Apolipoprotein B (ApoB): Why It May Predict Your Heart Attack Better Than LDL Cholesterol
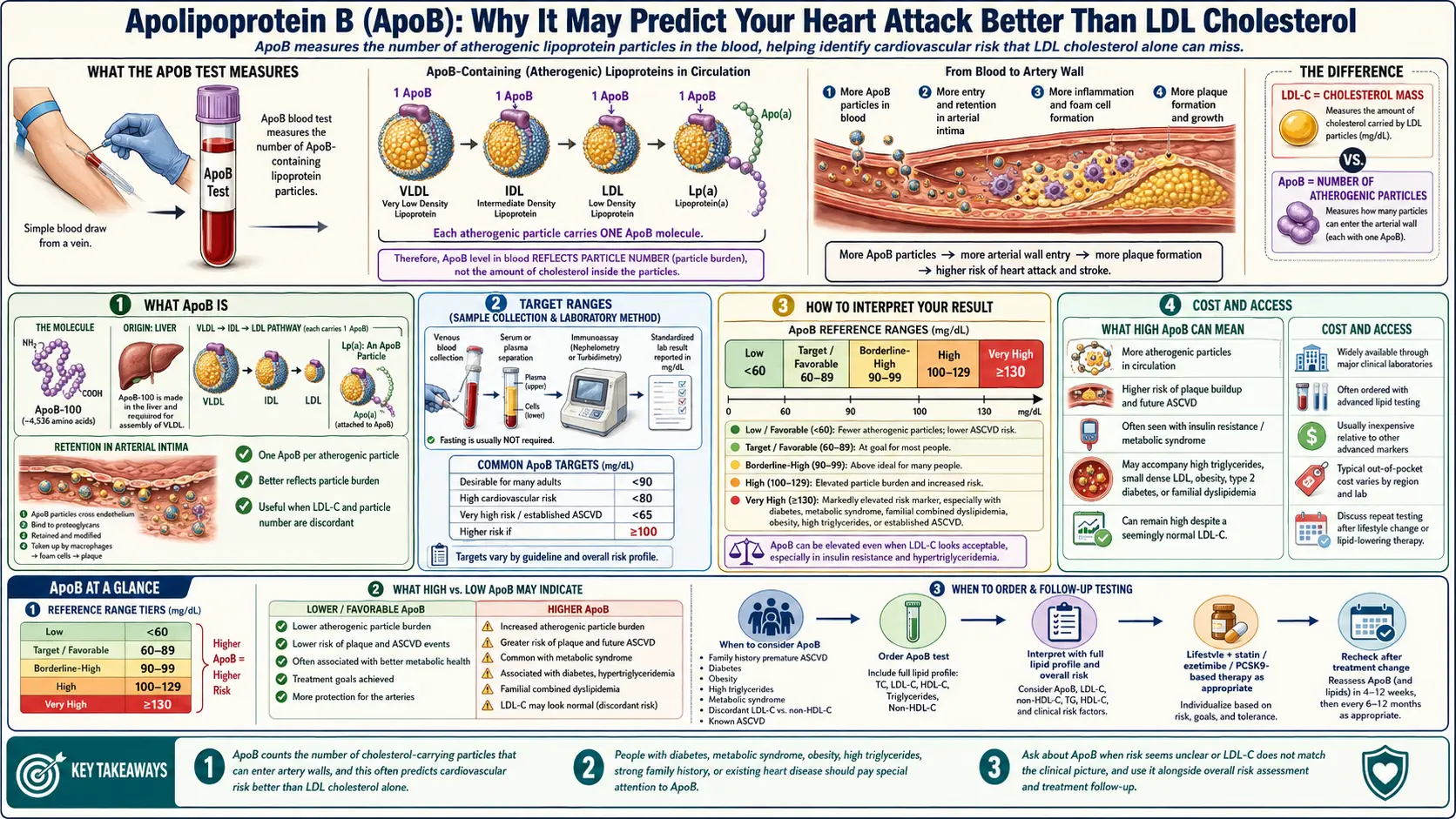
The standard lipid panel measures LDL cholesterol — the concentration of cholesterol molecules inside low-density lipoprotein particles. What it does not measure is the number of atherogenic lipoprotein particles themselves. Over the past two decades, evidence has mounted that particle number is a more accurate predictor of cardiovascular events than particle cholesterol content. That number is captured by a single inexpensive blood test: apolipoprotein B (ApoB). Each atherogenic lipoprotein particle — LDL, VLDL, IDL, Lp(a), and chylomicron remnants — carries exactly one ApoB molecule, so the ApoB concentration in blood equals the number of particles that can penetrate an artery wall and trigger atherosclerosis.
ApoB has been championed in the public sphere by Dr. Peter Attia and others as the single most important lipid biomarker. Major cardiology societies increasingly recommend it alongside or instead of LDL-C, and in discordant cases (where LDL-C and ApoB disagree) ApoB is the better predictor. This article explains what ApoB is, when to order it, how to interpret it, and what to do if it’s elevated.
Table of Contents
- What ApoB Is
- Why ApoB Beats LDL Cholesterol
- Target Ranges
- Who Should Order the Test
- How to Interpret Your Result
- How to Lower ApoB
- Cost and Access
- Connections
- Featured Videos
What ApoB Is
Apolipoprotein B is a large structural protein that wraps around lipoprotein particles that carry triglycerides and cholesterol through the bloodstream. There are two forms — ApoB-48 on chylomicrons (dietary fat transport) and ApoB-100 on liver-derived particles. The standard ApoB lab test measures the total; more than 90 percent of the signal in fasting adults comes from ApoB-100-containing atherogenic particles. One particle equals one ApoB molecule, so measuring ApoB directly counts how many potentially arterial-damaging particles are in circulation.
Why ApoB Beats LDL Cholesterol
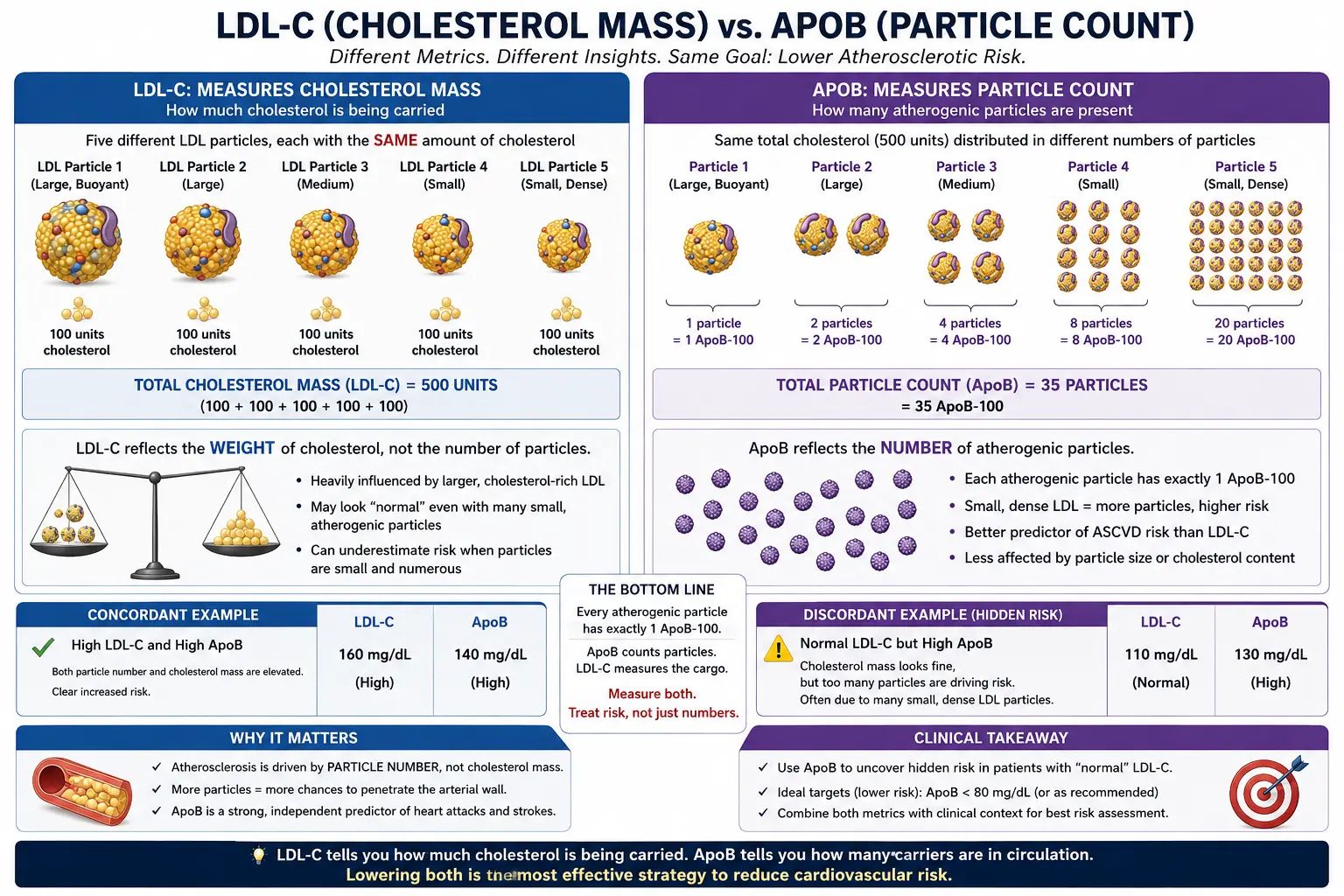
Two people can have identical LDL cholesterol of 120 mg/dL but very different particle numbers. Person A may have a small number of large, cholesterol-rich particles. Person B may have many small, cholesterol-poor particles carrying the same total cholesterol. Person B has far higher ApoB and far higher cardiovascular risk, because it is the particle count — not the total cholesterol they carry — that drives artery-wall penetration and plaque formation. This discordance between LDL-C and ApoB is especially common in insulin resistance, metabolic syndrome, type 2 diabetes, and in people on statins (where LDL-C falls more than particle number). Large prospective studies, including the MESA and EPIC cohorts, consistently show ApoB outperforms LDL-C for event prediction.
Target Ranges
- <60 mg/dL — Optimal for people with established cardiovascular disease or very high lifetime risk.
- <80 mg/dL — Target for primary prevention in high-risk adults (family history, diabetes, metabolic syndrome).
- <90 mg/dL — Population target consistent with roughly the 20th percentile of adult values.
- >130 mg/dL — Clearly elevated; lifestyle and typically pharmacological intervention warranted.
The lower-is-better principle applies across the whole range. Lifetime ApoB exposure — area under the curve — is what drives atherosclerosis.
Who Should Order the Test
ApoB is valuable for:
- Anyone with a family history of premature cardiovascular disease.
- People with metabolic syndrome, type 2 diabetes, insulin resistance, fatty liver, or PCOS.
- Anyone whose LDL-C and triglycerides disagree (low LDL-C with high triglycerides is a high-discordance pattern).
- Patients on statin therapy — to verify particle-number reduction, not just LDL-C.
- Adults following lower-carb, keto, or high-fat diets, which occasionally raise ApoB even when LDL-C is stable.
- Longevity-focused patients wanting the most predictive single lipid marker.
How to Interpret Your Result
ApoB is not fasting-sensitive, but modest fasting is still recommended for paired lipid testing. Interpret ApoB alongside your Lipid Panel, Lp(a), and — if available — a coronary calcium score. A single elevated ApoB is a signal; a pattern over years drives risk. Small reductions compound. If you are on statin or ezetimibe therapy, ApoB is the cleanest way to confirm actual particle-number reduction.
How to Lower ApoB
Lifestyle interventions:
- Reduce dietary saturated fat to <7% of calories; replace with monounsaturated fats and omega-3 fish fats.
- Increase viscous soluble fiber (oats, psyllium, beans, flax) — 10–25 g per day lowers ApoB by 5–10%.
- Weight loss of >5% reduces ApoB meaningfully.
- Aerobic exercise 150+ minutes/week.
- Alcohol moderation.
Pharmacological options:
- Statins — lower ApoB by 30–50%.
- Ezetimibe — additional 10–20% reduction.
- PCSK9 inhibitors (evolocumab, alirocumab) — up to 60% reduction in addition to statins.
- Bempedoic acid — statin-alternative for intolerance.
- Inclisiran — twice-yearly injectable PCSK9 small interfering RNA.
Cost and Access
ApoB testing costs roughly $15–30 direct-to-consumer through services like Quest or LabCorp and is typically covered by insurance when ordered by a clinician. The test is widely available at any standard lab. If your clinician is unfamiliar, you can request it by name — the turnaround is the same day.
Research Papers and References
The following are curated PubMed literature searches covering the evidence base for ApoB testing, interpretation, and clinical management. Each link opens a live, filtered PubMed query so the results stay current as new studies are indexed.
- Apolipoprotein B cardiovascular risk — PubMed literature search
- ApoB vs LDL discordance — PubMed literature search
- ApoB particle number — PubMed literature search
- ApoB Mendelian randomization — PubMed literature search
- Non-HDL vs ApoB — PubMed literature search
- ApoB statin response — PubMed literature search
- ApoB insulin resistance — PubMed literature search
- ApoB ASCVD risk — PubMed literature search
- ApoB Canadian Cardiovascular Society — PubMed literature search
- ApoB PCSK9 inhibitor — PubMed literature search
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- Lipid Panel
- Coronary Calcium Score
- Lipoprotein(a)
- Atherosclerosis
- Coronary Artery Disease
- Cardiovascular Disease
- Insulin Resistance
- Metabolic Syndrome
- CAC vs Other Cardiac Tests
- Statin Threshold and CAC
- Soft Plaque and CAC Limitations
- Fasting
- Inflammatory Markers
- Cholesterol Management
- Full Body MRI
- CAC Zero and the Power of Negative Result
- MESA Risk Calculator and Age Percentiles
- Agatston Score