Hypocalcemia (Low Calcium): Muscle Cramps and Tetany
Most people think of calcium as a bone mineral, so it surprises them to learn that the very first warning of low blood calcium — the condition doctors call hypocalcemia — is usually felt in the muscles and nerves, not the skeleton. Muscles cramp and seize, hands and feet draw inward into stiff, claw-like spasms, and in severe cases the whole body becomes jumpy and over-triggered — a state called tetany. The reason is a quiet paradox: the calcium that builds bone is the same calcium that calms nerves, and when the level in the blood drops, nerves and muscles lose their off-switch and start firing on their own. This page explains what those cramps and spasms feel like, the surprising mechanism behind them, the two bedside tests — the Trousseau and Chvostek signs — that doctors use to catch it, and how it is corrected safely.
Table of Contents
- What Low-Calcium Cramps and Tetany Feel Like
- The Mechanism: Why Calcium Is the Nerve's Off-Switch
- Trousseau and Chvostek: the Bedside Signs
- Honest Caveat: Most Cramps Are Not Low Calcium
- Clues That Point Toward Low Calcium
- Common Situations That Cause It
- The Magnesium and Vitamin D Factors
- Getting Tested
- Correcting Low Calcium Safely
- When to Seek Care / Red Flags
- Key Research Papers
- Connections
- Featured Videos
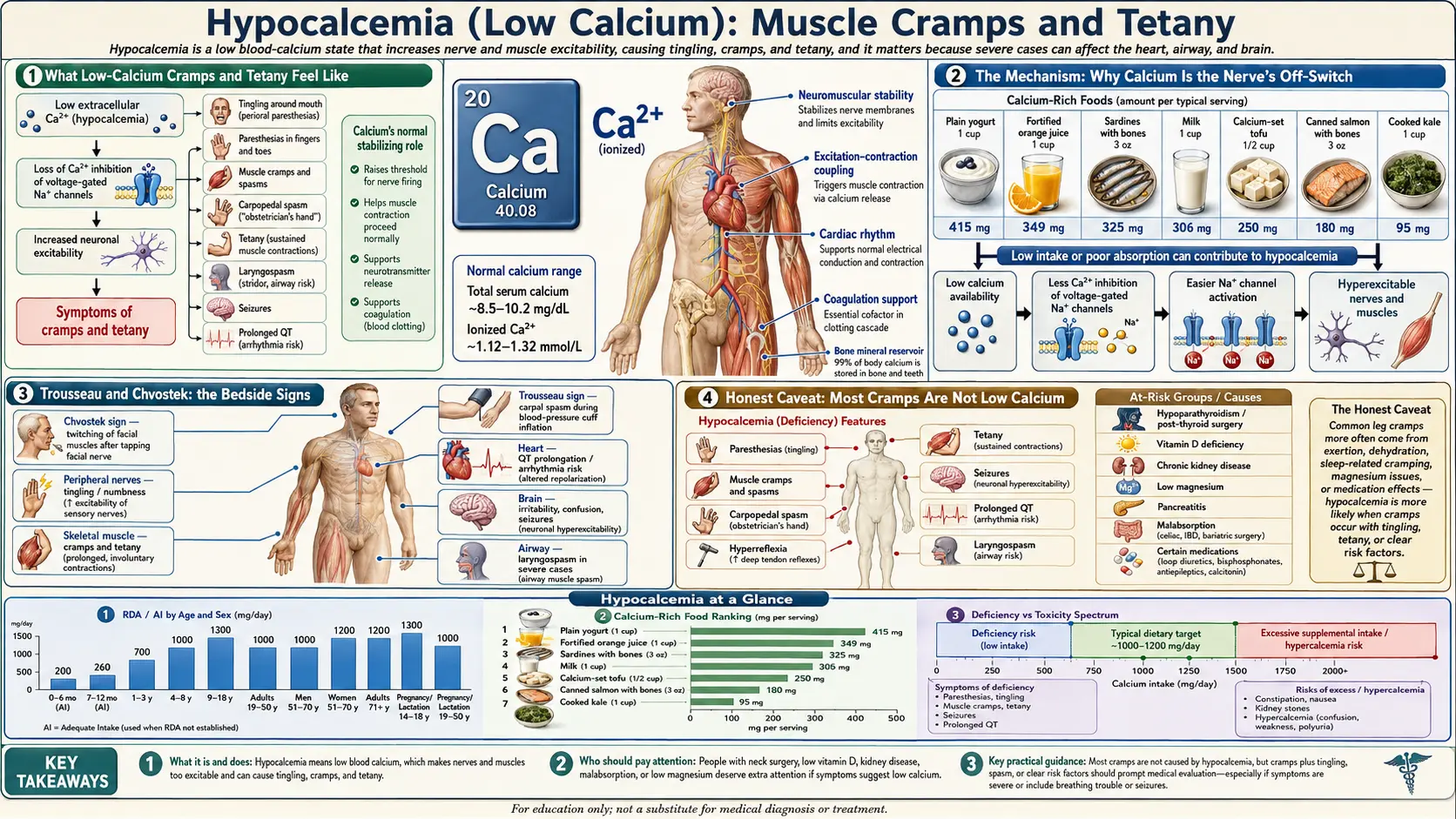
What Low-Calcium Cramps and Tetany Feel Like
The muscle symptoms of hypocalcemia sit on a spectrum, from a vague twitchiness that's easy to dismiss all the way to dramatic, frightening full-body spasms. People usually move up that spectrum as the calcium level falls, and the experience is recognizable once you know the pattern:
- Cramps and spasms — painful, involuntary tightening of a muscle that won't let go on command. The calf, foot, thigh, and hand muscles are common sites. Unlike an ordinary “charley horse” after exercise, low-calcium cramps often come at rest and can recur in clusters.
- Carpopedal spasm — the classic and most telling pattern. The hand draws into a stiff, cupped shape: the wrist and knuckles bend, the fingers straighten and press together, and the thumb pulls across the palm. The feet can do the same, arching and curling. It is involuntary, can be sustained for minutes, and is uncomfortable verging on painful.
- Perioral and facial twitching — flickering or tingling around the mouth and in the muscles of the face, sometimes the first thing noticed.
- A jumpy, “wound-up” whole body — in true tetany, the entire neuromuscular system becomes over-excitable. Light touch, a loud noise, or hyperventilating can set off a spasm. People describe feeling tightly strung, as if their muscles are primed to fire at the smallest provocation.
- Laryngospasm — at the dangerous end, the muscles of the voice box can clamp shut, producing a high-pitched, crowing breath (stridor), a sense of the throat closing, and genuine difficulty getting air. This is an emergency.
Crucially, these symptoms travel with the nerve-related complaints rather than apart from them. Tingling and numbness — especially around the lips and in the fingertips and toes (covered in detail on the sibling page Numbness & Tingling) — very often comes first and shades into the cramping and spasm as calcium drops further. If you picture a single process getting steadily louder — tingling, then twitching, then cramping, then full carpopedal spasm, then tetany — you have the natural progression of hypocalcemia.
The Mechanism: Why Calcium Is the Nerve's Off-Switch
Here is the part that genuinely surprises people. Inside a muscle fiber, calcium is what triggers a contraction — so you might reasonably expect that low calcium would make muscles weak and floppy, not cramp-prone. In fact the opposite happens, and the reason lies not inside the cell but on the outside surface of the nerve and muscle membranes.
Nerves and muscles fire by opening voltage-gated sodium channels — tiny gates that snap open to launch an electrical signal (an action potential). How easily those gates open depends on the electrical conditions right at the membrane surface, and calcium ions sit on that outer surface and stabilize it. The calcium clinging to the membrane raises the electrical threshold the cell must reach before its sodium gates will fire. In plain terms, blood calcium acts as a brake or off-switch on nerve and muscle excitability — it keeps the trigger from being too sensitive.
When blood calcium falls, that surface brake is removed. The sodium channels become “trigger-happy”: they open more easily, often without any real command from the brain, and they can fire repeatedly in a burst. Nerves discharge spontaneously; the muscles they serve receive a stream of phantom “contract” orders and seize into a cramp or sustained spasm. This is why hypocalcemia produces hyperexcitability — too much firing — rather than weakness. The classic laboratory work by Armstrong and Cota showed directly that external calcium blocks and shapes the behavior of sodium channels, the molecular basis of this membrane-stabilizing effect.
An analogy. Think of each nerve as a car with an overly sensitive accelerator. Calcium on the membrane is like a firm spring under the gas pedal — it takes a deliberate push to make the engine rev. Drop the calcium and you weaken that spring: now the lightest brush of your foot, or even a bump in the road, sends the engine racing. The nerves aren't broken and the muscles aren't out of fuel; the trigger has simply lost its resistance, so signals fire that were never intended. Restore calcium and the spring stiffens again, the accelerator settles, and the spasms stop — often within minutes of treatment.
One more wrinkle matters in practice. What counts is not total calcium but the ionized (free) calcium floating in the blood — the fraction not bound to the protein albumin. Anything that pulls more calcium onto albumin lowers the free fraction without changing the total. The most important everyday example is hyperventilation: breathing too fast (from panic, pain, or anxiety) blows off carbon dioxide, makes the blood more alkaline, and that alkalosis drives calcium onto albumin. The result is acute tetany with a perfectly normal total calcium — which is why a panic attack can produce tingling hands and carpopedal spasm in someone whose calcium stores are fine.
Trousseau and Chvostek: the Bedside Signs
Because hypocalcemia makes nerves over-excitable, doctors can provoke that excitability on purpose with two simple, century-old bedside tests. You may see them performed, and understanding them demystifies the exam:
- Trousseau sign — a blood-pressure cuff is inflated on the upper arm above the systolic pressure and held for up to three minutes. In hypocalcemia, the reduced blood flow and the irritable nerves combine to trigger the hand into the classic carpopedal spasm: wrist flexed, fingers straight and pressed together, thumb drawn in. It is considered the more reliable of the two signs.
- Chvostek sign — the examiner taps over the facial nerve just in front of the ear. A positive response is a twitch of the facial muscles, from a small flicker at the corner of the mouth up to a contraction of the whole side of the face. It is quicker to test but less specific.
An honest word about these signs: they are useful flags, not proof. The Chvostek sign in particular is imperfect — a meaningful share of perfectly healthy people show a mild positive twitch, while some people with genuine, significant hypocalcemia show none. A careful study by Hujoel found only a weak relationship between Chvostek positivity and the actual serum calcium level. So a positive sign raises suspicion and prompts a blood test; it does not by itself diagnose or exclude low calcium. The Trousseau sign is the sturdier of the two but still has to be confirmed with a laboratory calcium measurement.
Honest Caveat: Most Cramps Are Not Low Calcium
It is important to be straight about this, because the internet is full of advice to “take calcium for cramps,” and for most people that is the wrong answer. The overwhelming majority of ordinary muscle cramps have nothing to do with hypocalcemia. Common everyday cramps — the nighttime calf cramp, the foot cramp, the cramp during or after hard exercise — usually arise from other causes entirely:
- Benign nocturnal leg cramps — extremely common, especially with age, and in most cases no abnormality is ever found.
- Exercise-associated muscle cramps — the leading explanation today is not dehydration or salt loss but neuromuscular fatigue altering the reflexes that control muscle length, as reviewed by Miller and colleagues.
- Other electrolyte problems — low potassium and especially low magnesium are more frequent culprits for cramping than low calcium, and the three are intertwined.
- Medications — diuretics (“water pills”), statins, and some asthma inhalers are associated with cramps.
- Medical conditions — pregnancy, peripheral artery disease, nerve compression, hypothyroidism, and kidney disease all cause cramps; so do simple dehydration and prolonged sitting.
So this page is not claiming that a cramp means your calcium is low — in an otherwise well person, that is unlikely. What hypocalcemia tends to produce is a distinctive pattern: cramps plus tingling around the mouth and in the fingertips, plus the hand-and-foot carpopedal spasm, plus a sense of the whole body being wound up — usually in someone with a reason to be low (recent neck surgery, low vitamin D, low magnesium, kidney disease). It is that cluster, in the right context, that points to low calcium — not an isolated calf cramp on its own.
Clues That Point Toward Low Calcium
If cramps and spasms are common and rarely about calcium, what should make you — or your doctor — think specifically of hypocalcemia? A few features shift the odds:
- The company the cramps keep. Hypocalcemic cramps rarely travel alone. The strong clue is cramping together with tingling and numbness around the lips and in the fingers and toes (see Numbness & Tingling). That nerve-and-muscle combination is far more suggestive than a cramp by itself.
- Carpopedal spasm. The cupped, claw-like hand spasm is a much more specific finding than a calf cramp. If hands or feet draw inward and stay there, low calcium (or the hyperventilation form described above) climbs the list quickly.
- A reason to be low. Recent thyroid or neck surgery (which can injure or remove the parathyroid glands), known low vitamin D, known low magnesium, chronic kidney disease, or a history of parathyroid problems all make hypocalcemia plausible rather than far-fetched.
- Heart and rhythm symptoms alongside. Low calcium also lengthens the heart's electrical recovery (the QT interval), so cramps appearing with palpitations or lightheadedness deserve prompt attention — see the sibling page on Heart Rhythm & QT.
- A positive bedside sign. A clear Trousseau sign, or facial twitching on tapping (Chvostek), in someone with the right story is enough to send for a calcium level right away.
None of these prove hypocalcemia — that takes a blood test — but together they separate the rare cramp that warrants a calcium check from the common cramp that does not.
Common Situations That Cause It
When blood calcium really is low, there is almost always an identifiable reason. The body normally defends its calcium level tightly using parathyroid hormone (PTH) and vitamin D, so hypocalcemia points to a problem in one of those systems or to an unusual loss or shift of calcium. The main causes:
- Hypoparathyroidism — too little PTH, the hormone that normally raises calcium. By far the most common cause is injury to or accidental removal of the parathyroid glands during neck (thyroid) surgery. This is the single most frequent reason hospitalized patients develop symptomatic hypocalcemia, and it can appear within a day of the operation. (Less commonly the glands fail from autoimmune disease or a genetic disorder.)
- Vitamin D deficiency — vitamin D is required to absorb calcium from food. Severe, prolonged deficiency lowers calcium and, over time, softens bone (osteomalacia in adults, rickets in children). This is a global problem and a common cause worldwide. See Vitamin D3.
- Low magnesium — magnesium deficiency both blunts the release of PTH and makes tissues resistant to it, so calcium falls and — importantly — won't correct until the magnesium is fixed (see the next section).
- Chronic kidney disease — failing kidneys cannot activate vitamin D properly and retain phosphate, both of which drag calcium down. Hypocalcemia is common in advanced kidney disease.
- Acute illness — severe pancreatitis, widespread infection (sepsis), and large transfusions of stored blood (whose preservative binds calcium) can all drop calcium acutely in the hospital.
- Respiratory alkalosis from hyperventilation — as described in the mechanism section, fast breathing during a panic attack lowers ionized calcium and can cause acute tetany even when the total calcium is normal.
Pinning down which of these is at work matters, because the fixes differ enormously — replacing vitamin D, correcting magnesium, and managing post-surgical hypoparathyroidism are entirely different paths.
The Magnesium and Vitamin D Factors
Two related minerals deserve a section of their own because they so often sit behind a low calcium — and because ignoring them is the classic reason calcium “won't come up.”
Magnesium. Magnesium is required for the parathyroid glands to release PTH and for the body's tissues to respond to it. When magnesium is low — common with diuretics, alcohol use, poor intake, or gut losses — PTH output falls and calcium drops with it. The crucial clinical point, well described by Agus, is that this kind of hypocalcemia is refractory: it resists calcium replacement and will not normalize until the magnesium is corrected. For patients, the takeaway is that “just take calcium” can fail outright, and a stubborn low calcium should prompt a magnesium check. (A standard metabolic panel does not include magnesium, so it must be ordered separately.) See Magnesium Replenishment.
Vitamin D. Vitamin D is the key that lets the gut absorb calcium from food. Without enough of it, even a calcium-rich diet leaves the blood level struggling, and severe deficiency is a leading worldwide cause of hypocalcemia, as Holick's widely cited review lays out. Because vitamin D status is so central, a vitamin D blood test is a routine part of working up a low calcium, and replacing vitamin D is often the durable fix. (Vitamin K2 is frequently discussed alongside D for directing calcium into bone rather than soft tissue, though its role is in bone metabolism rather than in raising a low blood calcium acutely.)
Getting Tested
Confirming — or excluding — hypocalcemia as the cause of cramps is quick and inexpensive. A Comprehensive Metabolic Panel (CMP), a routine blood draw, reports the total serum calcium (normal roughly 8.5–10.5 mg/dL, though laboratories vary) alongside albumin, kidney function, and glucose. Because most calcium in the blood rides on albumin, a low albumin makes the total calcium look falsely low; clinicians either apply a corrected-calcium calculation or, better, measure the ionized (free) calcium directly — the value that actually determines symptoms.
If calcium really is low, the next tests sort out why: a parathyroid hormone (PTH) level (low or inappropriately normal PTH points to hypoparathyroidism; high PTH points to vitamin D deficiency or kidney disease), a vitamin D level, a magnesium level (ordered separately, since the CMP omits it), and a phosphate level. When the heart is a concern, an electrocardiogram (ECG) checks for the prolonged QT interval that low calcium causes. The reassuring message is that one cheap blood panel both settles whether calcium is the problem and launches the search for the cause.
Correcting Low Calcium Safely
How calcium is replaced depends entirely on how low it is and how severe the symptoms are. The guiding rule is to match the urgency to the danger — calm and oral for mild cases, intravenous and monitored for tetany or seizures.
- Acute, symptomatic hypocalcemia (tetany, seizures, laryngospasm, prolonged QT) is a hospital emergency treated with intravenous calcium (calcium gluconate) under heart-rhythm monitoring. The carpopedal spasm and tingling typically ease within minutes as the free calcium rises. This is not something to manage at home.
- Oral calcium and active vitamin D are the mainstay for ongoing or milder hypocalcemia — for example after thyroid surgery or in hypoparathyroidism. Calcium supplements (often calcium carbonate or citrate) are paired with vitamin D, and in hypoparathyroidism specifically with the activated form of vitamin D (calcitriol), because without PTH the body cannot activate ordinary vitamin D well. Dosing is prescribed and monitored.
- Fix the magnesium first. If magnesium is low, it is replaced alongside (or before) the calcium — otherwise the calcium simply will not stay up.
- Treat the cause. Replacing vitamin D when it is deficient, managing kidney disease, or adjusting a contributing medication is what makes the correction last rather than temporary.
- Food matters but is rarely enough alone for true hypocalcemia. Calcium-rich whole foods — yogurt, milk, sardines (with bones), kale, broccoli, and almonds — support healthy calcium status and are the right long-term foundation, but a diagnosed low blood calcium needs supplements and treatment of the cause, not diet alone.
A caution in the other direction: more is not better. Pushing calcium and vitamin D too hard can swing the level too high (hypercalcemia), so replacement — especially in hypoparathyroidism — is deliberately titrated and rechecked rather than maximized.
When to Seek Care / Red Flags
Most muscle cramps are harmless and are not about calcium at all. But a specific cluster of symptoms signals possible acute, severe hypocalcemia, which is a medical emergency. Seek emergency help right away — call emergency services, not a routine appointment — for any of the following:
- A seizure — severe hypocalcemia can trigger seizures even in people without epilepsy.
- Difficulty breathing, a sense of the throat closing, or a high-pitched crowing breath (stridor) — a sign of laryngospasm, which is life-threatening.
- Sustained whole-hand or whole-foot spasm (carpopedal spasm) that won't relax, especially with widespread tingling and a wound-up, jumpy feeling — the picture of frank tetany.
- Palpitations, fainting, or lightheadedness alongside cramps — low calcium can destabilize the heart's rhythm (see Heart Rhythm & QT).
- Confusion or marked irritability developing with the muscle symptoms.
- Cramps and spasms in the days after thyroid or neck surgery — expect and report these, as they signal post-surgical hypocalcemia that needs prompt treatment.
For milder, recurrent cramps without these danger signs — particularly if they come with persistent tingling, or if you have low vitamin D, kidney disease, or take a diuretic — it is reasonable to see your doctor and ask for a calcium, magnesium, and vitamin D check. Confirming or ruling out hypocalcemia takes a single, low-cost blood test.
Key Research Papers
- Cooper MS, Gittoes NJL (2008). Diagnosis and management of hypocalcaemia. BMJ;336(7656):1298-1302. — DOI: 10.1136/bmj.39582.589433.BE
- Schafer AL, Shoback DM (2016). Hypocalcemia: Diagnosis and Treatment. Endotext (NCBI Bookshelf). — PubMed
- Shoback D (2008). Hypoparathyroidism. New England Journal of Medicine;359(4):391-403. — DOI: 10.1056/NEJMcp0803050
- Peacock M (2010). Calcium Metabolism in Health and Disease. Clinical Journal of the American Society of Nephrology;5(Suppl 1):S23-S30. — DOI: 10.2215/CJN.05910809
- Goltzman D, Mannstadt M, Marcocci C (2018). Physiology of the Calcium-Parathyroid Hormone-Vitamin D Axis. Frontiers of Hormone Research;50:1-13. — DOI: 10.1159/000486060
- Armstrong CM, Cota G (1999). Calcium block of Na+ channels and its effect on closing rate. Proceedings of the National Academy of Sciences;96(7):4154-4157. — DOI: 10.1073/pnas.96.7.4154
- Jesus JE, Landry A (2012). Chvostek's and Trousseau's Signs. New England Journal of Medicine;367(11):e15. — DOI: 10.1056/NEJMicm1110569
- Hujoel IA (2016). The association between serum calcium levels and Chvostek sign. Neurology Clinical Practice;6(4):321-328. — DOI: 10.1212/cpj.0000000000000270
- Miller KC, McDermott BP, Yeargin SW, et al. (2022). An Evidence-Based Review of the Pathophysiology, Treatment, and Prevention of Exercise-Associated Muscle Cramps. Journal of Athletic Training;57(1):5-15. — DOI: 10.4085/1062-6050-0696.20
- Agus ZS (1999). Hypomagnesemia. Journal of the American Society of Nephrology;10(7):1616-1622. — DOI: 10.1681/ASN.V1071616
- Clarke BL (2018). Epidemiology and Complications of Hypoparathyroidism. Endocrinology and Metabolism Clinics of North America;47(4):771-782. — DOI: 10.1016/j.ecl.2018.07.004
- Holick MF (2007). Vitamin D Deficiency. New England Journal of Medicine;357(3):266-281. — DOI: 10.1056/NEJMra070553
PubMed Topic Searches
- PubMed — Hypocalcemia, tetany, and carpopedal spasm
- PubMed — Trousseau and Chvostek signs in hypocalcemia
- PubMed — Hypocalcemia after thyroidectomy and hypoparathyroidism
- PubMed — Hypomagnesemia and refractory hypocalcemia
- PubMed — Respiratory alkalosis, hyperventilation, and tetany
Connections
- Hypocalcemia Symptom Hub
- Hypocalcemia and Numbness & Tingling
- Hypocalcemia and Heart Rhythm & QT
- Hypocalcemia and Bone Loss
- Calcium Overview
- Calcium and Muscle Function
- Calcium and Nerve Transmission
- Magnesium
- Magnesium Replenishment
- Potassium
- Vitamin D3
- Vitamin K2
- Comprehensive Metabolic Panel
- Vitamin D Test
- Hyperparathyroidism
- Epilepsy / Seizures
- Arrhythmia
- Heart Palpitations
- Kidney Disease
- Yogurt
- Sardines
- Kale