Agatston Score: How the Coronary Calcium Number Is Calculated
The Agatston score is the standard way coronary artery calcium is reported. It's named after Arthur Agatston, the Florida cardiologist who first described the method in 1990 (and who later wrote The South Beach Diet). The score combines two attributes of every calcified lesion in your coronary arteries — how big it is, and how dense it is — into a single weighted number, summed across all coronary territories. Understanding the math is useful because it explains why some scores rise even as plaque stabilizes, why volume scoring is sometimes preferred over Agatston, and why a single number conceals a lot of clinical detail.
Table of Contents
- What Counts as Coronary Calcium
- The 130 HU Threshold
- The Density Factor (1–4)
- The Calculation, Lesion by Lesion
- Total Score and Vessel Distribution
- Calcium Volume Score
- Calcium Mass Score
- Standard Interpretation Bands
- Vessel Distribution Matters
- Interpretation Pitfalls
- Research Papers and References
- Connections
- Featured Videos
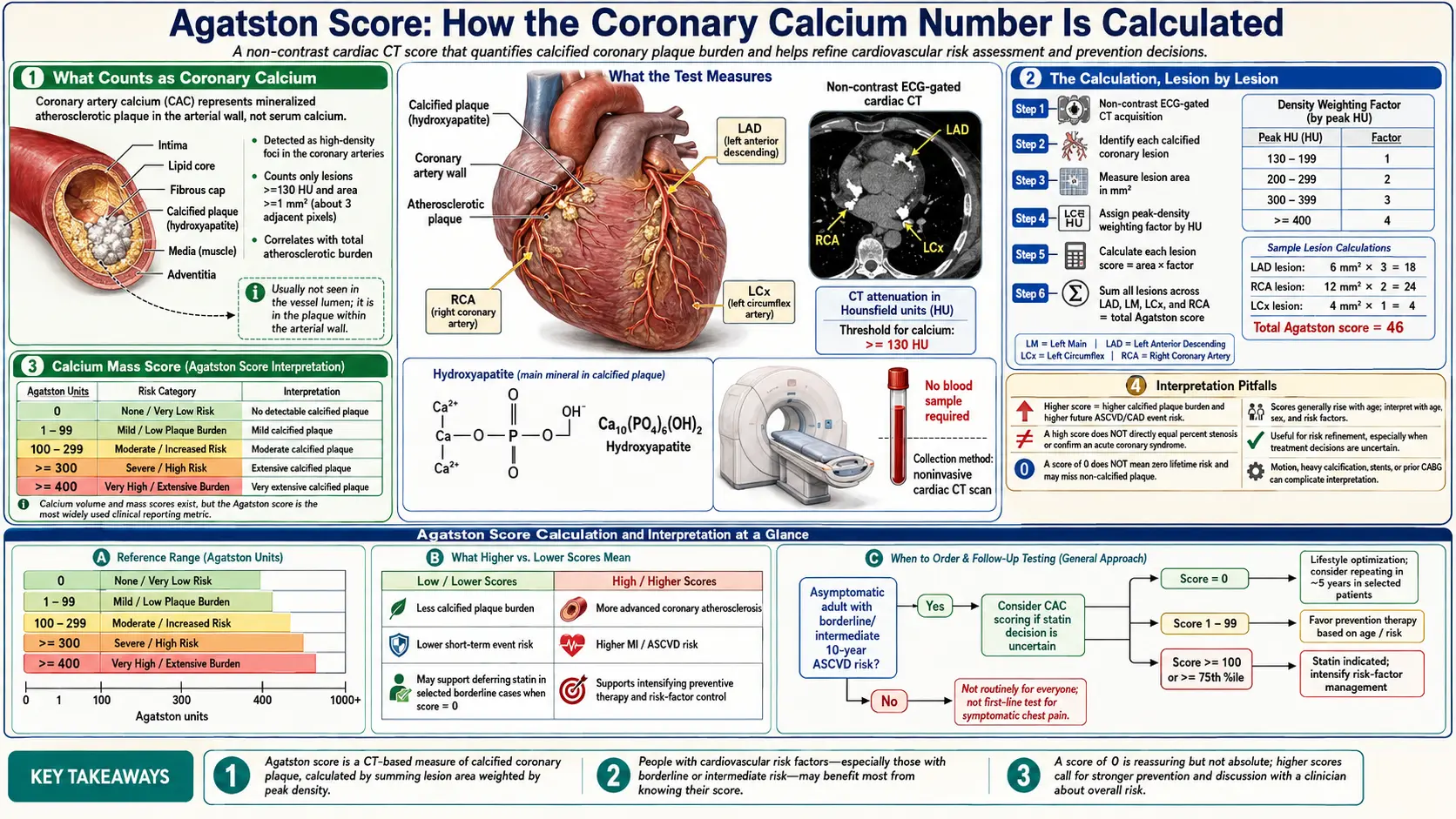
What Counts as Coronary Calcium
Coronary calcium is calcified atherosclerotic plaque in the wall of the coronary arteries. It is the body's stabilization response to mature atherosclerotic lesions: smooth-muscle-derived osteoblast-like cells deposit hydroxyapatite (the same mineral as bone) within and around the lipid core of an established plaque. Calcium volume tracks total plaque burden, especially in older lesions. It does not track soft plaque, vulnerable plaque, or very early atheroma — those are CAC's blind spot.
The CT scan that generates the Agatston score is a non-contrast, EKG-gated chest CT. The scanner produces a stack of axial images through the heart; software identifies all voxels that exceed a defined density threshold within the anatomic territory of the four major coronary arteries: the Left Main (LM), the Left Anterior Descending (LAD), the Left Circumflex (LCX), and the Right Coronary Artery (RCA).
The 130 HU Threshold
CT density is measured in Hounsfield Units (HU), with water defined as 0 HU and air as -1000 HU. Bone and calcified plaque are highly attenuating, falling in the +130 HU and above range. The Agatston method counts a voxel as “calcified” if its density is at least 130 HU and the lesion contains at least 3 contiguous pixels (an area of approximately 1 mm²).
The 130 HU threshold is not arbitrary — it is set above noise from blood pool artifacts and below the density of frank bone, isolating lesions whose density is consistent with plaque calcification. The threshold has been preserved through generations of CT scanner technology to keep scores comparable across decades and machines.
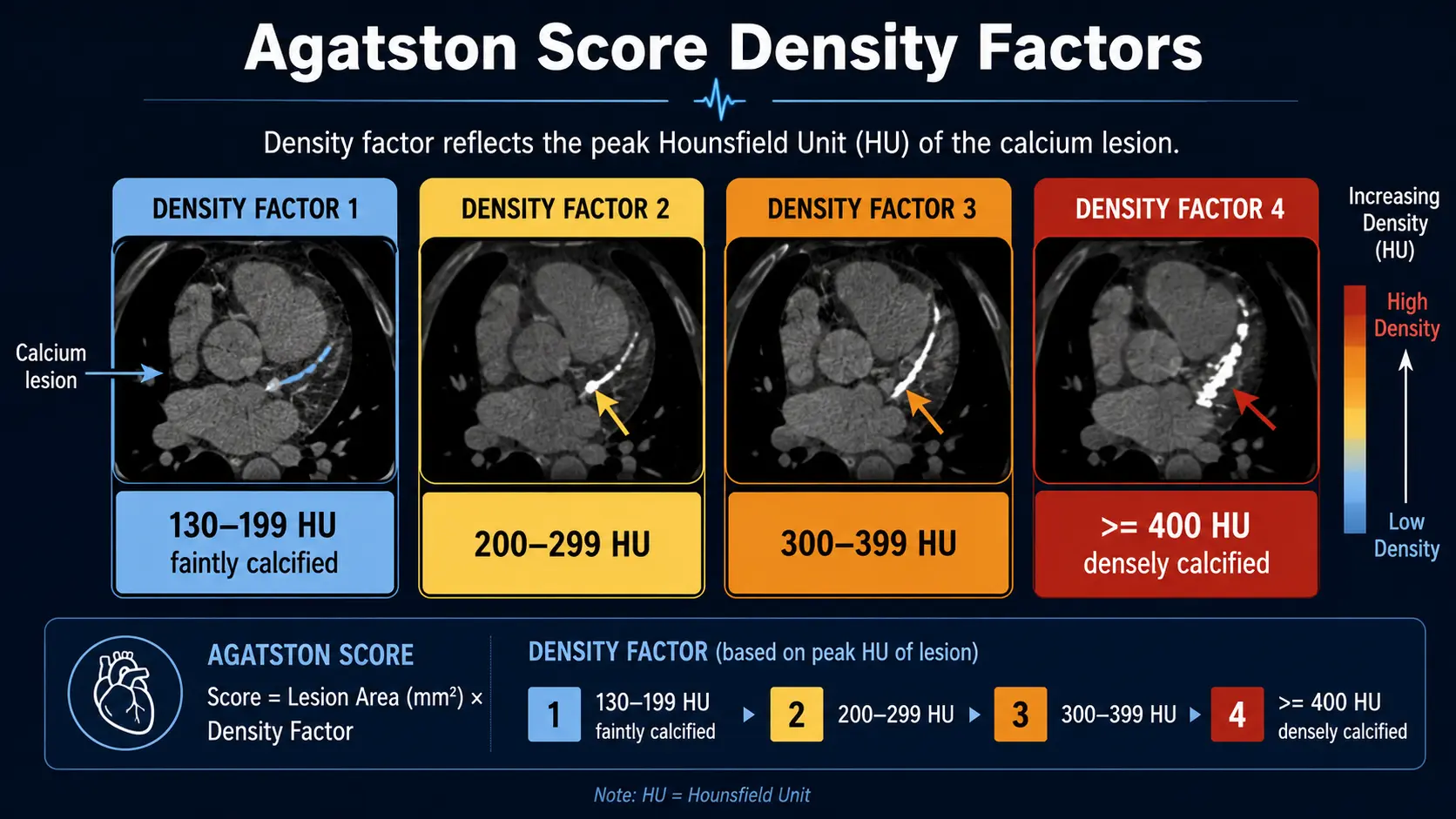
The Density Factor (1–4)
For each calcified lesion, the maximum Hounsfield Unit value within the lesion is recorded and converted to a density factor:
- 1 — peak density 130–199 HU (faintly calcified)
- 2 — peak density 200–299 HU
- 3 — peak density 300–399 HU
- 4 — peak density ≥400 HU (densely calcified)
This is the source of one of the more counterintuitive properties of the Agatston score: denser calcium gets a higher score. Densely calcified plaques are typically older and more stable — less likely to rupture and cause an acute event — than younger, less-dense (and partly soft) plaque. Statin therapy famously increases calcification density even as it reduces clinical events. The Agatston score, by design, can rise on statins for this reason.
The Calculation, Lesion by Lesion
For each calcified lesion in each coronary artery:
Lesion score = Lesion area (mm²) × Density factor
For example, a 4 mm² lesion in the LAD with a peak density of 250 HU (density factor 2) contributes a lesion score of 4 × 2 = 8 to the total. A 10 mm² lesion at 450 HU (density factor 4) contributes 40.
The total Agatston score is simply the sum of lesion scores across all lesions in all coronary arteries. There is no upper bound — scores in the 1000–3000 range are common in elderly patients with diabetes or familial hypercholesterolemia, and scores above 5000 occasionally appear.
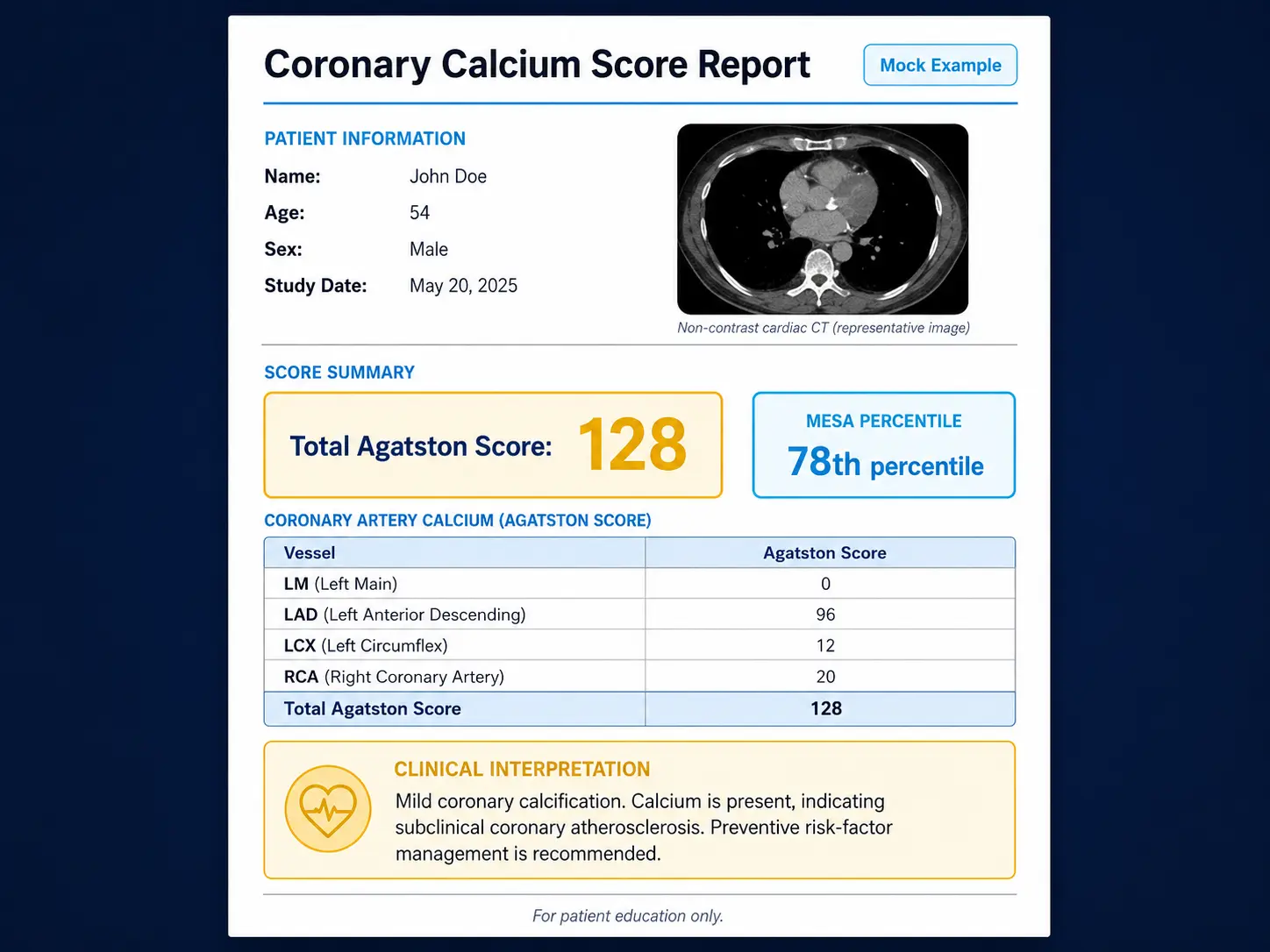
Total Score and Vessel Distribution
Radiology reports typically include:
- The total Agatston score
- Per-vessel scores: LM, LAD, LCX, RCA
- Number of lesions per vessel
- Age and sex percentile (using MESA data)
- Calcium volume score
- Sometimes a calcium mass score
The per-vessel breakdown matters more than the absolute score in some cases. Calcification in the Left Main coronary artery has different prognostic weight than the same volume of calcification in the LAD or RCA, because Left Main disease can compromise the supply to a much larger area of myocardium.
Calcium Volume Score
The volume score is the total volume of calcified plaque in cubic millimeters, calculated by summing voxel volumes above the 130 HU threshold. Unlike the Agatston score, volume scoring does not weight by density. This makes volume scoring more sensitive to changes in plaque burden over serial scans because it is not confounded by the density-shift artifact of stabilization.
Some research centers and longitudinal studies report calcium volume rather than Agatston score for follow-up scans because volume changes are more interpretable. Most clinical reports still use Agatston for absolute interpretation against established percentile tables.
Calcium Mass Score
The mass score is calculated by summing voxel-by-voxel calcium hydroxyapatite mass, calibrated against a phantom of known density included in the scan. Mass is the most physiologically meaningful unit of plaque burden but requires phantom calibration, which is not universal. Mass scoring is mostly a research tool.
Standard Interpretation Bands
The widely-used Agatston interpretation bands:
- 0 — No detectable coronary calcium. 10-year cardiovascular event risk <1% in most populations.
- 1–10 — Trivial calcification. Some prefer to consider this still “essentially zero” for practical decisions.
- 11–100 — Mild plaque. 10-year event risk approximately 1.5–2%.
- 101–400 — Moderate plaque. 10-year event risk 2.5–5%; statin recommended in most guidelines.
- 401–1000 — Significant disease. 10-year event risk 5–10%; aggressive prevention.
- >1000 — Extensive disease. 10-year event risk often >10%; cardiology evaluation, consideration of stress testing or CT angiography.
These bands are population averages. The MESA percentile (see MESA Calculator page) reframes the absolute number against age-and-sex norms, often providing a more clinically meaningful interpretation.
Vessel Distribution Matters
Two patients with identical Agatston scores can have very different prognoses depending on vessel distribution:
- Diffuse multi-vessel calcification (LAD + LCX + RCA + LM) suggests a generalized atherosclerotic process and a higher event rate
- Single-vessel disease (e.g., all calcium in the LAD) is more localized but has its own implications for what regions of myocardium would be affected by an event
- Left Main involvement at any score warrants particular attention because of the size of the vascular bed served
- Proximal LAD calcification is more clinically significant than distal LAD calcification of the same volume because of the territory at risk
A 200-Agatston score with all calcification in the proximal LAD is more concerning than a 300-Agatston score with calcium spread across the distal LCX and distal RCA branches.
Interpretation Pitfalls
- Statin-induced density rise — a score that climbs from 250 to 350 in 5 years on statins likely reflects stabilization (denser, more stable plaque) rather than progression
- Misclassification of non-coronary calcium — mitral valve, pericardial, or aortic valve calcification can occasionally be miscounted; modern scanners and software correct for this
- Movement artifact — high heart rates or arrhythmia can blur images; beta-blockade is sometimes used to lower heart rate before scan
- Stent or pacemaker artifact — metal hardware creates blooming artifact; CAC scoring is less useful in patients with prior stents or device leads
- Background coronary calcification scoring — population norms are derived from the MESA cohort; ethnic-specific norms differ
- Single threshold — some emerging research questions whether a continuous calcium-density scale would outperform the four-bin density factor; current Agatston methodology preserves comparability
Research Papers and References
- Original Agatston methodology — PubMed search
- Volume score vs Agatston score — PubMed search
- Density and statin stabilization — PubMed search
- Vessel-specific calcium prognosis — PubMed search
- 130 HU threshold — PubMed search
External Authoritative Resources
- American Heart Association
- American College of Cardiology
- MESA Study (Multi-Ethnic Study of Atherosclerosis)
Connections
- Coronary Calcium Score
- MESA Risk Calculator and Age Percentiles
- CAC Zero and the Power of Negative Result
- CAC vs Other Cardiac Tests
- Statin Threshold and CAC
- Soft Plaque and CAC Limitations
- Insurance Cost and Access
- CAC in Women and Younger Adults
- Reversal Plaque Stabilization and Lifestyle
- Lipoprotein(a)
- ApoB
- Lipid Panel
- Calcium
- Atherosclerosis
- Cardiovascular Disease
- Full Body MRI