Vitamin A for Skin & Cellular Differentiation
Topical and oral Vitamin A derivatives — collectively called retinoids — constitute the single most therapeutically important drug class in dermatology. Tretinoin (Retin-A) for acne and photoaging, isotretinoin (Accutane) for severe nodulocystic acne, acitretin for psoriasis, adapalene for over-the-counter acne, retinaldehyde for sensitive skin, and the retinyl esters of mass-market cosmetics all work through the same RAR/RXR nuclear receptor mechanism that drives normal keratinocyte differentiation. The same mechanism that makes retinoids so effective also makes them the most reliably teratogenic drug class known to dermatology — oral retinoids are absolutely contraindicated in pregnancy and require monthly pregnancy testing under the iPLEDGE program in the United States. This deep-dive walks through each retinoid drug, its mechanism, its place in clinical practice, and the warnings that matter most.
Table of Contents
- Retinoids and Keratinocyte Differentiation
- Topical Tretinoin (Retin-A)
- Oral Isotretinoin (Accutane) for Severe Acne
- Acitretin and Psoriasis
- Photoaging Reversal Trials
- Retinaldehyde — The Gentler Alternative
- Retinyl Esters in OTC Cosmetics
- Adapalene — OTC Synthetic Retinoid
- Pregnancy Contraindication and iPLEDGE
- Practical Patient Protocol
- Cautions
- Key Research Papers
- Connections
- Featured Videos
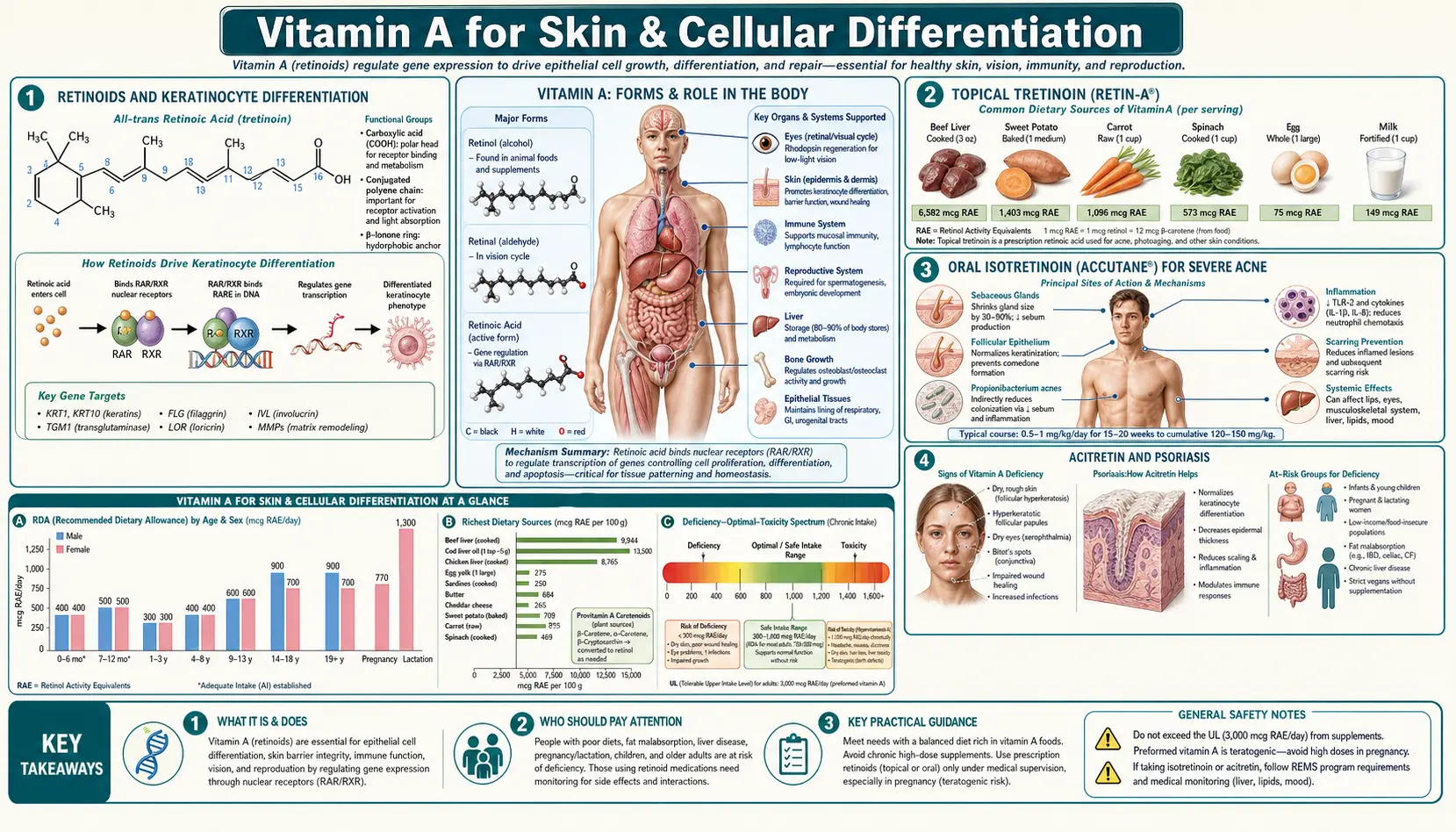
Retinoids and Keratinocyte Differentiation
The epidermis is a stratified squamous epithelium with a continuous lineage from basal keratinocytes to terminally differentiated, anucleate corneocytes that shed from the skin surface. The journey from stem-cell-like basal layer to fully cornified flake takes approximately 28 days in healthy adult skin. Retinoic acid is a master regulator of this differentiation program.
Retinoic acid binds to RAR (retinoic acid receptor) and RXR (retinoid X receptor) nuclear receptors, which heterodimerize and bind retinoic acid response elements (RAREs) in promoter regions of dozens of keratin and cornified-envelope genes. The effects on keratinocyte biology are:
- Acceleration of basal keratinocyte proliferation (the layer thickens)
- Normalization of the differentiation gradient (cells progress at the correct rate through the differentiation layers)
- Prevention of pathological hyperkeratosis (the abnormal thickening of cornified layer seen in psoriasis, ichthyosis, and acne plugs)
- Reduction of sebaceous gland output (the basis for the dramatic isotretinoin effect on acne)
- Increased dermal collagen synthesis through fibroblast effects (the basis for photoaging reversal)
- Reduction of melanocyte hyperactivity and reduction of post-inflammatory hyperpigmentation
- Suppression of matrix metalloproteinases (MMP-1, MMP-3, MMP-9) that drive collagen breakdown in photoaged skin
The same mechanism that produces these therapeutic effects also produces the characteristic irritation profile of topical retinoid use — erythema, scaling, dryness, and sting — especially during the first 4-8 weeks while the keratinocyte turnover rate normalizes. This is called "retinization" and is expected, not a sign of allergy or wrong product choice.
Topical Tretinoin (Retin-A)
Tretinoin is all-trans-retinoic acid — the same molecule produced endogenously when retinaldehyde is oxidized in the skin and other tissues. As a topical drug, tretinoin acts directly on the RAR receptors of basal keratinocytes without requiring any further metabolic conversion, which makes it the most potent (and most irritating) of the topical retinoids.
FDA-approved indications are acne vulgaris and photoaging. Available concentrations range from 0.01% through 0.025%, 0.05%, and 0.1% in cream, gel, and microsphere-encapsulated formulations. The brand name Retin-A was originally Ortho Pharmaceutical's formulation; today generic and brand variants are widely available.
Clinical use pattern:
- Start low (0.025% cream) and titrate up over weeks-months as tolerated
- Apply pea-sized amount to entire face, not just affected spots
- Apply at bedtime — tretinoin is photolabile and is degraded by daylight
- Wait 20-30 minutes after washing the face (apply to dry skin to reduce irritation)
- Use only every other night for the first 2-3 weeks to allow tolerance development
- Always pair with daily SPF 30+ sunscreen — retinized skin is more photosensitive
- Use a basic moisturizer (ceramide-based products work well) to manage retinization dryness
- Expect 8-12 weeks before peak clinical improvement
The microsphere-encapsulated formulation (tretinoin 0.025% or 0.04% Microsphere, brand name Retin-A Micro) releases the active drug more slowly, reducing peak skin concentration and substantially reducing irritation. For sensitive skin patients who cannot tolerate plain tretinoin, this is often the preferred prescription option.
For more on the disease context, see our Acne page.
Oral Isotretinoin (Accutane) for Severe Acne
Isotretinoin is 13-cis-retinoic acid — a stereoisomer of tretinoin that can be metabolized in tissue to all-trans-retinoic acid (the active RAR ligand) and to 4-oxo-isotretinoin metabolites. As an oral drug, isotretinoin produces sustained tissue exposure to retinoids and is the only treatment that can produce permanent remission of severe nodulocystic acne in a substantial fraction of patients.
Mechanism of action against acne (the four pillars of acne pathogenesis it addresses):
- Sebum reduction — isotretinoin causes apoptosis and atrophy of sebaceous glands, reducing sebum output by 80-90%. This is the central effect — without sebum, the entire downstream acne cascade is suppressed.
- Comedolysis — normalizes follicular keratinization, dissolving existing comedones and preventing new ones
- Anti-inflammatory — reduces neutrophil chemotaxis and proinflammatory cytokine production in the pilosebaceous unit
- Reduction of Cutibacterium acnes — secondary to sebum reduction; with no sebum the anaerobic bacterium loses its growth substrate
Standard course: 0.5-1.0 mg/kg/day for 16-24 weeks, targeting a cumulative dose of approximately 120-150 mg/kg total. Clinical improvement begins around week 4-6, typically with an "initial flare" period during the first month as deep nodules are mobilized. Peak benefit at week 16-20. After completing the course, approximately 50-60% of patients have permanent remission, 30% have lasting improvement but require some topical maintenance, and 10-15% relapse and may benefit from a second course.
Side effect profile is significant and predictable:
- Universal: dry lips (cheilitis), dry skin, dry eyes, dry nasal mucosa with epistaxis
- Common: elevated triglycerides and LDL cholesterol, mildly elevated liver transaminases, joint and muscle aches
- Less common: increased intracranial pressure (pseudotumor cerebri, especially with concurrent tetracycline class antibiotics — combination is contraindicated), corneal opacities, decreased night vision
- Controversial: mood changes and depression — the FDA label warns of this association, but controlled studies have not consistently demonstrated causation distinct from the impact of severe acne itself on mood
- Absolute: teratogenicity — see iPLEDGE section below
Acitretin and Psoriasis
Acitretin (brand name Soriatane) is an oral retinoid specifically developed for hyperkeratotic disorders, particularly chronic plaque psoriasis and pustular variants. It is the active metabolite of etretinate (which is no longer marketed because of its extraordinarily long half-life of 120 days).
The clinical mechanism in psoriasis is normalization of the dramatically accelerated keratinocyte turnover that defines the disease. In psoriasis, the normal 28-day epidermal turnover compresses to 3-7 days, producing the characteristic thickened plaques with silvery scale. Acitretin slows this turnover by RAR-mediated suppression of basal keratinocyte proliferation and acceleration of terminal differentiation, allowing the abnormal stratum corneum to shed and the epidermis to normalize.
Typical dosing: 25-50 mg/day orally, often combined with phototherapy (PUVA or narrow-band UVB) for synergistic effect. Clinical response begins at 4-6 weeks and peaks at 12-16 weeks. Acitretin works particularly well for pustular psoriasis, erythrodermic psoriasis, and palmoplantar variants that respond poorly to other treatments.
Side effect profile is similar to isotretinoin: dry lips, skin, and eyes; elevated triglycerides; teratogenicity. The teratogenicity warning is particularly stringent for acitretin because it can be re-esterified to long-half-life etretinate in vivo, and pregnancy must be avoided for at least 3 years after completing therapy. For this reason, acitretin is largely restricted to male patients and post-menopausal women.
For more on the disease context, see our Psoriasis page.
Photoaging Reversal Trials
The classic photoaging trials by Albert Kligman, Jonathan Weiss, and James Leyden in the late 1980s and early 1990s established topical tretinoin as the first scientifically demonstrated reversal of photoaging changes — not just prevention of further damage but actual partial reversal of accumulated damage.
Key findings from the Kligman / Weiss tretinoin photoaging trials:
- Daily 0.1% tretinoin cream applied for 6-12 months produces measurable improvements in fine wrinkles, mottled hyperpigmentation, skin roughness, and sallow color
- Improvements were objectively documented by silicone replica analysis, photography, and histology — not just subjective patient-reported outcomes
- Histologic findings showed increased basal keratinocyte proliferation, normalization of cellular atypia, increased dermal collagen synthesis, reduced solar elastosis, and increased dermal-epidermal anchoring
- Improvements continued progressively for 12+ months of treatment, then plateaued
- Discontinuation of treatment led to gradual loss of benefit over 6-12 months — tretinoin is a long-term commitment for photoaging maintenance, similar to its use for acne
For long-term anti-aging use, the typical pattern is:
- Start with 0.025% tretinoin cream nightly, titrate up to 0.05% or 0.1% as tolerated
- Combine with broad-spectrum SPF 30+ sunscreen daily — non-negotiable
- Pair with moisturizing skincare to manage retinization
- Expect 3-6 months for visible improvement; 12+ months for full benefit
- Continue indefinitely for maintained results
Lower-concentration prescription options exist for sensitive-skin patients: tazarotene 0.05% and trifarotene 0.005% (a fourth-generation retinoid). For OTC alternatives without prescription requirements, see the retinaldehyde and retinyl ester sections below.
Retinaldehyde — The Gentler Alternative
Retinaldehyde (also called retinal) is the aldehyde intermediate in the conversion of retinol to retinoic acid. Topically applied retinaldehyde is metabolized by skin enzymes (aldehyde dehydrogenases) to retinoic acid at the cellular site of action, providing the same RAR signaling as tretinoin but at a lower peak concentration — and therefore with substantially less irritation.
Comparative pharmacology:
- Tretinoin (retinoic acid): potency 100%, irritation 100% (reference)
- Retinaldehyde (retinal): potency approximately 25-50%, irritation approximately 10-25% — the favorable efficacy-to-tolerability ratio
- Retinol: potency approximately 5-10%, irritation approximately 5-10%
- Retinyl esters (retinyl palmitate, retinyl acetate): potency approximately 1-5%, irritation minimal
Retinaldehyde is available OTC in concentrations up to 0.1% in serums and creams from prestige skincare brands. Avene, La Roche-Posay, Medik8, and SkinCeuticals all offer well-formulated retinaldehyde products. The trade-off compared to prescription tretinoin is slightly slower onset (perhaps 3-4 months to peak effect instead of 8-12 weeks) and slightly lower peak benefit, in exchange for dramatically better tolerability and no prescription required.
Retinaldehyde is the typical recommendation for:
- First-time retinoid users who want to ease in
- Sensitive-skin patients who cannot tolerate tretinoin even at the lowest concentration
- Maintenance users who have completed an isotretinoin course and want a topical for long-term skin maintenance
- Patients who want anti-aging benefits without dealing with prescription logistics
Retinyl Esters in OTC Cosmetics
Retinyl palmitate and retinyl acetate are the storage forms of Vitamin A in the body (the liver stores Vitamin A primarily as retinyl palmitate in hepatic stellate cells). When applied topically, retinyl esters must be hydrolyzed to retinol, then oxidized to retinaldehyde, then oxidized again to retinoic acid before they can engage RAR receptors. Each step is enzyme-limited, so peak skin retinoic acid concentration from a retinyl ester is dramatically lower than from applied tretinoin.
The practical consequence is that retinyl ester products in mass-market cosmetics provide gentle, slow-acting anti-aging effects with minimal irritation, but require longer treatment timelines (6-12 months) to produce visible benefit comparable to a few months of prescription tretinoin. They are useful as entry-level retinoids and as maintenance products for very sensitive skin, but should not be expected to match prescription strength.
One specific cosmetic-safety concern: the FDA has reviewed but not enacted concerns about retinyl palmitate possibly increasing UV-driven skin damage when applied just before sun exposure. The mechanism is debated; some researchers have suggested retinyl palmitate may catalyze free-radical formation under UV light. The practical recommendation is to apply retinyl palmitate at bedtime (as with all retinoids) and to pair with daily sunscreen — both of which are standard retinoid practice anyway.
Adapalene — OTC Synthetic Retinoid
Adapalene (brand name Differin in the United States) is a third-generation synthetic retinoid that selectively binds RAR-beta and RAR-gamma receptors. It was approved for prescription acne use in the 1990s and was switched to over-the-counter status in the United States in 2016 — making it the only true retinoid (RAR-binding compound) available without a prescription.
Compared to tretinoin:
- Better photostability (does not degrade in daylight, so can be applied at any time)
- Better tolerability profile (less retinization in the first weeks)
- Similar efficacy for inflammatory acne
- Slightly less efficacy for comedonal acne
- Less photoaging data — the FDA approval is for acne only, not photoaging
- Available as 0.1% or 0.3% gel
For OTC retinoid users wanting predictable RAR signaling without prescription logistics, adapalene 0.1% gel is often the first recommendation. Application pattern is the same as tretinoin: pea-sized amount to dry skin, start every other night and titrate to nightly, pair with moisturizer and sunscreen.
Pregnancy Contraindication and iPLEDGE
Oral retinoids are the most reliably teratogenic drug class in dermatology. The teratogenic effect was first documented in case series in the early 1980s. The Lammer 1985 NEJM paper documented a characteristic pattern of fetal malformations from isotretinoin exposure: CNS abnormalities (hydrocephalus, microcephaly, cortical malformations), craniofacial defects (microtia/anotia, cleft palate, micrognathia), cardiac outflow tract defects (transposition of great vessels, tetralogy of Fallot), and thymic hypoplasia. Approximately 25% of isotretinoin-exposed pregnancies result in major malformations.
The U.S. response evolved over decades from voluntary patient warnings (1982) through the SMART program (System to Manage Accutane-Related Teratogenicity, 2002) to the current iPLEDGE program (2006-present), a mandatory risk evaluation and mitigation strategy (REMS) administered by the FDA:
- Both prescribers and patients must register
- Female patients of reproductive potential must commit to two simultaneous forms of contraception
- Monthly pregnancy testing required before each prescription refill
- Prescriptions are limited to 30-day supplies, must be filled within 7 days of pregnancy test
- Patient must answer monthly comprehension questions about teratogenicity
- Prescriber must verify all elements through the iPLEDGE web portal
- Pharmacy must verify all elements before dispensing
The system is logistically burdensome but has reduced isotretinoin-exposed pregnancies. The teratogenic risk persists for approximately one month after discontinuing isotretinoin (the elimination half-life of the parent drug and its metabolites). For acitretin, the recommendation is to avoid pregnancy for at least 3 years after discontinuation because of potential re-esterification to long-half-life etretinate.
Topical tretinoin and adapalene are FDA pregnancy category C — absorption through intact skin is typically very low, and observational studies have not consistently demonstrated teratogenic effect, but caution is appropriate and most dermatologists advise pausing topical retinoids in pregnancy.
Practical Patient Protocol
For acne (mild-to-moderate)
- Start: adapalene 0.1% gel OTC (Differin) or prescription tretinoin 0.025% cream
- Frequency: every other night for the first 2 weeks, then nightly
- Pair with: gentle non-comedogenic cleanser, ceramide-based moisturizer, daily SPF 30+ sunscreen
- Expect: visible improvement at 8-12 weeks, peak benefit at 4-6 months
- If insufficient response after 4 months: titrate up to tretinoin 0.05% or 0.1%, add benzoyl peroxide morning use, consider antibiotic course
For severe nodulocystic acne
- Refer to dermatology for isotretinoin evaluation
- Pre-treatment: pregnancy test (women), lipid panel, liver function tests, complete blood count
- iPLEDGE enrollment if female of reproductive potential
- Standard course: 0.5-1.0 mg/kg/day for 16-24 weeks, target cumulative dose 120-150 mg/kg
- Monthly monitoring: pregnancy test, lipids, LFTs, symptom check
For photoaging / anti-aging
- Start: retinaldehyde 0.05% serum (OTC, prestige brand) or prescription tretinoin 0.025%
- Frequency: every other night for 2 weeks, then nightly
- Pair with: vitamin C serum in the morning, daily SPF 30+ sunscreen, weekly hydrating mask
- Expect: visible improvement at 3-6 months, continued improvement through year 1, plateau thereafter
- Continue indefinitely for maintained benefit
For psoriasis (moderate-to-severe)
- Refer to dermatology
- Acitretin 25-50 mg/day, often combined with phototherapy (PUVA or NB-UVB)
- Monitoring: lipids, LFTs every 1-3 months, bone density at baseline
- Strict pregnancy avoidance for women of reproductive potential (3 years after discontinuation)
Cautions
- Teratogenicity in pregnancy — absolute for oral retinoids (isotretinoin, acitretin, bexarotene, alitretinoin). Two forms of contraception, monthly pregnancy testing, iPLEDGE program enrollment required for isotretinoin in the United States. For acitretin, contraception must continue for 3 years after discontinuation. Topical retinoids in pregnancy are typically avoided despite limited evidence of harm.
- Concurrent tetracycline antibiotics with isotretinoin — absolute contraindication; combination increases risk of pseudotumor cerebri (idiopathic intracranial hypertension) with potential vision loss. Doxycycline, minocycline, and tetracycline must be discontinued before starting isotretinoin.
- Liver disease — isotretinoin and acitretin can elevate transaminases. Pre-existing liver disease is a relative contraindication; monitoring required during treatment.
- Hypertriglyceridemia — isotretinoin and acitretin can substantially elevate triglycerides. Pre-existing severe hypertriglyceridemia is a relative contraindication; monitoring is required.
- Depression / mood symptoms with isotretinoin — FDA label warns of association; controlled studies are inconsistent. Screen all patients for baseline mood disorder and monitor during treatment.
- Bone effects with chronic retinoid use — long-term acitretin can produce diffuse interstitial skeletal hyperostosis (DISH) and bone loss. Periodic bone density screening recommended for multi-year users.
- Sun sensitivity with all topical retinoids — retinized skin is more vulnerable to UV damage. Daily broad-spectrum SPF 30+ sunscreen is non-negotiable.
- Irritation in first weeks (retinization) — expected, not allergic. Manage with reduced frequency (every 2-3 nights initially), low-strength formulation, ceramide moisturizer, gentle cleanser. Do not stop the retinoid; reduce frequency until tolerance develops.
Key Research Papers
- Lammer EJ et al. (1985). Retinoic acid embryopathy. NEJM. — PubMed
- Kligman AM et al. (1986). Topical tretinoin for photoaged skin. JAAD. — PubMed
- Weiss JS et al. (1988). Topical tretinoin improves photoaged skin. A double-blind vehicle-controlled study. JAMA. — PubMed
- Plewig G et al. (1982). Isotretinoin for acne. JAAD. — PubMed
- Goldfarb MT, Ellis CN, Voorhees JJ (1987). Topical tretinoin: its use in daily practice to reverse photoageing. British Journal of Dermatology. — PubMed
- Fisher GJ et al. (1996). Pathophysiology of premature skin aging induced by ultraviolet light. NEJM. — PubMed
- Saurat JH et al. (1994). Topical retinaldehyde on human skin: biologic effects and tolerance. JID. — PubMed
- Roenigk HH et al. (1999). Acitretin therapy for psoriasis. Archives of Dermatology. — PubMed
- Pile HD et al. (2023). Isotretinoin and the iPLEDGE program: a review. Cutis. — PubMed
- Mukherjee S et al. (2006). Retinoids in the treatment of skin aging: an overview of clinical efficacy and safety. Clinical Interventions in Aging. — PubMed
- Bagatin E et al. (2018). Adapalene 0.3% for the treatment of acne. Dermatologic Therapy. — PubMed
- Huang CK, Miller TA (2007). The truth about over-the-counter topical anti-aging products: a comprehensive review. Aesthetic Surgery Journal. — PubMed
PubMed Topic Searches
- PubMed: Topical tretinoin for acne
- PubMed: Isotretinoin nodulocystic acne
- PubMed: Acitretin psoriasis
- PubMed: Retinaldehyde topical
- PubMed: Retinoid teratogenicity
Connections
- Vitamin A Overview
- Vitamin A Benefits Hub
- Beef Liver for Vitamin A
- Vitamin A for Vision
- Vitamin A for Immune Function
- Beta-Carotene vs Preformed
- Acne
- Psoriasis
- Eczema
- Zinc (Acne, RBP Synthesis)
- Vitamin D3
- Vitamin E
- Vitamin C (Photoaging Synergy)
- Collagen
- Organ Meats
- All Vitamins