Full-Body MRI Screening: Benefits, Limits, Incidentalomas, and Whether to Get One

Full-body MRI screening — offered by services such as Prenuvo, Ezra, SimonMed, and an expanding list of clinics — uses a single magnetic-resonance scan lasting roughly 30 to 60 minutes to image nearly every organ system from the skull base to the pelvis, without radiation and without iodinated contrast. Proponents argue this can detect tumors, aneurysms, neurodegeneration, musculoskeletal disease, and early organ pathology years before symptoms. Critics argue it leads to widespread detection of incidental findings that produce anxiety, additional testing, biopsies, and occasionally harm without meaningful life extension.
Both sides have legitimate points. This article walks through what full-body MRI actually finds, the evidence base, typical findings and their real clinical significance, cost, and how to decide whether it makes sense for you.
Table of Contents
- How Full-Body MRI Works
- Major Providers
- What It Actually Finds
- The Incidentaloma Problem
- What the Evidence Supports and Doesn’t
- Reasonable Candidates
- When It’s Probably Not Worth It
- Cost and Insurance
- Connections
- Featured Videos
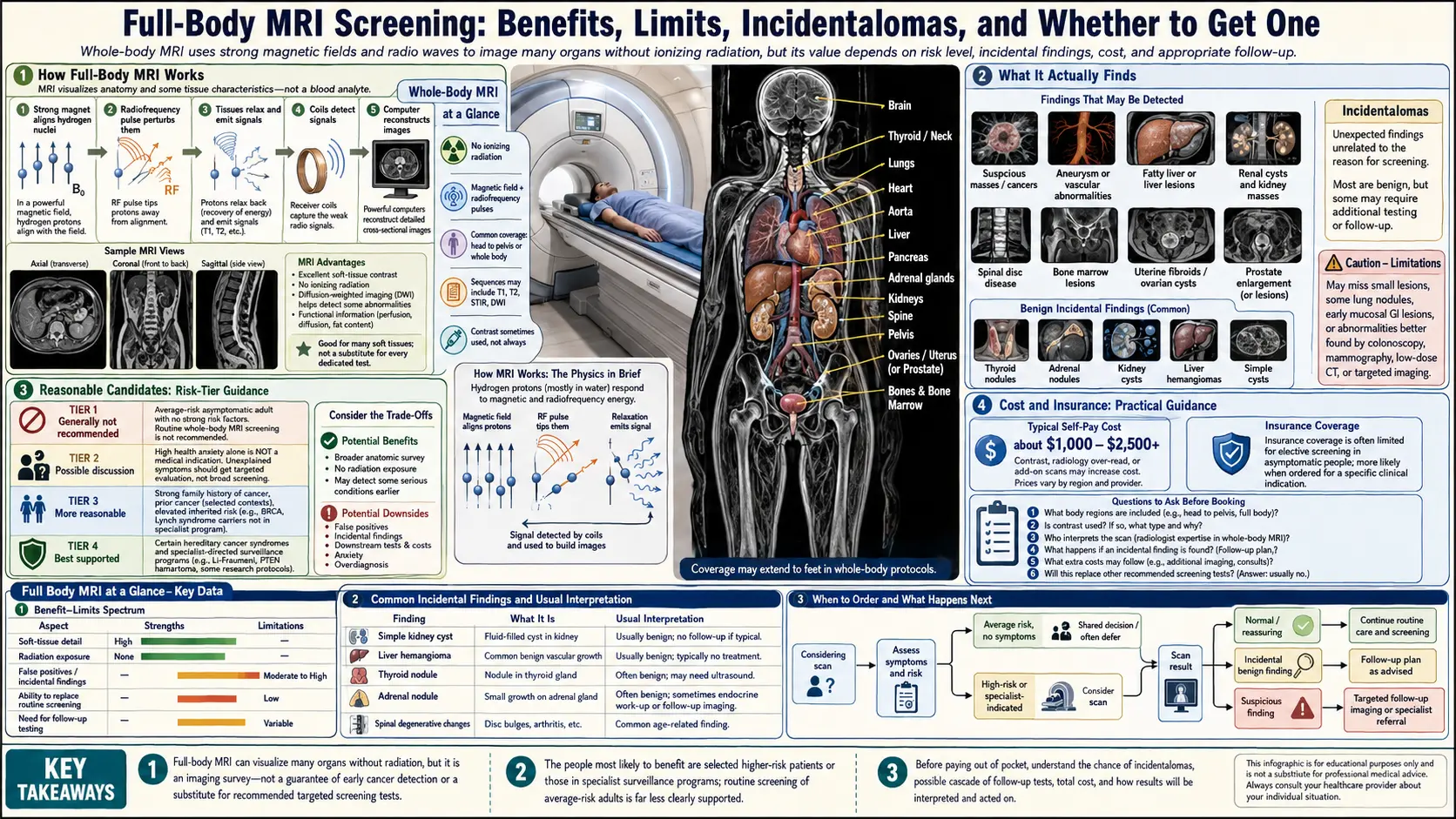
How Full-Body MRI Works
Standard MRI uses magnetic fields and radio-frequency pulses to generate detailed images of soft tissue without ionizing radiation. Screening protocols combine rapid sequences (T1-weighted, T2-weighted, diffusion-weighted, STIR) across the whole body, interpreted by radiologists often aided by AI pre-reads. No contrast is used for most screening protocols (avoiding gadolinium retention concerns). The scan itself is claustrophobic for some patients and involves lying still in a loud magnet bore.
Major Providers
- Prenuvo — Flagship full-body MRI at ~60 minutes, roughly $2,500 list price with variable bundling.
- Ezra — Offers 30-, 45-, and 60-minute scans across organ-system packages; ~$1,500–2,500.
- SimonMed, Premier Health, academic medical centers — Sometimes lower-cost standalone scans.
What It Actually Finds
In large published cohorts, full-body MRI detects one of the following in approximately the fractions shown:
- Potentially actionable findings (true abnormalities likely meaningful): 1–3% of scans. Includes some early cancers, significant aneurysms, and meaningful organ pathology.
- Incidentalomas requiring follow-up: 15–35% of scans. Benign cysts, hemangiomas, fibroids, small thyroid nodules, benign masses.
- Clearly benign but reported findings: Very common.
The Incidentaloma Problem
Incidentalomas — abnormalities found incidentally without any symptom pointing to them — are the central critique of broad screening. Most are benign and clinically meaningless, but once found they cannot be unseen. Follow-up imaging, biopsies, surgeries, and anxiety accumulate, and a meaningful minority of patients experience procedural complications from investigating findings that would never have caused harm. This is the concept of overdiagnosis — detecting disease that would never have manifested.
What the Evidence Supports and Doesn’t
No randomized trial has shown that routine full-body MRI screening reduces cancer-specific or all-cause mortality in asymptomatic average-risk adults. Detection rates of early cancer are real but modest; it is not yet established that earlier detection in this heterogeneous pathway translates to survival benefit in the way that, for example, mammography or colonoscopy have been shown to in specific populations. The technology is powerful; the evidence base for screening unselected adults is young. Major cancer societies do not yet endorse full-body MRI for general screening.
Reasonable Candidates
- Strong family history of cancer at young ages, particularly genetic predispositions (Li-Fraumeni, hereditary breast/ovarian, Lynch syndrome) — in some cases formally recommended as part of screening protocols.
- People with prior cancers at elevated risk of recurrence.
- Symptom-directed concern that primary-care workup has not resolved.
- Patients prepared psychologically and financially for the follow-up testing that incidental findings trigger.
When It’s Probably Not Worth It
- Healthy low-risk adults seeking reassurance — the false-positive and incidentaloma burden often outweighs benefit.
- People with high anxiety who would find any incidental finding distressing.
- People without access or willingness to navigate the downstream follow-up system.
- Situations where basic preventive care (colonoscopy, mammography, blood pressure, ApoB, calcium score) is incomplete — those established tests have better evidence and should come first.
Cost and Insurance
Out-of-pocket costs range from roughly $1,500 to $2,500 in the United States. Insurance coverage is generally limited to people with specific genetic high-risk designations or symptoms. HSAs and FSAs may cover portions. Comparative value: the same amount spent on Coronary Calcium, ApoB, Lp(a), colonoscopy, and a few other targeted tests typically delivers more predictive information per dollar for most healthy adults.
Research Papers and References
The following are curated PubMed literature searches covering the evidence base for whole body MRI screening testing, interpretation, and clinical management. Each link opens a live, filtered PubMed query so the results stay current as new studies are indexed.
- Whole body MRI screening — PubMed literature search
- Incidentaloma management — PubMed literature search
- Prenuvo whole body MRI — PubMed literature search
- Whole body MRI cancer screening — PubMed literature search
- Li-Fraumeni syndrome MRI screening — PubMed literature search
- MRI false positive rate — PubMed literature search
- Whole body MRI BRCA — PubMed literature search
- Asymptomatic screening MRI — PubMed literature search
- Screening overdiagnosis imaging — PubMed literature search
- Whole body MRI multiple myeloma — PubMed literature search
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- Coronary Calcium Score
- Cancer
- ApoB
- Soft Plaque and CAC Limitations
- MESA Risk Calculator and Age Percentiles
- Agatston Score Calculation and Interpretation
- CAC Zero and the Power of Negative Result
- Lipoprotein(a)
- Lipid Panel
- Anxiety
- Multiple Myeloma
- Calcium
- Complete Blood Count
- Cancer Treatment
- Laparoscopy Excision vs Ablation
- Ovarian Cysts
- ANA dsDNA and Lupus Autoantibodies