journal of Dentistry. 2010;2010:981072. — Search PubMed. doi:10.1155/2010/981072
- Mäkinen KK, Bennett CA, Hujoel PP, et al. Xylitol Chewing Gums and Caries Rates: A 40-Month Cohort Study. Journal of Dental Research. 1995;74(12):1904–1913. — Search PubMed. doi:10.1177/00220345950740121501 (the Belize Children’s Study).
- Söderling E, Isokangas P, Pienihäkkinen K, Tenovuo J. Influence of Maternal Xylitol Consumption on Acquisition of Mutans Streptococci by Infants. Journal of Dental Research. 2000;79(3):882–887. PMID 10765964. doi:10.1177/00220345000790031601
- Milgrom P, Ly KA, Roberts MC, et al. Mutans Streptococci Dose Response to Xylitol Chewing Gum. Journal of Dental Research. 2006;85(2):177–181. PMID 16434738. doi:10.1177/154405910608500214
- Trahan L. Xylitol: A Review of Its Action on Mutans Streptococci and Dental Plaque — Its Clinical Significance. International Dental Journal. 1995;45(1 Suppl 1):77–92. — Search PubMed
- Maguire A, Rugg-Gunn AJ. Xylitol and Caries Prevention — Is It a Magic Bullet? British Dental Journal. 2003;194(8):429–436. PMID 12778091. doi:10.1038/sj.bdj.4810022
- Honkala S, Runnel R, Mäkinen KK, et al. Effect of Erythritol and Xylitol on Dental Caries Prevention in Children. Caries Research. 2014;48(5):482–490. PMID 24852946. doi:10.1159/000358399
- Schäfer A, Adler I, Trompelt J, et al. Xylitol and Caries Prevention — A Systematic Review. BMC Oral Health. 2020;20(1):288. — Search PubMed. doi:10.1186/s12903-020-01233-0
Otitis Media, Sinus, and Oral Microbiome
- Uhari M, Kontiokari T, Niemelä M. A Novel Use of Xylitol Sugar in Preventing Acute Otitis Media. Pediatrics. 1998;102(4 Pt 1):879–884. PMID 9755259. doi:10.1542/peds.102.4.879
- Azarpazhooh A, Lawrence HP, Shah PS. Xylitol for Preventing Acute Otitis Media in Children up to 12 Years of Age. Cochrane Database of Systematic Reviews. 2016;(8):CD007095. PMID 27486835. doi:10.1002/14651858.CD007095.pub3
- Kontiokari T, Uhari M, Koskela M. Effect of Xylitol on Growth of Nasopharyngeal Bacteria In Vitro. Antimicrobial Agents and Chemotherapy. 1995;39(8):1820–1823. PMID 7486925. doi:10.1128/aac.39.8.1820
- Weissman JD, Fernández F, Hwang PH. Xylitol Nasal Irrigation in the Management of Chronic Rhinosinusitis: A Pilot Study. Laryngoscope. 2011;121(11):2468–2472. PMID 21994147. doi:10.1002/lary.22176
Pet Toxicity (Veterinary)
- Dunayer EK, Gwaltney-Brant SM. Acute Hepatic Failure and Coagulopathy Associated with Xylitol Ingestion in Eight Dogs. Journal of the American Veterinary Medical Association. 2006;229(7):1113–1117. PMID 17014359. doi:10.2460/javma.229.7.1113
- Dunayer EK. Hypoglycemia Following Canine Ingestion of Xylitol-Containing Gum. Veterinary and Human Toxicology. 2004;46(2):87–88. — Search PubMed
- Cope RB. A Screening Study of Xylitol Binding In Vitro to Activated Charcoal. Veterinary and Human Toxicology. 2004;46(6):336–337. — Search PubMed
- Schmid RD, Hovda LR. Acute Hepatic Failure in a Dog after Xylitol Ingestion. Journal of Medical Toxicology. 2016;12(2):201–205. — Search PubMed. doi:10.1007/s13181-015-0518-4
Background & Mechanism
- Mäkinen KK. History, Safety, and Dental Properties of Xylitol. Caries Research. 2010;44(Suppl 1):1–19. — Search PubMed
- Salli K, Lehtinen MJ, Tiihonen K, Ouwehand AC. Xylitol’s Health Benefits beyond Dental Health: A Comprehensive Review. Nutrients. 2019;11(8):1813. PMID 31390800. doi:10.3390/nu11081813
- Bonifait L, Grenier D. Cranberry Polyphenols: Potential Benefits for Dental Caries and Periodontal Disease. Journal of the Canadian Dental Association. 2010;76:a130. PMID 20943032 (background on biofilm-targeted approaches to caries prevention).
- Rafeek RAM, Carrington C, Gomez A, et al. Xylitol and Sorbitol Effects on the Microbiome of Saliva and Plaque. Journal of Oral Microbiology. 2019;11(1):1536181. — Search PubMed. doi:10.1080/20002297.2018.1536181
- Janakiram C, Deepan Kumar CV, Joseph J. Xylitol in Preventing Dental Caries: A Systematic Review and Meta-Analyses. Journal of Natural Science, Biology and Medicine. 2017;8(1):16–21. PMID 28250669. doi:10.4103/0976-9668.198344
- Witkowski M, Weeks TL, Hazen SL. Gut Microbiota and Cardiovascular Disease. Circulation Research. 2020;127(4):553–570. PMID 32762536. doi:10.1161/CIRCRESAHA.120.316242 (broader Hazen-group review on diet-derived small molecules and CV disease).
Regulatory and Position Statements
- U.S. Food and Drug Administration. Select Committee on GRAS Substances (SCOGS) Opinion: Xylitol. SCOGS-Report Number 109. FDA SCOGS Database
- European Food Safety Authority Panel on Food Additives. Re-Evaluation of Xylitol (E 967) as a Food Additive. EFSA Journal. 2018;16(3):5158. doi:10.2903/j.efsa.2018.5158
- American Academy of Pediatric Dentistry. Policy on the Use of Xylitol. AAPD Reference Manual of Pediatric Dentistry. 2023–2024. aapd.org
- American Dental Association Council on Scientific Affairs. ADA Statement on Xylitol and Dental Caries Prevention. Journal of the American Dental Association. Various position updates. ada.org
- U.S. Food and Drug Administration. Xylitol and Your Dog: Danger, Paws Off. FDA Consumer Update. fda.gov consumer update
Live PubMed Searches
- PubMed: xylitol cardiovascular risk
- PubMed: xylitol platelet activation
- PubMed: xylitol thrombosis
- PubMed: xylitol dental caries
- PubMed: xylitol Streptococcus mutans
- PubMed: xylitol otitis media
- PubMed: xylitol sinusitis nasal
- PubMed: xylitol chewing gum RCT
- PubMed: xylitol oral microbiome
- PubMed: xylitol dog toxicity hypoglycemia
- PubMed: xylitol pharmacokinetics humans
- PubMed: erythritol cardiovascular Hazen
- PubMed: sugar alcohols caries systematic review
- PubMed: xylitol pregnancy mutans streptococci
- PubMed: non-nutritive sweeteners cardiovascular disease
- PubMed: xylitol IBS FODMAP GI tolerance
Related Articles on MyHealthcare.com
- Artificial Sweeteners — Hub Page
- Aspartame
- Sucralose
- Acesulfame Potassium
- Oral Microbiome
- Cardiology
- Cardiovascular Disease
- Atherosclerosis
- Coronary Artery Disease
- Stroke
- Cholesterol Management
- Deep Vein Thrombosis
- Thrombocytopenia
- Disseminated Intravascular Coagulation
- Sinusitis
- Sjögren’s Syndrome
- Coagulation Panel
- Inflammatory Markers
- Lipid Panel
- ApoB
- Lipoprotein(a)
- Coronary Calcium Score
- April 12, 2026 News
- April 27, 2026 — Gut, Brain, and the Bacteria Between Them
- May 11, 2026 — Methylene Blue and the Kidneys