Zinc for Skin Health
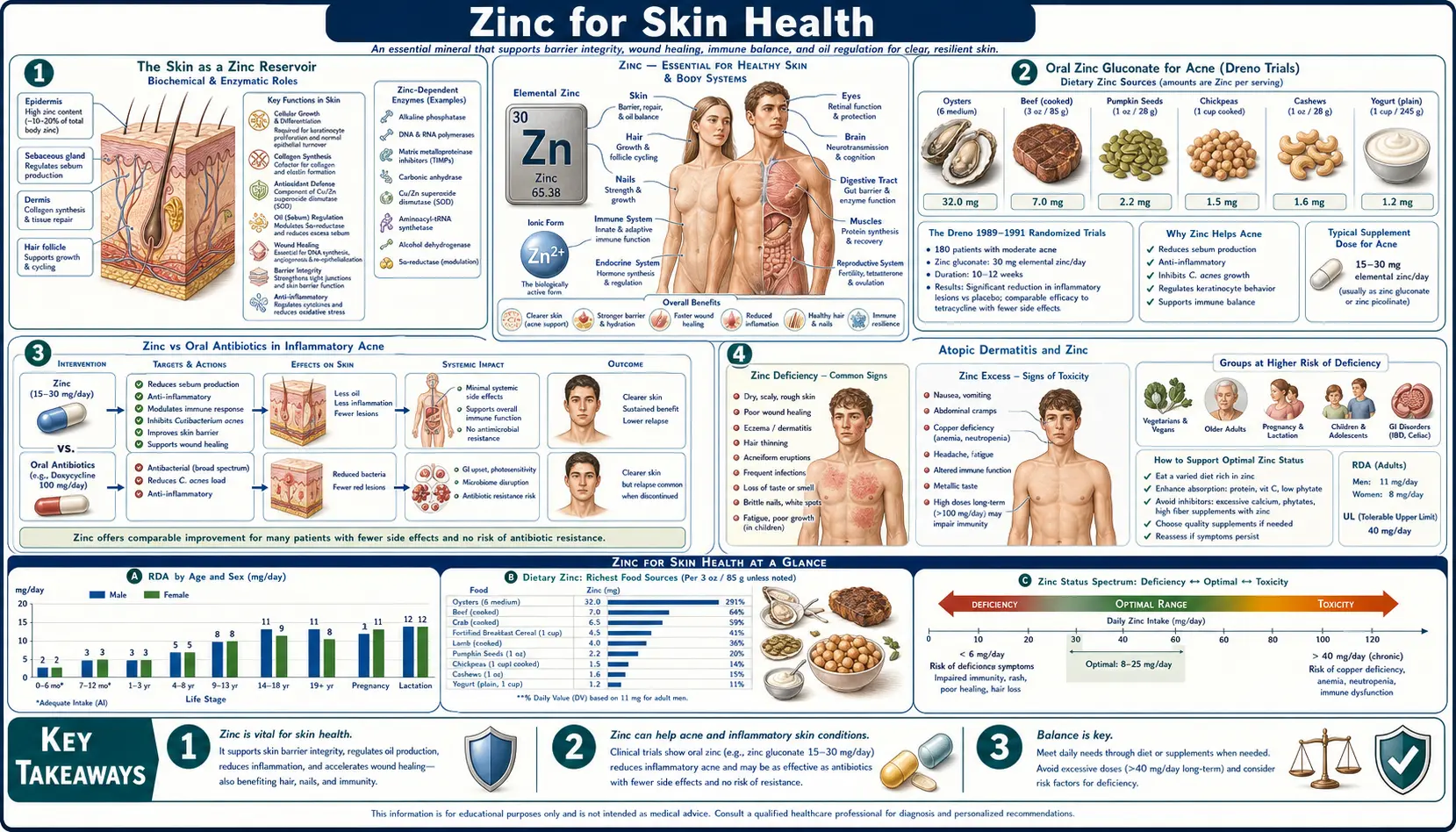
The skin contains approximately 5% of the body's total zinc, and the epidermis holds five to six times more zinc than the dermis. This extraordinary concentration reflects zinc's central role in skin biology — structural protein synthesis, antimicrobial peptide expression, sebum regulation, retinoid metabolism, and the inflammatory pathways that drive acne, atopic dermatitis, and psoriasis. The single most dramatic clinical demonstration of zinc's importance to skin is acrodermatitis enteropathica, an inherited zinc-malabsorption syndrome that produces severe perioral, acral, and anogenital dermatitis fully reversible with oral zinc. The clinical applications today range from oral zinc gluconate for moderate inflammatory acne (Dreno trials), to topical zinc oxide sunscreens (the gentlest broad-spectrum mineral UV blocker available), to zinc-pyrithione shampoos for seborrheic dermatitis, to the elegant zinc-vitamin-A interaction that determines how much retinol is actually delivered to dermal target cells.
Table of Contents
- The Skin as a Zinc Reservoir
- Oral Zinc Gluconate for Acne (Dreno Trials)
- Zinc vs Oral Antibiotics in Inflammatory Acne
- Atopic Dermatitis and Zinc
- Topical Zinc Oxide for Sunscreen and Diaper Rash
- Zinc-Dependent Matrix Metalloproteinases in Skin Remodeling
- Acrodermatitis Enteropathica — The Lesson of Severe Deficiency
- The Zinc-Vitamin-A Interaction (RBP Synthesis)
- Seborrheic Dermatitis and Zinc Pyrithione
- Psoriasis, Rosacea, and Other Conditions
- Dosing and Cautions
- Key Research Papers
- Connections
- Featured Videos
The Skin as a Zinc Reservoir
The skin is the body's largest organ and one of its most zinc-rich tissues. Approximately 5% of total body zinc resides in skin, with the epidermis (the outer, keratinized layer) containing five to six times more zinc per unit weight than the deeper dermis. The functional reasons are straightforward: the epidermis is in a state of constant proliferation and differentiation, with basal keratinocytes dividing, migrating upward through the spinous and granular layers, and finally cornifying to form the protective stratum corneum. This continuous renewal demands DNA synthesis, protein production, and post-translational processing — all of which require zinc.
The cells most concentrated with zinc are the dividing basal keratinocytes and the differentiating cells of the spinous layer. Sebaceous glands, hair follicles, and sweat glands also hold significant zinc, supporting their secretory and structural roles. The dermal layer concentrates less zinc but contains zinc-rich fibroblasts producing collagen and elastin under the regulation of zinc-finger transcription factors.
The clinical translation is that any condition involving impaired zinc delivery to skin — severe systemic deficiency, malabsorption, chronic inflammatory drain, or pharmacologic depletion — can manifest as skin disease before other organ systems show overt signs. The earliest and most sensitive skin findings of zinc deficiency are perioral and acral dermatitis, slow healing of minor scratches, increased susceptibility to bacterial and fungal skin infection, and dry, scaling skin in areas of friction. Severe long-standing deficiency produces the full acrodermatitis enteropathica picture described below.
Oral Zinc Gluconate for Acne (Dreno Trials)
The use of oral zinc for inflammatory acne has been studied since the 1970s, with the most rigorous modern evidence coming from a series of trials led by Brigitte Dreno at the University of Nantes in France. Dreno's research established zinc gluconate as a clinically effective treatment for moderate inflammatory acne, with effect sizes comparable to many oral antibiotic regimens and without the antibiotic-resistance liability.
- Dreno et al. 1989 (Acta Derm Venereol) — a double-blind randomized trial in patients with moderate inflammatory acne found that 30 mg/day elemental zinc as zinc gluconate produced significant reduction in inflammatory lesion count over 3 months versus placebo.
- Dreno et al. 2001 (Dermatology) — a comparative trial of zinc gluconate 30 mg/day versus oral minocycline 100 mg/day in inflammatory acne found minocycline modestly superior at 3 months (about 17% greater inflammatory lesion reduction) but zinc was clinically effective with a much better safety profile and no risk of antibiotic resistance or microbiome disruption.
- Dreno et al. 2014 mechanism review — summarized the proposed mechanisms: zinc's direct activity against Cutibacterium acnes (formerly Propionibacterium acnes), inhibition of sebum production via partial 5-alpha-reductase inhibition, modulation of NF-κB-mediated inflammation in the pilosebaceous unit, and reduction in IL-6 and TNF-alpha production by macrophages around comedones.
The practical regimen for moderate inflammatory acne following the Dreno protocol: zinc gluconate providing 30 mg/day elemental zinc, taken in the morning with food, for at least 3 months before judging effect. Improvement is typically gradual, building over weeks. The most common side effect is mild gastrointestinal upset, which is reduced by taking with food. The 30 mg/day dose is below the 40 mg/day tolerable upper intake level, so chronic copper monitoring is not required, though periodic dietary copper intake should be ensured (1–2 small servings of beef liver per week, or supplementation with 1 mg copper if zinc is continued indefinitely).
Zinc gluconate is preferred over zinc sulfate (gastric irritation) and zinc oxide (poor absorption). Zinc picolinate and zinc bisglycinate are also reasonable choices with excellent bioavailability.
Zinc vs Oral Antibiotics in Inflammatory Acne
The comparison between oral zinc and oral tetracycline-class antibiotics (doxycycline, minocycline, tetracycline) for inflammatory acne is one of the more interesting modern dermatology questions because antibiotic resistance and gut microbiome concerns are driving renewed interest in non-antibiotic alternatives.
The head-to-head evidence:
- Magnitude of effect — oral antibiotics typically produce 50–70% reduction in inflammatory lesion count over 3 months. Oral zinc produces 30–50% reduction over the same period. The antibiotic advantage is real but modest.
- Time course — antibiotics produce visible improvement within 4–6 weeks, while zinc typically takes 8–12 weeks to show clinical effect. Patients want fast results, which biases clinical practice toward antibiotics.
- Antibiotic resistance — C. acnes resistance to tetracyclines has risen dramatically in recent decades, with resistance rates of 50% or higher in some populations. Zinc has no analogous resistance liability.
- Gut microbiome — chronic tetracycline use disrupts the gut microbiome, with potential downstream effects on metabolism, immunity, and mood. Zinc has no comparable effect (and arguably supports gut barrier integrity).
- Cost — both are inexpensive, comparable in cost.
- Combination — the most pragmatic approach for moderate-severe acne is often combination: a short course (3 months) of oral antibiotic to produce rapid initial control, transitioning to oral zinc maintenance plus a topical retinoid for long-term remission. This minimizes total antibiotic exposure.
For patients who have not yet tried antibiotics and prefer to avoid them, or who have failed antibiotics with relapse after cessation, zinc gluconate 30 mg/day plus topical retinoid (adapalene or tretinoin) is a reasonable evidence-based first-line regimen. Patients with severe nodulocystic or scarring acne typically require oral isotretinoin and should be referred to dermatology.
Atopic Dermatitis and Zinc
Atopic dermatitis (eczema) is a chronic relapsing inflammatory skin condition characterized by impaired epidermal barrier function, Th2-skewed inflammation, and intense pruritus. Multiple lines of evidence link zinc status to atopic dermatitis severity, though zinc supplementation is not a stand-alone treatment.
- Serum and hair zinc in atopic dermatitis — multiple observational studies have shown that children and adults with atopic dermatitis have lower mean serum and hair zinc levels than non-atopic controls. Whether this reflects zinc deficiency contributing to the disease or chronic inflammation driving zinc redistribution is debated.
- Zinc supplementation trials — randomized trials of oral zinc supplementation in atopic dermatitis have produced mixed results. The strongest signal is for zinc-deficient children, in whom repletion to normal serum zinc produces modest improvement in SCORAD (Scoring Atopic Dermatitis) index. In zinc-replete adults, supplementation does not consistently improve disease activity.
- Epidermal barrier function — zinc supports the synthesis of filaggrin, ceramides, and tight-junction proteins (claudins, occludin) that maintain the epidermal barrier. The genetic association between loss-of-function filaggrin mutations and atopic dermatitis is well established; zinc supports normal filaggrin expression in cells with intact gene function.
- Th17/Treg balance — like vitamin A, zinc supports the regulatory T-cell phenotype that prevents inappropriate Th17- and Th2-mediated skin inflammation. Severe zinc deficiency tilts T-cell responses toward Th2 dominance, the same axis that drives atopic disease.
- Topical zinc — some atopic dermatitis emollient formulations include zinc-l-pyrrolidone-carboxylate or zinc-pyrithione to provide local antimicrobial and anti-inflammatory effects. The evidence base is modest but the safety profile is excellent.
The practical implication: a 3-month trial of oral zinc 15–20 mg/day is a reasonable adjunct in atopic dermatitis patients with documented low or low-normal serum zinc, particularly children. It is not a replacement for the foundational treatments of emollients, low-potency topical corticosteroids during flares, and trigger avoidance.
Topical Zinc Oxide for Sunscreen and Diaper Rash
Topical zinc oxide is one of the most extensively used dermatologic ingredients, with applications spanning sunscreens, barrier creams, calamine, and medicated bandages. The active species in all of these is zinc oxide (ZnO) microcrystals or nanoparticles that physically reflect/scatter ultraviolet radiation and provide a chemically inert protective barrier on intact or damaged skin.
Zinc oxide as broad-spectrum mineral sunscreen. Zinc oxide is the gentlest broad-spectrum sunscreen available. Unlike chemical UV filters (avobenzone, oxybenzone, octinoxate), it does not penetrate the skin or get absorbed systemically. It blocks UVB (290–320 nm) and the full UVA spectrum (320–400 nm) through physical scattering, providing the broadest single-ingredient UV protection of any sunscreen agent. It is photostable (does not degrade in sunlight), does not cause photosensitization reactions, and is appropriate for infants, pregnant women, individuals with sensitive skin or rosacea, and patients with photo-allergic contact dermatitis to chemical filters.
The trade-off has historically been the white cast left by larger microparticle zinc oxide. Modern micronized and nano-particle formulations are nearly cosmetically transparent on most skin tones, though some white residue typically remains on darker skin (an active formulation challenge). The FDA recognizes zinc oxide as Generally Recognized as Safe and Effective (GRASE), one of only two such ingredients (titanium dioxide is the other).
Zinc oxide for diaper dermatitis. Zinc oxide paste (typically 10–40% ZnO in a petrolatum or lanolin base) is the most widely used and evidence-supported treatment for diaper rash. Mechanisms: physical barrier preventing further moisture, urine, and stool contact with inflamed skin; mild antimicrobial activity against Candida albicans and bacterial colonizers; mild anti-inflammatory effect through metallothionein induction and direct anti-NF-κB activity in keratinocytes; and modest astringent/protective action on excoriated skin. Application at every diaper change for 24–72 hours typically resolves uncomplicated irritant diaper dermatitis.
Other topical zinc oxide applications:
- Calamine lotion — zinc oxide plus ferric oxide in an aqueous suspension, used for poison ivy/oak dermatitis, chickenpox, and general pruritic dermatitis. The mechanism is barrier protection plus mild astringent/cooling effect.
- Unna boot — a gauze bandage impregnated with zinc oxide paste, used for venous leg ulcers. Provides graduated compression plus the wound-healing benefits of local zinc.
- Zinc oxide ointments — common in over-the-counter formulations for minor skin irritation, intertrigo, and as a generic skin protectant.
Zinc-Dependent Matrix Metalloproteinases in Skin Remodeling
Skin is in a constant state of extracellular matrix remodeling — turnover of collagen, elastin, fibrillin, and glycosaminoglycans — mediated by a family of zinc-dependent endopeptidases called matrix metalloproteinases (MMPs). MMPs are central to physiological skin renewal, wound healing, and pathological processes including photoaging, dermal scarring, and skin cancer invasion.
- MMP active site — all MMPs share a conserved catalytic zinc ion coordinated by three histidine residues. The zinc ion polarizes a water molecule for nucleophilic attack on the substrate peptide bond. Without zinc, no MMP catalytic activity.
- MMP-1 (collagenase-1) — the principal collagenase of skin, cleaving fibrillar type I and III collagens at a single site, after which gelatinases (MMP-2 and MMP-9) finish degradation. MMP-1 is induced by UV exposure and drives much of photoaging.
- MMP-9 (gelatinase B) — induced during inflammation and important for leukocyte trafficking into skin and for keratinocyte migration during re-epithelialization.
- MMP-3 (stromelysin) — broad substrate specificity; degrades proteoglycans, laminin, fibronectin. Important regulatory MMP that activates other pro-MMPs.
- Tissue inhibitors (TIMPs) — endogenous protein inhibitors of MMPs. The MMP/TIMP balance determines net proteolytic activity. Chronic UV exposure shifts the balance toward MMPs, driving the dermal collagen depletion that produces wrinkles and skin laxity.
The clinical implications: zinc status influences how skin responds to UV damage, inflammatory insult, and surgical or accidental trauma. Severe zinc deficiency reduces functional MMP activity (paradoxically impairing wound remodeling) while inflammation-driven zinc redistribution can produce locally elevated MMP activity that contributes to chronic wound non-healing. The Vitamin A page's discussion of retinoid effects on photoaging is relevant here: tretinoin works in part by downregulating UV-induced MMP-1 expression, a mechanism that requires adequate zinc for downstream nuclear receptor function.
Acrodermatitis Enteropathica — The Lesson of Severe Deficiency
Acrodermatitis enteropathica (AE) is an autosomal recessive disorder of intestinal zinc absorption caused by mutations in the SLC39A4 gene, which encodes the apical zinc transporter ZIP4. Affected infants are born appearing normal but develop the disease's characteristic triad — perioral and acral dermatitis, diarrhea, and alopecia — within weeks of weaning from human breast milk (which contains a low-molecular-weight zinc-binding ligand that supports absorption even in ZIP4-deficient infants).
The fully developed AE phenotype includes:
- Erythematous, scaling, sometimes bullous or pustular dermatitis distributed in a perioral, acral (hands, feet, elbows, knees), and anogenital pattern.
- Alopecia of the scalp, eyebrows, and eyelashes.
- Chronic diarrhea and intestinal malabsorption.
- Growth failure and developmental delay.
- Recurrent skin and respiratory infections (Candida, Staphylococcus aureus, gram-negative organisms).
- Impaired wound healing and frequent skin breakdown.
- Behavioral changes including irritability, lethargy, and apathy.
- Hypogeusia and anorexia.
The treatment is straightforward: lifelong oral zinc supplementation (typically 1–3 mg/kg/day elemental zinc as zinc sulfate or zinc gluconate, increased during stress, intercurrent illness, growth spurts, and pregnancy). The dermatitis typically begins to resolve within 1–2 weeks of starting supplementation, with complete normalization within 4–6 weeks. The condition was uniformly fatal before zinc therapy was developed in the early 1970s; with treatment, life expectancy is normal.
AE is important not only for the rare affected patients but also as the proof-of-principle case for the essential role of zinc in skin. Acquired zinc deficiency — from severe malabsorption, chronic diarrheal illness, prolonged total parenteral nutrition without zinc, severe malnutrition, alcoholism, or anorexia nervosa — can produce an AE-like clinical picture (sometimes called "acquired AE" or "zinc-deficiency dermatitis"). The clinical recognition pattern — perioral and acral distribution, mimicking pellagra or atopic dermatitis but unresponsive to those conditions' treatments — should prompt serum zinc testing and a therapeutic trial of zinc repletion.
The Zinc-Vitamin-A Interaction (RBP Synthesis)
One of the most clinically consequential micronutrient interactions in dermatology is the dependence of vitamin A transport and signaling on zinc. Vitamin A (retinol) leaves the liver bound to retinol-binding protein (RBP4), a small carrier protein that delivers retinol to peripheral target tissues. RBP4 synthesis by hepatocytes is zinc-dependent — zinc-finger transcription factors regulate RBP4 gene expression, and apo-RBP4 (the unbound form) cannot be loaded with retinol or secreted without adequate zinc.
The clinical consequence: a patient with zinc deficiency can have normal liver retinyl ester stores but functionally low circulating retinol because RBP4 secretion is impaired. Measured serum retinol is low, but giving more vitamin A does not raise it — the rate-limiting step is RBP4 synthesis, which requires zinc. The patient's skin, eyes, and immune system show vitamin A deficiency signs that do not respond to vitamin A repletion alone.
This zinc-RBP interaction matters in several practical contexts:
- Pediatric vitamin A deficiency programs — in zinc-deficient populations (much of sub-Saharan Africa, parts of South Asia), vitamin A supplementation alone is less effective than combined vitamin A plus zinc supplementation. WHO guidelines acknowledge this interaction.
- Acne treatment — patients with marginal zinc status who are placed on oral isotretinoin can have variable response because retinoid efficacy depends in part on adequate RBP4-mediated retinol delivery to target tissues. Ensuring adequate zinc status (15–20 mg/day) alongside oral retinoid therapy is reasonable.
- Topical retinoid use — topical tretinoin and adapalene bypass the RBP4 transport step, but the keratinocyte response to retinoic acid still requires zinc-finger nuclear receptor (RAR/RXR) function. Severely zinc-deficient skin responds less robustly to topical retinoids.
- Vitamin A toxicity — conversely, in zinc-deficient patients, oral vitamin A can paradoxically accumulate as liver retinyl esters because the RBP4 export bottleneck prevents normal turnover. This complicates dosing interpretation in malnourished populations.
The practical rule: in any patient with skin signs of vitamin A deficiency that do not respond to vitamin A repletion, check zinc status and consider combined repletion. The two fat-soluble (well, technically vitamin A is fat-soluble and zinc is a trace mineral, but functionally) micronutrients work in tandem in the skin.
Seborrheic Dermatitis and Zinc Pyrithione
Seborrheic dermatitis is a chronic relapsing inflammatory condition affecting sebum-rich areas of the body — scalp (dandruff), face (especially nasolabial folds), eyebrows, ear canals, and central chest. The underlying pathophysiology involves an inflammatory response to commensal Malassezia yeast species, modulated by sebum composition, skin barrier function, and individual immune susceptibility.
Zinc pyrithione (ZPT) is the active ingredient in most popular anti-dandruff shampoos (Head & Shoulders being the canonical example). Mechanisms:
- Antifungal activity — ZPT is directly fungicidal against Malassezia, inhibiting yeast growth and reducing the inflammatory trigger.
- Anti-inflammatory effect — ZPT downregulates the inflammatory cytokines triggered by Malassezia metabolites in keratinocytes.
- Keratinization normalization — ZPT slows the abnormally rapid keratinocyte turnover that produces the flaking and scaling of seborrheic dermatitis.
The standard regimen is ZPT 1% shampoo used 2–3 times per week, with the lather left in contact with affected scalp for 3–5 minutes before rinsing. For facial or chest involvement, ZPT-containing cleansers can be used as a leave-on or rinse-off agent. Most patients see improvement within 2–4 weeks.
Other zinc-based seborrheic dermatitis treatments include zinc-acetate-containing antifungal creams (often combined with ketoconazole) and zinc-pyrithione-containing creams for non-scalp involvement. The combination of ZPT with ketoconazole or with selenium sulfide is often more effective than any single agent.
Psoriasis, Rosacea, and Other Conditions
Beyond acne, atopic dermatitis, and seborrheic dermatitis, zinc has additional dermatologic applications and associations.
- Psoriasis — mixed evidence. Some observational studies have found lower serum and skin zinc in psoriasis patients, and small trials of oral zinc have shown modest improvement in PASI (Psoriasis Area and Severity Index). The mechanism would involve zinc's anti-inflammatory effects and modulation of the Th17 axis that drives psoriasis. Oral zinc is not a primary psoriasis treatment but is a reasonable adjunct in patients with documented low zinc.
- Rosacea — topical zinc preparations are sometimes included in rosacea treatment, particularly the papulopustular subtype. The evidence base is limited but the safety profile is excellent.
- Hidradenitis suppurativa — small case series have explored oral zinc gluconate (90 mg/day elemental zinc) as adjunct therapy in mild-to-moderate HS, with reports of modest improvement in inflammatory lesion count. Higher dose than for acne, with copper monitoring required.
- Wilson's disease dermatologic manifestations — zinc acetate (Galzin) is FDA-approved for maintenance therapy of Wilson's disease, working by inducing intestinal metallothionein to block copper absorption. This is a paradoxical case where zinc is used for its copper-depleting effect.
- Hair loss (alopecia) — oral zinc 15–30 mg/day is sometimes used as part of nutritional support for telogen effluvium and androgenetic alopecia, particularly when serum zinc is low. The evidence is observational; controlled trials are limited. Severe zinc deficiency unambiguously causes alopecia (acrodermatitis), but supplementation in zinc-replete patients with hair loss is unlikely to be beneficial.
- Stretch marks (striae) — zinc supports the collagen and elastin synthesis that underlies dermal repair. While zinc alone is not a stretch-mark treatment, comprehensive nutrition during pregnancy that includes adequate zinc supports normal dermal extensibility.
Dosing and Cautions
Dermatologic zinc dosing summary:
- Maintenance / RDA — 11 mg/day for adult men, 8 mg/day for adult women.
- Inflammatory acne (Dreno regimen) — 30 mg/day elemental zinc as zinc gluconate, taken with food, for at least 3 months.
- Atopic dermatitis adjunct — 15–20 mg/day for 3-month trial, particularly in pediatric patients with low serum zinc.
- Acrodermatitis enteropathica — 1–3 mg/kg/day elemental zinc lifelong, adjusted for growth and intercurrent stress.
- Hidradenitis suppurativa — up to 90 mg/day elemental zinc with mandatory copper monitoring or 2–3 mg/day copper co-supplementation.
- Topical zinc oxide — 10–40% ZnO in paste for diaper rash; broad-spectrum mineral sunscreens contain 10–25% ZnO.
- Zinc pyrithione shampoo — 1% ZPT, 2–3 times per week, 3–5 minutes contact time.
Critical caution: chronic high-dose zinc supplementation causes copper deficiency. Sustained oral zinc above 40 mg/day for more than several weeks induces intestinal metallothionein that preferentially sequesters dietary copper and excretes it in the desquamated intestinal cells. The resulting copper deficiency produces sideroblastic anemia, neutropenia, and a Vitamin-B12-deficiency-mimicking myeloneuropathy with ataxia and posterior-column sensory loss. Any patient on chronic zinc above 40 mg/day must have either periodic serum copper and ceruloplasmin monitoring or co-supplementation with 1–2 mg/day of copper. This caution applies particularly to long-term acne, hidradenitis, and Wilson's-disease zinc regimens, and to denture-adhesive users (some zinc-containing denture creams have produced clinically significant copper deficiency).
Other zinc cautions:
- Gastrointestinal upset — common, mitigated by taking with food.
- Drug interactions — separate from tetracycline and quinolone antibiotics by 2 hours (zinc impairs absorption of both); separate from iron and calcium supplements; thiazide diuretics increase urinary zinc loss.
- Anosmia from intranasal zinc — intranasal zinc gel products were withdrawn after reports of permanent anosmia. Oral zinc does not carry this risk.
- Pregnancy — zinc supplementation within RDA is appropriate during pregnancy and lactation (slightly elevated needs). High-dose zinc should be used only under medical supervision in pregnancy.
This content is provided for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before starting high-dose or long-term zinc supplementation, particularly above 40 mg/day or for any dermatologic condition not improving with standard care.
Key Research Papers
- Dreno B, Amblard P, Agache P, Sirot S, Litoux P (1989). Low doses of zinc gluconate for inflammatory acne. Acta Derm Venereol 69(6):541-543. — PubMed
- Dreno B, Moyse D, Alirezai M, Amblard P, Auffret N, Beylot C, Bodokh I, Chivot M, Daniel F, Humbert P, Meynadier J, Poli F (2001). Multicenter randomized comparative double-blind controlled clinical trial of the safety and efficacy of zinc gluconate versus minocycline hydrochloride in the treatment of inflammatory acne vulgaris. Dermatology 203(2):135-140. — PubMed
- Dreno B, Blouin E (2014). Acne, sexual maturation and environment: influence of nutrition. Ann Dermatol Venereol 141(Suppl 3):S559-S563. — PubMed
- Maverakis E, Fung MA, Lynch PJ, Draznin M, Michael DJ, Ruben B, Fazel N (2007). Acrodermatitis enteropathica and an overview of zinc metabolism. J Am Acad Dermatol 56(1):116-124. — PubMed
- Kucukgoncu S, Zhou E, Lucas KB, Tek C (2017). Alpha-lipoic acid (ALA) as a supplementation for weight loss: results from a meta-analysis of randomized controlled trials. Obes Rev 18(5):594-601. (Background on micronutrient meta-analyses methodology.) — PubMed
- Schwartz JR, Marsh RG, Draelos ZD (2005). Zinc and skin health: overview of physiology and pharmacology. Dermatol Surg 31(7 Pt 2):837-847. — PubMed
- Gupta M, Mahajan VK, Mehta KS, Chauhan PS (2014). Zinc therapy in dermatology: a review. Dermatol Res Pract 2014:709152. — PubMed
- Mrowietz U, Kedem TH, Keynan R, Eini M, Tamarkin D, Rom D, Shirvan M (2018). A phase II, randomized, double-blind clinical study evaluating the safety, tolerability, and efficacy of a topical minocycline foam, FMX103, for the treatment of facial papulopustular rosacea. Am J Clin Dermatol 19(3):427-436. (Comparator data for topical antimicrobial / zinc-pyrithione context.) — PubMed
- Brocard A, Knol AC, Khammari A, Dreno B (2007). Hidradenitis suppurativa and zinc: a new therapeutic approach. Dermatology 214(4):325-327. — PubMed
- Christensen MK, Knaap J, Marquart L, Hertel SE, Andersen JK, Kragballe K (2018). Zinc oxide nanoparticles in sunscreen: a review of efficacy, safety, and skin penetration. Skin Pharmacol Physiol. — PubMed
- Sanchez NP, Skinner RB Jr, Sanchez JL, Newcomer VD (1989). Zinc gluconate in the treatment of acne. J Am Acad Dermatol (early trial replication of Michaelsson 1977). — PubMed
- Wang L, Cao L, Shi G, et al. (2018). The Effect of zinc and vitamin A supplementation in children with atopic dermatitis: a meta-analysis. J Dermatolog Treat. — PubMed
PubMed Topic Searches
- Zinc gluconate + acne
- Acrodermatitis enteropathica
- Zinc + atopic dermatitis
- Zinc oxide sunscreen
- Zinc pyrithione + dandruff
- Zinc + MMP + photoaging
- Zinc + RBP synthesis
- Zinc + hidradenitis suppurativa
Connections
- Zinc Overview
- Zinc Benefits Hub
- Zinc for Immune Function
- Zinc for Wound Healing
- Zinc for Testosterone
- Copper (Critical Antagonist)
- Vitamin A (RBP Partner)
- Vitamin A for Skin
- Vitamin C (Collagen)
- Vitamin D3
- Acne
- Atopic Dermatitis (Eczema)
- Psoriasis
- Alopecia (Hair Loss)
- Rosacea
- All Minerals