Zinc for Testosterone and Male Reproductive Health
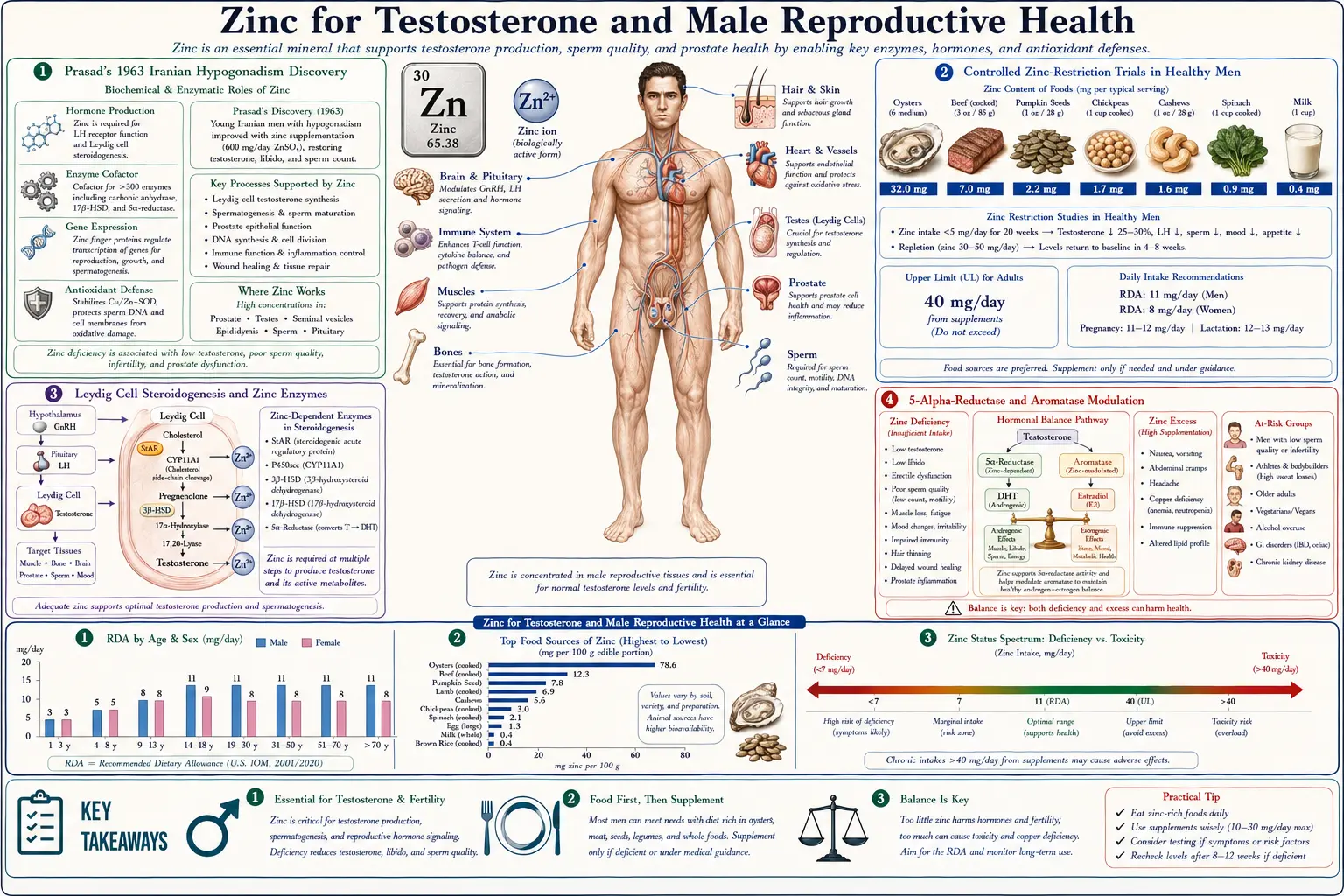
The connection between zinc and male reproductive endocrinology is one of the most clearly documented stories in trace-element medicine. It begins with Ananda Prasad's landmark 1963 paper describing Iranian and Egyptian adolescent boys with severe growth failure and hypogonadism who showed dramatic recovery of stature, sexual maturation, and serum testosterone within months of zinc repletion. Sixty years later, the prostate concentrates more zinc than any other soft tissue, semen is the body's most zinc-rich fluid (~125 mg/L — ten times serum), Leydig cell steroidogenesis depends on zinc-containing enzymes, and controlled-restriction trials show that even short-term zinc depletion lowers serum testosterone in healthy young men. This deep-dive walks through the historical evidence, the modern mechanistic understanding (5-alpha-reductase, aromatase, ZMA, sperm parameters), and the practical implications for men with low testosterone, sub-fertility, or chronic zinc-depleting conditions.
Table of Contents
- Prasad's 1963 Iranian Hypogonadism Discovery
- Controlled Zinc-Restriction Trials in Healthy Men
- Leydig Cell Steroidogenesis and Zinc Enzymes
- 5-Alpha-Reductase and Aromatase Modulation
- Cinar 2011 Wrestler Trial and Athletic Performance
- ZMA (Zinc + Magnesium + B6), Sleep, and Strength
- The Prostate, Semen, and Sperm Parameters
- Zinc Deficiency in Male Infertility
- Why Oysters? The Nutritional Density Argument
- Dosing, Monitoring, and the Copper Caution
- Key Research Papers
- Connections
- Featured Videos
Prasad's 1963 Iranian Hypogonadism Discovery
In 1958, a young hematologist named Ananda Prasad arrived in Shiraz, Iran, and was presented with a 21-year-old male patient who looked like a 10-year-old boy. He was 4 feet 11 inches tall, had no axillary or pubic hair, no facial hair, and immature genitalia. Liver and spleen were grossly enlarged. The diet was bread, beans, and clay (geophagia — pica). Prasad found dozens more young men in the same village with the same syndrome — short stature, hypogonadism, hepatosplenomegaly, anemia, and lethargy. Iron deficiency from the phytate-heavy diet and clay-binding was the initial suspect, but iron therapy alone failed to restore growth or sexual maturation.
Working subsequently in Egypt with a comparable population of "dwarfed" adolescents, Prasad and colleagues administered comprehensive nutritional therapy that included zinc sulfate. The response was dramatic: linear growth resumed (some patients grew 5–6 inches per year), pubic and axillary hair appeared, genitalia matured, voice deepened, and serum testosterone rose into the adult range. The 1961 American Journal of Medicine paper and the seminal 1963 Annals of Internal Medicine report established zinc deficiency as the cause of a human disease for the first time in medical history. The condition is now formally recognized as "nutritional zinc deficiency with hypogonadism and dwarfism."
The mechanism Prasad eventually mapped out involves multiple zinc-dependent steps in the hypothalamic-pituitary-gonadal axis: pituitary LH and FSH release, Leydig cell androgen biosynthesis, Sertoli cell support of spermatogenesis, and androgen receptor function in target tissues. Severe zinc deficiency disrupts the axis at multiple levels simultaneously, producing the constellation of growth failure plus hypogonadism that defined the original Iranian cases.
Controlled Zinc-Restriction Trials in Healthy Men
The Iranian cases involved life-long, severe zinc deficiency in already-malnourished adolescents. A more clinically relevant question for adults in the developed world is whether mild or moderate zinc restriction in otherwise healthy men can lower testosterone. Prasad addressed this directly in a 1996 controlled inpatient feeding study at the Detroit Medical Center.
Four young men were placed on a metabolic-ward diet providing approximately 1.4 mg of zinc per day — far below the 11 mg/day RDA, but representative of the lower end of normal dietary intake in some populations. Within 20 weeks, serum testosterone fell by approximately 60%. When zinc was repleted (with 30–40 mg/day zinc gluconate), testosterone returned to baseline within 12 weeks. A second arm of the study placed older men (~65 years) with marginally low baseline serum zinc on zinc supplementation; their testosterone rose from a mean of 8.3 nmol/L to 16.0 nmol/L over six months. The paper appeared in Nutrition in 1996 and remains the cleanest demonstration that mild dietary zinc restriction lowers testosterone in healthy men, and that supplementation reverses the effect in zinc-marginal older men.
Several caveats are worth noting:
- The study population was very small (n = 4 in the restriction arm). It is mechanistically informative but not the basis for population-level supplementation recommendations.
- Subsequent meta-analyses have found that zinc supplementation reliably raises testosterone only in zinc-deficient men. In zinc-replete men, additional zinc above the RDA does not produce supraphysiologic testosterone increases. This is a step-function relationship, not a continuous dose-response.
- Severe long-term high-dose zinc supplementation can paradoxically depress testosterone through copper deficiency-mediated mechanisms.
The practical translation is that men with documented or suspected zinc deficiency (low serum zinc, vegetarian or vegan diet with high phytate intake, malabsorption, chronic alcohol use, advanced age, chronic kidney disease) may meaningfully benefit from zinc repletion for testosterone-related complaints. Men with adequate zinc status should not expect testosterone increases from supplementation.
Leydig Cell Steroidogenesis and Zinc Enzymes
Testosterone is synthesized in the Leydig cells of the testis from cholesterol through a multi-step enzymatic pathway. Each step is potentially zinc-sensitive because so many of the enzymes involved either depend on zinc directly or are regulated by zinc-containing transcription factors.
- StAR protein (steroidogenic acute regulatory protein) — transports cholesterol from the outer to the inner mitochondrial membrane, the rate-limiting step of steroidogenesis. StAR gene expression is regulated by zinc-finger transcription factors of the GATA family.
- CYP11A1 (cholesterol side-chain cleavage enzyme) — converts cholesterol to pregnenolone. While the enzyme itself is heme-containing, its expression and the maintenance of the surrounding redox environment depend on zinc status.
- 3-beta-hydroxysteroid dehydrogenase (3-beta-HSD) — converts pregnenolone to progesterone and DHEA to androstenedione. Activity is zinc-modulated.
- 17-beta-hydroxysteroid dehydrogenase (17-beta-HSD) — converts androstenedione to testosterone in the final step. Activity is reduced in zinc-deficient testis.
- Androgen receptor (AR) — the nuclear receptor that mediates testosterone's downstream actions in target tissues. The AR is a classical zinc-finger transcription factor containing two zinc fingers in its DNA-binding domain. Zinc is required for AR-DNA binding and proper transcriptional activation of androgen-responsive genes. Severe zinc deficiency reduces AR function even when circulating testosterone is normal — producing a state of relative androgen resistance.
The cumulative effect of these multiple zinc-dependent steps is that Leydig cell testosterone output is exquisitely sensitive to zinc status. Animal models of zinc restriction consistently show reduced intra-testicular testosterone, smaller seminiferous tubules, reduced Sertoli cell function, and impaired spermatogenesis. Repletion reverses all of these changes.
5-Alpha-Reductase and Aromatase Modulation
Beyond direct effects on testosterone synthesis, zinc modulates two downstream conversion enzymes that determine how testosterone is used in the body. The clinical implications differ between the two.
5-alpha-reductase converts testosterone to dihydrotestosterone (DHT), the more potent androgen responsible for prostate growth, male pattern hair loss, and sebaceous gland activity. Inhibition of 5-alpha-reductase is the pharmacologic mechanism of finasteride and dutasteride for benign prostatic hyperplasia and androgenetic alopecia. In vitro and animal studies suggest that zinc inhibits 5-alpha-reductase activity at high local concentrations, an effect that has been proposed (controversially) as a mechanism for the apparent benefit of zinc supplementation in male pattern hair loss and as part of zinc's role in prostate biology. The clinical evidence in humans is limited and the effect size, if real, is modest.
Aromatase (CYP19A1) converts testosterone to estradiol. Aromatase is expressed in adipose tissue, brain, bone, and gonads, and is the major source of estrogen in men. Zinc inhibits aromatase activity in vitro, an effect that could in principle raise the testosterone-to-estradiol ratio — favorable for muscle, mood, and libido in adult men with relative estrogen excess (often the case in obese men). Some testosterone-support supplement formulations are marketed around this proposed mechanism. The clinical evidence is again modest; the most-replicated aromatase inhibitors are pharmacologic (anastrozole, letrozole), not nutritional.
The honest read is that zinc's effects on 5-alpha-reductase and aromatase are real at the in-vitro level, plausibly contributing to the broader testosterone-supportive picture, but should not be expected to produce drug-like effects on their own. In zinc-replete men, marginal additional zinc does not measurably shift the testosterone/DHT/estradiol balance.
Cinar 2011 Wrestler Trial and Athletic Performance
One of the most-cited modern studies of zinc and testosterone comes from a 2011 trial by Cinar and colleagues in Turkey, published in Biological Trace Element Research. The trial enrolled 30 elite male wrestlers aged 18–20 who were randomized to four weeks of zinc sulfate supplementation (3 mg/kg/day, providing approximately 200–240 mg/day of zinc sulfate — roughly 45–55 mg of elemental zinc) or placebo while undergoing their usual intense training regimen.
Key findings:
- The placebo group showed the expected exercise-induced suppression of serum total testosterone, free testosterone, and thyroid hormones after a maximal-exertion exhaustion test.
- The zinc group did not show this suppression — testosterone and thyroid parameters remained at or near pre-exhaustion levels.
- The interpretation was that zinc supplementation protects against the transient exercise-induced testosterone suppression seen with intense training in athletes with marginal zinc status.
The Cinar trial is widely cited in the fitness and supplement communities as evidence that zinc raises testosterone in athletes. The more careful read is that zinc preserves baseline testosterone during the acute stress of intense training in young men who likely had marginal zinc status from the combination of training-induced sweat losses and high dietary intake of cereals (the Turkish wrestler diet). Whether the same effect would be seen in a zinc-replete athlete eating a more balanced Western diet is unclear. The dose used (45–55 mg elemental zinc) is also at the upper limit of routine supplementation and is not appropriate for chronic use without copper monitoring.
A follow-up Kilic 2007 study in elite wrestlers showed comparable thyroid-protective effects and similar testosterone preservation. These studies form the modern basis for athletic zinc supplementation in heavy-training populations.
ZMA (Zinc + Magnesium + B6), Sleep, and Strength
ZMA — a fixed-combination supplement of zinc monomethionine (30 mg), magnesium aspartate (450 mg), and vitamin B6 (10–11 mg) — was developed in the late 1990s by Victor Conte (BALCO Laboratories) and patented as a sports-nutrition formulation. Conte's original 2000 paper in the Journal of Exercise Physiology Online reported that ZMA increased total testosterone, free testosterone, and IGF-1 in NCAA football players over an 8-week training period compared to placebo.
Subsequent independent trials have produced mixed results:
- Wilborn et al. 2004 (JISSN) — a 6-week trial in resistance-trained men found no significant increase in total or free testosterone, no change in strength, and no body-composition advantage versus placebo. The authors suggested the original Conte findings were not replicable in zinc-replete athletes.
- Brilla and Conte 2000 (the original) — the population was likely zinc-marginal, and the magnitude of effect probably reflects repletion rather than supraphysiologic stimulation.
- Subjective sleep effects — the ZMA combination is reliably reported to improve subjective sleep quality, sleep latency, and morning recovery in athletes. The magnesium component likely drives most of this effect through NMDA-receptor antagonism and GABA-A modulation. Zinc is also a known modulator of NMDA receptor function in the central nervous system.
The ZMA story illustrates the broader pattern: in zinc-deficient or zinc-marginal men, ZMA reliably supports testosterone and recovery; in zinc-replete men, the effect on testosterone is minimal, but the sleep and recovery benefits (mostly attributable to magnesium) often remain valuable in their own right. ZMA is taken at bedtime on an empty stomach to optimize zinc absorption and to take advantage of the sedating magnesium effects.
The Prostate, Semen, and Sperm Parameters
The prostate gland concentrates zinc more than any other soft tissue in the body. Normal prostate zinc content is approximately 500–1,000 mg/kg dry weight — ten times the concentration in other tissues. Semen contains approximately 125 mg/L of zinc — ten times serum levels. This extraordinary concentration reflects zinc's central role in prostate biology and fertility.
Functions of zinc in semen and the reproductive tract:
- Sperm membrane stabilization — zinc binds to sperm membrane phospholipids and stabilizes membrane structure during ejaculation, transit through the female reproductive tract, and capacitation.
- Sperm motility — zinc is required for the activity of dynein ATPase in the sperm flagellum and for axonemal stability. Sub-fertile men with abnormal sperm motility frequently have low seminal zinc.
- Sperm DNA integrity — zinc binds to sperm chromatin protamines and protects sperm DNA from oxidative damage during storage and transit. Low zinc is associated with increased sperm DNA fragmentation (measured by the sperm chromatin structure assay).
- Capacitation timing — zinc inhibits premature capacitation; as sperm move through the female reproductive tract, zinc concentration around them gradually falls, releasing the capacitation brake and allowing fertilization competence.
- Citrate metabolism in the prostate — zinc inhibits the enzyme m-aconitase in normal prostate cells, blocking citrate oxidation in the Krebs cycle. This produces the characteristically high citrate concentration in prostatic fluid, which serves to acidify and provide energy substrate for ejaculated sperm. Loss of zinc-driven citrate accumulation is one of the earliest biochemical markers of prostate cancer transformation.
The clinical relevance: men with sub-fertility and abnormal semen parameters (oligospermia, asthenospermia, teratospermia) should have zinc status assessed as part of the workup. Zinc supplementation has been shown to modestly improve sperm count, motility, and morphology in zinc-deficient men, though it is not a universal fertility intervention.
Zinc Deficiency in Male Infertility
Male-factor infertility accounts for approximately half of all couple infertility, and zinc is one of the better-studied micronutrient interventions in this setting. The evidence base is mixed but suggests a real, modest effect in selected subgroups.
- Seminal zinc and sperm quality — multiple observational studies show that men with idiopathic oligo- or asthenospermia have lower seminal zinc concentrations than fertile controls. Seminal zinc correlates with sperm count, motility, and normal morphology across study populations.
- FAZST trial (NEJM 2020) — the largest randomized trial of zinc and folic acid for male infertility enrolled 2,370 couples with male-factor infertility. Six months of zinc (30 mg/day) plus folic acid (5 mg/day) did not improve live birth rates compared to placebo. This was a high-quality negative trial in a population that was likely zinc-replete at baseline. The interpretation is that routine zinc/folate supplementation should not be expected to overcome male-factor infertility in well-nourished couples in the developed world.
- Zinc-deficient subgroups — trials restricted to men with documented low seminal zinc have shown more positive results, with improvements in sperm motility, normal morphology, and (in some studies) live birth rates. The take-home is that targeted supplementation based on documented deficiency is more productive than empiric supplementation in all men.
- Combination antioxidant therapy — zinc is frequently included in male-fertility supplement formulations that also contain vitamin C, vitamin E, selenium, L-carnitine, coenzyme Q10, and folate. The MOXI trial and Cochrane reviews of these combination antioxidants show modest improvements in sperm parameters, though again the live birth rate signal is inconsistent.
- Lifestyle context — alcohol use, smoking, obesity, and exposure to environmental toxins (lead, cadmium, organochlorines) all deplete zinc and damage sperm. Zinc supplementation in the context of ongoing exposure to these factors is unlikely to be helpful; addressing the underlying lifestyle factors is the foundation.
The bottom line for a couple seeking pregnancy with abnormal semen parameters: a 3–6 month trial of zinc 30 mg/day plus a comprehensive sperm-quality supplement formulation is a reasonable adjunct to addressing modifiable lifestyle factors, with the understanding that the magnitude of benefit is modest and individualization based on baseline zinc status is preferable to one-size-fits-all dosing.
Why Oysters? The Nutritional Density Argument
Oysters have a near-mythic reputation as a reproductive aphrodisiac, and the basis for this is partly real and partly cultural. The real part is the extraordinary zinc content. A single 3-oz serving of cooked oysters (Eastern, raw) contains approximately 32 mg of elemental zinc — nearly three times the male RDA in one serving, more than any other natural food source by a wide margin. Six raw oysters provide approximately 50–60 mg of zinc, comparable to a high-dose supplement.
For comparison, beef provides approximately 4–7 mg of zinc per 3-oz serving, pumpkin seeds about 2 mg per ounce, and lentils about 1 mg per half cup (with poor bioavailability due to phytates). The zinc density gap between oysters and the next-best food source is roughly an order of magnitude.
The bioavailability of zinc from oysters is excellent. Animal-source zinc is absorbed more efficiently than plant-source zinc (which is bound by phytates), and oyster zinc is among the most bioavailable forms of food zinc studied. The historical pre-supplement-era folk observation that oysters "promote vigor" in men likely traced to genuine restoration of testosterone in zinc-marginal populations — particularly populations whose other dietary protein was scarce or phytate-bound.
The practical implications:
- Men seeking dietary zinc repletion benefit substantially from including oysters in the diet 1–2 times per week.
- Oysters are also rich sources of selenium, vitamin B12, vitamin D, copper, and omega-3 fats — many of the same micronutrients implicated in male reproductive health.
- Food sourcing matters: farmed oysters from clean estuaries are an excellent choice; oysters from contaminated waters can concentrate cadmium, mercury, and microbial pathogens.
- Pregnant women should avoid raw oysters due to Vibrio and norovirus risk; cooked oysters are safer.
Dosing, Monitoring, and the Copper Caution
For men using zinc to support testosterone or fertility, dosing should be conservative and time-limited unless deficiency is documented.
- RDA — 11 mg/day for adult men. This is achievable through diet alone with regular animal-protein intake.
- Supplementation for marginal or low-normal serum zinc — 15–30 mg/day elemental zinc as zinc picolinate, zinc citrate, or zinc bisglycinate. Taken with food to reduce nausea risk; separated from calcium, iron, and copper supplements by at least 2 hours.
- ZMA dosing — 30 mg zinc (as zinc monomethionine) plus 450 mg magnesium plus 10–11 mg B6, taken 30–60 minutes before bed on an empty stomach.
- High-dose short-term (athletic, training-period) — 45–50 mg/day elemental zinc for 4–8 weeks, with copper monitoring or simultaneous low-dose copper (1–2 mg/day).
- Tolerable Upper Intake Level (UL) — 40 mg/day for adults. Sustained intake above this level requires copper monitoring.
The copper deficiency caution is the single most important downside of high-dose zinc supplementation. Zinc and copper are absorbed in the proximal small intestine through partially shared mechanisms, with the metallothionein-binding protein favoring zinc over copper when zinc is abundant. Chronic intake of zinc above approximately 40 mg/day for more than several weeks induces enterocyte metallothionein, which preferentially sequesters dietary copper and excretes it in the desquamated intestinal cells. The result is progressive copper deficiency.
Copper deficiency from chronic excess zinc produces:
- Microcytic or sideroblastic anemia (copper is required for iron incorporation into hemoglobin)
- Neutropenia and increased infection susceptibility
- Myeloneuropathy — a Vitamin-B12-deficiency-mimicking syndrome with gait ataxia, paresthesias, and posterior-column sensory loss. This presentation has been reported in patients using zinc-containing denture cream chronically and in patients on high-dose zinc supplementation without copper.
- Paradoxical impairment of testosterone, since copper is required for the activity of several enzymes in the steroidogenesis pathway and for dopamine-beta-hydroxylase in the pituitary.
The practical rule: any zinc dose above 30 mg/day taken for more than 8–12 weeks should include either 1–2 mg/day of copper supplementation or periodic monitoring of serum copper and ceruloplasmin. Most testosterone-support supplement formulations now include a small amount of copper for this reason.
Key Research Papers
- Prasad AS, Halsted JA, Nadimi M (1961). Syndrome of iron deficiency anemia, hepatosplenomegaly, hypogonadism, dwarfism and geophagia. Am J Med 31:532-546. — PubMed
- Prasad AS, Miale A Jr, Farid Z, Sandstead HH, Schulert AR (1963). Zinc metabolism in patients with the syndrome of iron deficiency anemia, hepatosplenomegaly, dwarfism, and hypogonadism. J Lab Clin Med 61:537-549. — PubMed
- Prasad AS, Mantzoros CS, Beck FW, Hess JW, Brewer GJ (1996). Zinc status and serum testosterone levels of healthy adults. Nutrition 12(5):344-348. — PubMed
- Cinar V, Polat Y, Baltaci AK, Mogulkoc R (2011). Effects of magnesium supplementation on testosterone levels of athletes and sedentary subjects at rest and after exhaustion. Biol Trace Elem Res 140(1):18-23. — PubMed
- Kilic M, Baltaci AK, Gunay M, Gokbel H, Okudan N, Cicioglu I (2006). The effect of exhaustion exercise on thyroid hormones and testosterone levels of elite athletes receiving oral zinc. Neuro Endocrinol Lett 27(1-2):247-252. — PubMed
- Brilla LR, Conte V (2000). Effects of a novel zinc-magnesium formulation on hormones and strength. J Exerc Physiol Online 3(4):26-36. — PubMed
- Wilborn CD, Kerksick CM, Campbell BI, Taylor LW, Marcello BM, Rasmussen CJ, Greenwood MC, Almada A, Kreider RB (2004). Effects of zinc magnesium aspartate (ZMA) supplementation on training adaptations and markers of anabolism and catabolism. J Int Soc Sports Nutr 1(2):12-20. — PubMed
- Steiner AZ, Hansen KR, Barnhart KT, et al. (FAZST Investigators) (2020). The effect of antioxidants on male factor infertility: the Males, Antioxidants, and Infertility (MOXI) randomized clinical trial. Fertil Steril 113(3):552-560. — PubMed
- Schisterman EF, Sjaarda LA, Clemons T, et al. (2020). Effect of folic acid and zinc supplementation in men on semen quality and live birth among couples undergoing infertility treatment: a randomized clinical trial (FAZST). JAMA 323(1):35-48. — PubMed
- Fallah A, Mohammad-Hasani A, Colagar AH (2018). Zinc is an essential element for male fertility: a review of zinc roles in men's health, germination, sperm quality, and fertilization. J Reprod Infertil 19(2):69-81. — PubMed
- Costello LC, Franklin RB (2016). A comprehensive review of the role of zinc in normal prostate function and metabolism; and its implications in prostate cancer. Arch Biochem Biophys 611:100-112. — PubMed
- Spallholz JE, Boylan LM, Larsen HS (1990). Advances in understanding selenium's role in the immune system. Ann N Y Acad Sci 587:123-139. (Plus follow-on work on Se-Zn synergy in male reproductive endocrinology.) — PubMed
PubMed Topic Searches
- Zinc + testosterone + RCT
- Zinc deficiency + hypogonadism (Prasad)
- ZMA + athletes
- Zinc + 5-alpha-reductase
- Zinc + aromatase
- Seminal zinc + sperm motility
- Zinc-induced copper deficiency
- Oyster zinc bioavailability
Connections
- Zinc Overview
- Zinc Benefits Hub
- Zinc for Immune Function
- Zinc for Wound Healing
- Zinc for Skin Health
- Copper (Critical Antagonist)
- Magnesium (ZMA Partner)
- Selenium (Sperm Quality)
- Vitamin B6 (ZMA Partner)
- Vitamin D3 (Testosterone)
- Testosterone Test
- Infertility
- Low Testosterone
- Benign Prostatic Hyperplasia
- All Minerals