Ferritin Test: Iron Storage Protein and Reference Ranges
Ferritin is the body's primary iron storage protein, found in virtually every cell but most concentrated in the liver, spleen, and bone marrow. A serum ferritin blood test measures the amount of ferritin circulating in the bloodstream, which directly reflects total body iron stores — making it the single most sensitive and specific marker for assessing iron status. Because ferritin falls long before hemoglobin declines, it can detect iron deficiency weeks or months before classic anemia develops. At the other extreme, markedly elevated ferritin points toward iron overload, chronic inflammation, liver disease, or malignancy. Understanding your ferritin level in context is one of the most actionable pieces of information a routine blood panel can provide.
Interactive Visualization Iron Absorption & the Hepcidin Gate Watch vitamin C unlock plant iron and hepcidin slam the gate shut — then see why inflammation makes ferritin lie. Launch →Table of Contents
- Overview
- When Ordered
- Reference Ranges
- Iron Deficiency Anemia
- Ferritin as Acute-Phase Reactant
- Hemochromatosis Screening
- Chronic Disease Elevation
- Interpreting Results in Context
- References
- Featured Videos
Overview
Ferritin is a large, hollow protein shell — technically a nanocage — composed of 24 subunits that assemble around an iron core. Each ferritin molecule can store up to 4,500 iron atoms in a safe, non-reactive form, releasing them on demand for hemoglobin synthesis, enzyme production, and cellular energy generation. The liver is the dominant storage site; hepatocytes release a small fraction of their ferritin into circulation, and this serum ferritin level correlates closely with the total iron stored throughout the body.
The critical clinical insight is the sequential depletion model of iron status. Iron deficiency progresses through three stages: in Stage 1, iron stores are depleted and ferritin falls, but blood hemoglobin and red cell indices remain normal. In Stage 2 (iron-restricted erythropoiesis), the bone marrow begins producing iron-deficient red cells — MCV and MCH start to fall — but hemoglobin stays near normal. Only in Stage 3 does frank iron-deficiency anemia appear, with low hemoglobin, small pale red cells, and classic fatigue. Ferritin is the only routine test that identifies Stages 1 and 2 before anemia sets in.
Conversely, very high ferritin is not simply "too much iron." Because ferritin is also an acute-phase reactant synthesized in greater quantities during inflammation, infection, and liver disease, a high ferritin result must be interpreted with additional context. The distinction between true iron overload and inflammatory hyperferritinemia changes the clinical approach entirely.
When Ordered
A ferritin test is appropriate in a wide range of clinical situations. Clinicians typically order it when:
- Fatigue and weakness: Iron-deficient tissues produce less ATP. Fatigue, exercise intolerance, and difficulty concentrating are common even before anemia develops — ferritin identifies depletion at this pre-anemia stage.
- Suspected iron-deficiency anemia: Ferritin paired with a complete blood count (CBC) confirms the diagnosis and quantifies severity of depletion.
- Heavy menstrual periods (menorrhagia): Monthly blood loss is the leading cause of iron deficiency in premenopausal women; ferritin should be checked routinely in this population.
- Vegetarian or vegan diet: Plant-based (non-heme) iron is absorbed at a fraction of the rate of heme iron from animal sources. Regular monitoring prevents silent depletion.
- Pregnancy: Iron demands roughly double in the second and third trimester. Low ferritin during pregnancy is associated with preterm birth and low birth weight.
- Suspected hemochromatosis: Hereditary hemochromatosis causes progressive iron overload. Elevated ferritin plus elevated transferrin saturation is the screening flag that triggers genetic testing.
- Chronic disease monitoring: Inflammatory conditions (IBD, rheumatoid arthritis, CKD) distort ferritin levels; serial testing tracks changes in iron status despite chronic inflammation.
- Restless legs syndrome (RLS): Low brain iron — reflected by low serum ferritin — is a recognized contributing factor in RLS. Guidelines recommend checking ferritin in all RLS patients; levels below 50–75 ng/mL warrant iron supplementation.
- Hair loss: Hair follicles are among the first tissues to lose iron when stores are low. Ferritin below 30–50 ng/mL is frequently identified in women with telogen effluvium.
- Pre-operative assessment: Anemia and iron deficiency before surgery increase transfusion risk and prolong recovery. Pre-operative iron optimization can be guided by ferritin.
- ADHD and cognitive evaluation: Emerging evidence links low ferritin — even in the absence of anemia — to attention difficulties, impulsivity, and poor working memory in children and adults.
The test itself requires a simple venous blood draw and is usually included in iron-studies panels alongside serum iron and transferrin (TIBC). No fasting is required, although some labs recommend avoiding iron supplements for 24 hours before testing.
Reference Ranges
Ferritin — Men (ng/mL)
Ferritin — Women (Premenopausal) (ng/mL)
Ferritin — Women (Postmenopausal) (ng/mL)
Ferritin — Children (ng/mL)
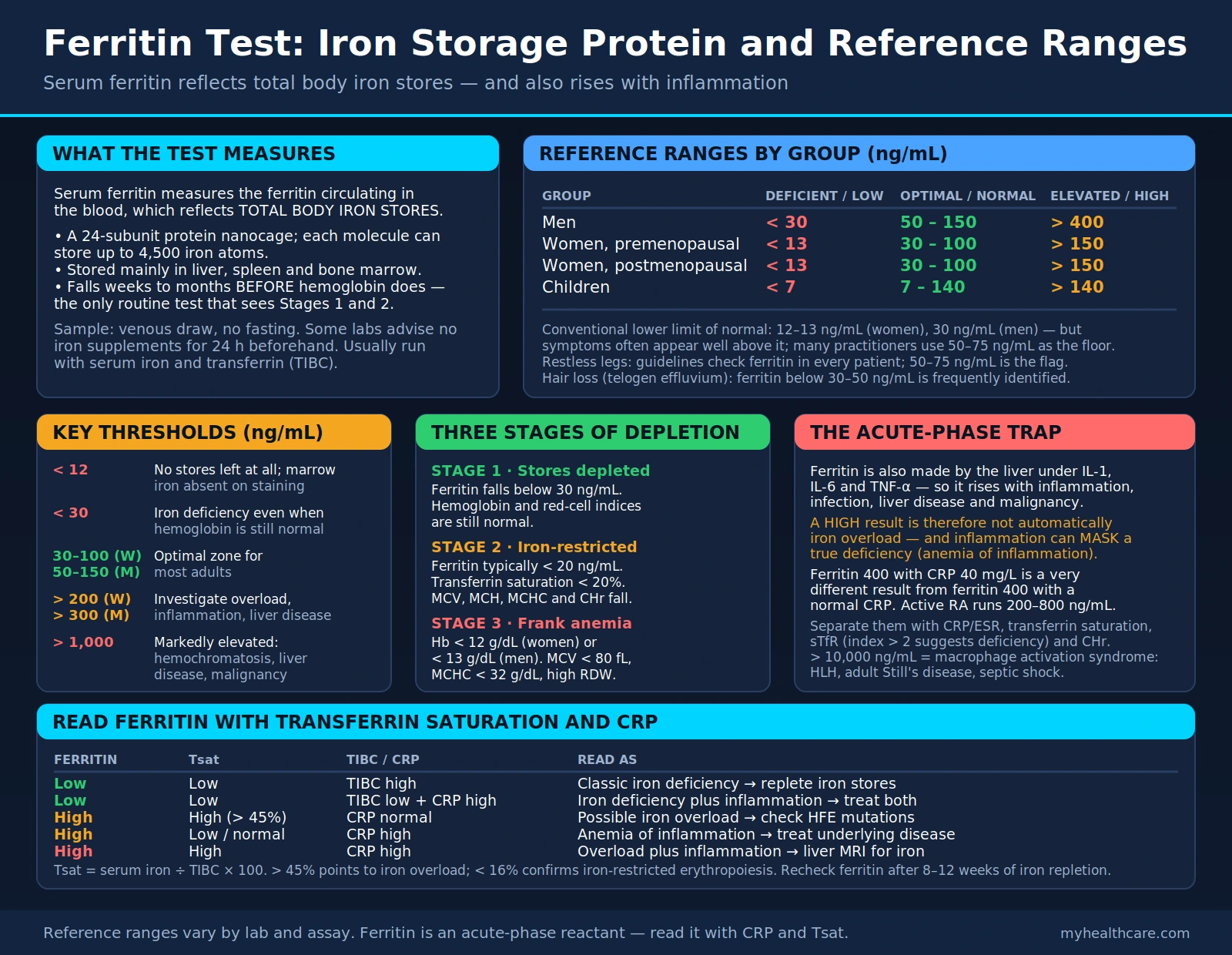
Reference ranges vary between laboratories and assay methods. The conventional lower limit of normal is set at 12–13 ng/mL for women and 30 ng/mL for men, but clinical iron deficiency symptoms frequently appear at ferritin levels well above these cutoffs. Many functional and integrative medicine practitioners use 50–75 ng/mL as the practical floor, particularly when evaluating fatigue, hair loss, or restless legs syndrome.
Key thresholds to know:
- < 12 ng/mL: Iron depletion — essentially no iron stores remain. Bone marrow iron is absent on staining.
- < 30 ng/mL: Iron deficiency, even if hemoglobin is still normal. Treat with iron supplementation.
- 30–100 ng/mL (women) / 50–150 ng/mL (men): Optimal zone for most adults.
- > 200 ng/mL (women) / > 300 ng/mL (men): Warrants investigation for iron overload, inflammation, or liver disease; pair with transferrin saturation and liver function tests.
- > 1,000 ng/mL: Markedly elevated — often seen in hemochromatosis, liver disease, or malignancy; less common in straightforward inflammation.
Iron Deficiency Anemia
Iron deficiency anemia is the world's most common nutritional deficiency, affecting an estimated 1.2 billion people globally. It is the endpoint of a progressive depletion process that ferritin testing can detect — and interrupt — long before anemia develops.
The three stages of iron deficiency:
- Stage 1 — Iron Store Depletion: Ferritin falls below 30 ng/mL. Serum iron may still be normal. Hemoglobin and red cell indices are normal. Symptoms can include fatigue, reduced exercise capacity, poor concentration, cold intolerance, and hair shedding — all caused by iron-dependent enzyme deficiencies in non-hematopoietic tissues. This stage is invisible to a CBC alone.
- Stage 2 — Iron-Restricted Erythropoiesis: The bone marrow no longer has enough iron to make fully hemoglobinized red cells. Red cell indices begin to fall (MCV, MCH, MCHC decline). Transferrin saturation drops below 20%. Reticulocyte hemoglobin content (CHr) falls — a sensitive early marker. Ferritin is typically < 20 ng/mL. Symptoms worsen.
- Stage 3 — Frank Iron-Deficiency Anemia: Hemoglobin falls below 12 g/dL (women) or 13 g/dL (men). Red cells are small (microcytic, MCV < 80 fL) and pale (hypochromic, MCHC < 32 g/dL). Classic symptoms: pallor, palpitations, dyspnea on exertion, tinnitus, glossitis, angular cheilitis, and in severe cases koilonychia (spoon nails) or pica (craving for ice or dirt).
Common causes of iron deficiency:
- Blood loss: Heavy menstrual periods, GI bleeding (peptic ulcer, colorectal cancer, angiodysplasia), frequent blood donation, or surgical blood loss.
- Poor absorption: Celiac disease, Helicobacter pylori infection, atrophic gastritis, post-bariatric surgery, and long-term proton pump inhibitor (PPI) use all reduce gastric acid and impair non-heme iron absorption.
- Increased demand: Pregnancy, rapid growth in adolescence, and endurance athletics (especially running, which causes foot-strike hemolysis and GI microbleeding).
- Inadequate dietary intake: Restrictive vegetarian or vegan diets without adequate non-heme iron sources or vitamin C co-ingestion to enhance absorption.
Treatment is guided by severity. Stage 1–2 responds well to oral ferrous sulfate, ferrous bisglycinate (better tolerated), or dietary optimization. Stage 3 with symptomatic anemia may require higher-dose oral iron; Stage 3 with malabsorption, intolerance, or urgent need (pre-surgery, severe anemia) typically requires intravenous iron infusion.
Ferritin as Acute-Phase Reactant
One of the most clinically important — and frequently misunderstood — properties of ferritin is that it is not simply a passive storage protein. Ferritin is actively synthesized by the liver in response to inflammatory signals, specifically interleukin-1 (IL-1), interleukin-6 (IL-6), and tumor necrosis factor-alpha (TNF-α). This makes ferritin an acute-phase reactant — a protein whose serum level rises during systemic inflammation, infection, and tissue injury, independent of actual iron stores.
The practical consequence is critical: a high ferritin result does not automatically mean iron overload. In a patient with active rheumatoid arthritis, lupus flare, severe infection, liver disease, or malignancy, ferritin may be elevated into the hundreds or even thousands of ng/mL while iron stores are actually normal or even low. This situation — functional iron deficiency masked by an inflammatory ferritin elevation — is called anemia of chronic disease (now often termed anemia of inflammation).
How to distinguish true iron overload from inflammatory hyperferritinemia:
- C-reactive protein (CRP) and ESR: If ferritin is high and CRP is also elevated, inflammation is the likely driver of the ferritin rise, not iron overload. A ferritin of 400 ng/mL with a CRP of 40 mg/L is very different from a ferritin of 400 ng/mL with a normal CRP.
- Transferrin saturation: In true iron overload (hemochromatosis, transfusional iron overload), both ferritin and transferrin saturation are high (>45%). In anemia of inflammation, ferritin is high but transferrin saturation is often low (<20%), because inflammatory cytokines also suppress iron release from stores (via hepcidin upregulation).
- Soluble transferrin receptor (sTfR): sTfR rises when cells are starved for iron (true deficiency) but does NOT rise in pure inflammation. The sTfR-to-log-ferritin ratio (sTfR index) can distinguish iron-deficiency anemia from anemia of inflammation — useful when both conditions coexist.
- Reticulocyte hemoglobin content (CHr/Ret-He): Falls in iron-restricted erythropoiesis regardless of ferritin level, providing real-time information about how much iron is actually reaching the bone marrow.
Extreme hyperferritinemia (> 10,000 ng/mL) is sometimes called "macrophage activation syndrome" and is seen in severe conditions: adult-onset Still's disease, hemophagocytic lymphohistiocytosis (HLH), septic shock, and massive hepatic necrosis. In these contexts, ferritin itself may be directly toxic to endothelium and immune cells, and is used as a diagnostic and prognostic marker.
Hemochromatosis Screening
Hereditary hemochromatosis (HH) is one of the most common autosomal recessive genetic disorders in populations of Northern European ancestry, affecting approximately 1 in 200–300 individuals of that background. It is caused primarily by mutations in the HFE gene — most commonly the C282Y substitution (rs1800562), with H63D (rs1799945) as a secondary variant. These mutations impair the hepcidin-mediated regulation of iron absorption, causing the intestine to absorb far more iron than the body requires, leading to progressive iron accumulation in the liver, heart, pancreas, joints, and pituitary gland over decades.
The screening strategy uses ferritin and transferrin saturation together:
- Elevated transferrin saturation (> 45%): The earliest biochemical abnormality in HH, appearing before ferritin rises significantly. Calculated as (serum iron / TIBC) × 100.
- Elevated ferritin (> 300 ng/mL in men, > 200 ng/mL in women) plus elevated transferrin saturation: Triggers genetic testing for HFE C282Y/H63D mutations.
- C282Y homozygosity: Confirms hereditary hemochromatosis. Liver biopsy or MRI liver iron quantification is used to assess degree of iron loading and fibrosis.
Untreated hemochromatosis causes:
- Liver cirrhosis and hepatocellular carcinoma (the most serious consequences)
- Bronze diabetes (pancreatic iron deposition causing insulin resistance and diabetes)
- Cardiomyopathy and arrhythmias
- Hypogonadism and infertility (pituitary iron deposition)
- Arthritis, particularly of the 2nd and 3rd metacarpophalangeal joints (a distinctive pattern)
- Fatigue and lethargy (often the first symptom)
Treatment is remarkably simple and effective when diagnosed early: therapeutic phlebotomy (regular blood donation) removes iron-laden red cells and prevents further organ damage. Weekly phlebotomy continues until ferritin falls to 50–100 ng/mL, followed by maintenance phlebotomy every 2–4 months indefinitely. When phlebotomy is not tolerated (severe anemia, heart failure), iron chelation with deferasirox or deferoxamine is an alternative.
Secondary (acquired) hemochromatosis can result from transfusional iron overload in patients with thalassemia, sickle cell disease, or myelodysplastic syndrome receiving chronic red cell transfusions. It can also result from alcoholic liver disease, which impairs hepcidin production, and from chronic hepatitis C.
Chronic Disease Elevation
Beyond hereditary hemochromatosis, many common chronic conditions cause ferritin elevation that must be recognized and distinguished from iron overload. Elevated ferritin in these settings reflects inflammation, hepatocyte injury, or both — not necessarily excess iron stores.
Inflammatory and autoimmune conditions:
- Rheumatoid arthritis: Ferritin commonly runs 200–800 ng/mL during active disease due to IL-6-driven acute-phase synthesis. Monitoring ferritin trends alongside CRP helps track disease activity.
- Systemic lupus erythematosus (SLE): Ferritin elevation proportional to disease flare activity; extreme hyperferritinemia can signal macrophage activation syndrome, a serious complication.
- Inflammatory bowel disease (IBD): Both Crohn's disease and ulcerative colitis elevate ferritin via inflammation while simultaneously causing iron deficiency through GI blood loss and poor absorption — a challenging dual problem.
Liver disease:
- Non-alcoholic fatty liver disease (NAFLD) and NASH: Hepatocyte injury releases intracellular ferritin; ferritin correlates with severity of steatohepatitis and fibrosis. Ferritin > 1.5 × ULN is a component of some NASH risk scores.
- Alcoholic liver disease: Alcohol both damages hepatocytes (releasing ferritin) and increases GI iron absorption, often producing combined true iron overload and inflammatory elevation.
- Viral hepatitis (B and C): Active hepatic inflammation elevates ferritin. Sustained virological response to hepatitis C treatment often causes ferritin to fall.
- Cirrhosis: Markedly elevated ferritin from combined hepatocyte destruction and impaired ferritin clearance.
Metabolic conditions:
- Type 2 diabetes and insulin resistance: Hyperinsulinemia stimulates ferritin synthesis; ferritin elevation precedes the development of frank diabetes in prospective studies, suggesting it as a risk marker.
- Obesity: Adipose tissue is an inflammatory organ; elevated adipokines and inflammatory cytokines drive ferritin elevation in proportion to BMI and visceral fat.
Malignancy:
- Lymphoma (especially Hodgkin's): Ferritin is frequently markedly elevated and tracks disease burden; very high ferritin at diagnosis is an adverse prognostic factor.
- Hepatocellular carcinoma (HCC): Ferritin can serve as a tumor-associated marker in HCC alongside AFP (alpha-fetoprotein).
- Other malignancies: Breast, lung, and colorectal cancers can cause paraneoplastic ferritin elevation, thought to reflect both tumor-cell ferritin production and systemic inflammatory response.
Rare conditions: Hyperferritinemia-cataract syndrome is a rare autosomal dominant disorder caused by mutations in the iron-responsive element of the ferritin light-chain gene. Affected individuals have persistently elevated serum ferritin (500–2,000 ng/mL) without iron overload, but develop bilateral cataracts from ferritin crystallization in the ocular lens. This condition illustrates that high ferritin alone is not synonymous with high iron stores.
Interpreting Results in Context
Ferritin is best understood not as a standalone test but as one data point within a coordinated panel of iron and inflammatory markers. The following companion tests, ordered alongside ferritin, maximize diagnostic clarity:
- Serum iron: The amount of iron currently circulating bound to transferrin. Low in true iron deficiency and anemia of inflammation; high in iron overload.
- Total iron-binding capacity (TIBC) / transferrin: Reflects the number of available iron-binding sites on transferrin. TIBC rises when the body is iron-hungry (true deficiency); TIBC falls in inflammation, liver disease, and iron overload.
- Transferrin saturation (Tsat): Serum iron ÷ TIBC × 100. The single most useful companion to ferritin. Low Tsat (< 16%) confirms iron-restricted erythropoiesis. High Tsat (> 45%) with high ferritin points to iron overload.
- CBC with differential: Hemoglobin, hematocrit, MCV, MCH, MCHC, and RDW together characterize the red cell population. Microcytic, hypochromic anemia with high RDW is the classic CBC pattern of iron deficiency anemia.
- Reticulocyte count and reticulocyte hemoglobin content (CHr): Assess how effectively the bone marrow is currently producing iron-replete red cells. CHr below 28–29 pg indicates functional iron deficiency at the marrow level.
- CRP and ESR: Quantify the degree of systemic inflammation. Elevated inflammatory markers with elevated ferritin suggests the ferritin rise is predominantly inflammatory rather than reflecting true iron overload.
- Soluble transferrin receptor (sTfR): Rises in true iron deficiency even when ferritin is artificially elevated by inflammation. The sTfR index (sTfR / log ferritin) > 2 suggests iron deficiency in the presence of inflammation. Available at specialized laboratories.
- Liver function tests (ALT, AST, GGT): Hepatocellular damage elevates ferritin via cell lysis. Transaminase elevation alongside hyperferritinemia points toward liver disease as the source.
A useful decision framework:
- Low ferritin + low Tsat + high TIBC = classic iron deficiency → replete iron stores
- Low ferritin + low Tsat + low TIBC + elevated CRP = iron deficiency plus inflammation → treat both
- High ferritin + high Tsat + normal CRP = possible iron overload → check HFE mutations
- High ferritin + low/normal Tsat + elevated CRP = anemia of inflammation → treat underlying disease
- High ferritin + high Tsat + elevated CRP = complex picture (overload plus inflammation) → liver MRI for iron quantification
Repeat ferritin testing after 8–12 weeks on iron supplementation confirms repletion. In treated hemochromatosis, ferritin is monitored at each phlebotomy session as the primary target endpoint. In chronic inflammatory disease, serial ferritin trends alongside CRP help disentangle iron status from disease activity over time.
References
The following are curated PubMed literature searches covering the evidence base for ferritin testing, interpretation, and clinical management. Each link opens a live, filtered PubMed query so the results stay current as new studies are indexed.
- Serum ferritin iron deficiency anemia diagnosis — PubMed literature search
- Ferritin as acute-phase reactant in inflammation — PubMed literature search
- Hereditary hemochromatosis ferritin screening — PubMed literature search
- Ferritin reference range and iron stores — PubMed literature search
- Iron deficiency without anemia and fatigue — PubMed literature search
- Ferritin elevation in liver disease — PubMed literature search
- Ferritin as malignancy tumor marker — PubMed literature search
- Transferrin saturation hemochromatosis HFE gene — PubMed literature search
- Ferritin in chronic kidney disease and inflammation — PubMed literature search
- Restless legs syndrome iron and ferritin — PubMed literature search
- Iron deficiency hair loss and ferritin levels — PubMed literature search
- Ferritin in pregnancy and iron supplementation — PubMed literature search
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Clinical Laboratory Reference
Connections
- All Lab Tests
- Iron Absorption & the Hepcidin Gate — interactive animation
- Anemia
- Hemochromatosis
- Complete Blood Count
- Inflammatory Markers
- Iron
- Iron Deficiency
- Vitamin C
- Celiac Disease
- NAFLD
- Crohn's Disease
- Rheumatoid Arthritis
- Chronic Kidney Disease
- Restless Legs Syndrome
- Homocysteine Test
- Lipid Panel
- Type 2 Diabetes
- Lymphoma
- Beef