Turmeric for Brain Health and Cognition
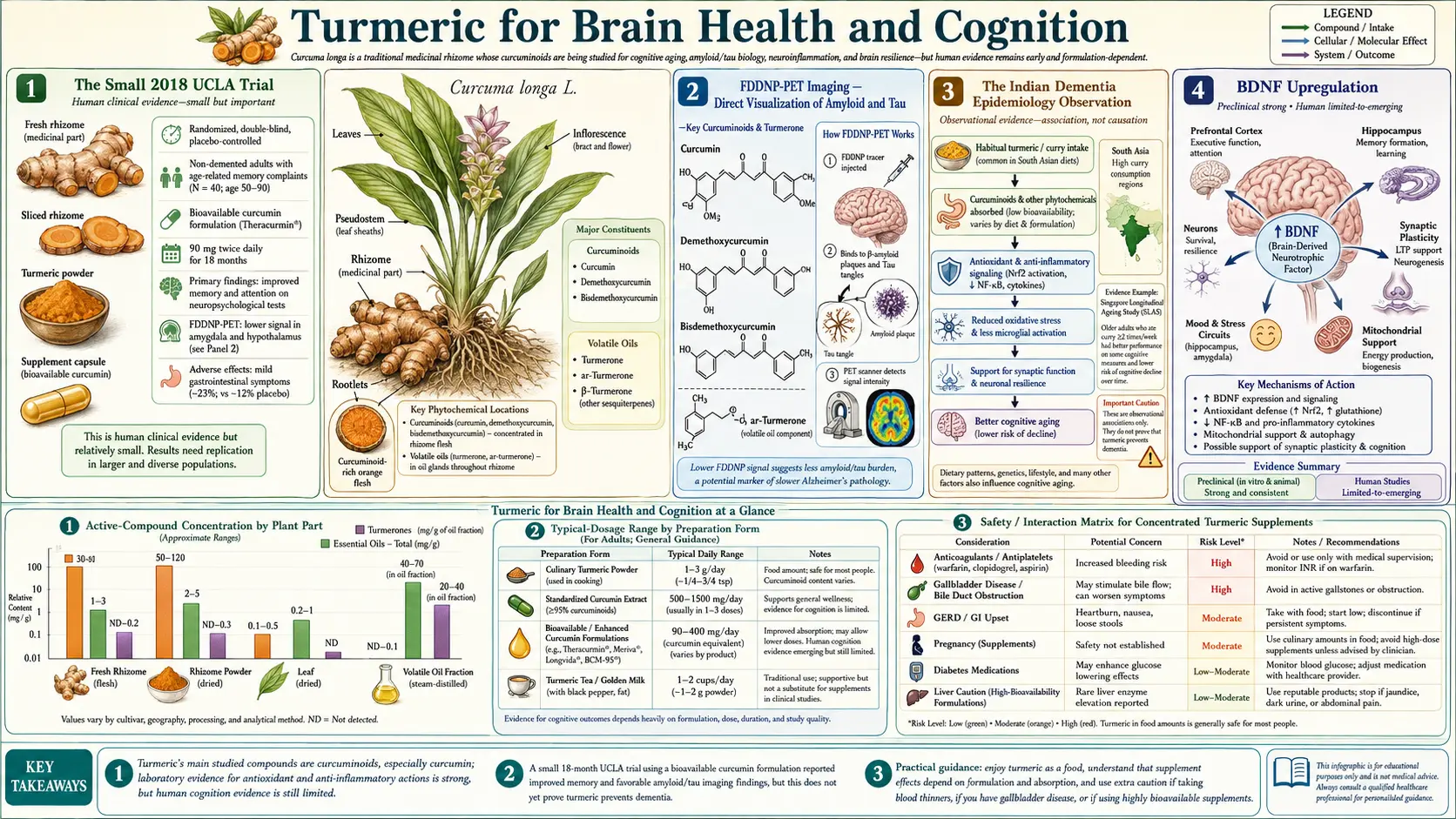
The most compelling human cognitive trial of curcumin is the Small GW et al. 2018 UCLA study published in the American Journal of Geriatric Psychiatry. Forty older adults with mild subjective memory complaints were randomized to Theracurmin 90 mg twice daily or placebo for 18 months, with serial neuropsychological testing and FDDNP-PET brain imaging. The curcumin group showed significant improvements in both verbal memory (SVLT) and visual memory (BVMT) testing, plus statistically significant reductions in amyloid-beta and tau accumulation in the amygdala and hypothalamus on PET imaging — physical evidence that the cognitive effect corresponds to a measurable change in Alzheimer's-pathology biomarkers. This sits on top of a long-standing epidemiologic observation: India has among the lowest dementia prevalence rates in the world, and turmeric-rich diet is one of several hypothesized contributors. Mechanistically, curcumin upregulates BDNF (brain-derived neurotrophic factor), suppresses microglial neuroinflammation, disaggregates amyloid-beta fibrils in vitro, and — uniquely among most polyphenols — crosses the blood-brain barrier in measurable quantities, especially in the lipid-formulation versions like Longvida SLCP.
Table of Contents
- The Small 2018 UCLA Trial
- FDDNP-PET Imaging — Direct Visualization of Amyloid and Tau
- The Indian Dementia Epidemiology Observation
- BDNF Upregulation
- Neuroinflammation and Microglial Activation
- Amyloid-Beta Binding and Disaggregation
- Blood-Brain Barrier Crossing
- Depression and Mood
- Vascular Cognitive Impairment and Stroke
- Parkinson's and Other Neurodegenerative Conditions
- Dosing for Cognitive Applications
- Key Research Papers
- Connections
- Featured Videos
The Small 2018 UCLA Trial
Gary Small and colleagues at the UCLA Longevity Center designed the Small 2018 trial to address a specific gap in the curcumin cognitive literature: most prior trials had been short (8–12 weeks) and used cognitive endpoints alone. Small added two critical elements — long duration (18 months) and direct brain imaging of Alzheimer's pathology (FDDNP-PET) — that turned a typical supplement trial into a more rigorous test of disease modification.
Study design:
- Participants: 40 non-demented adults aged 50–90 (mean age 64), with mild memory complaints but no diagnosis of dementia or MCI
- Intervention: Theracurmin (Theravalues colloidal submicron-particle curcumin) 90 mg twice daily, totaling 180 mg/day. Theracurmin was chosen specifically for its documented high bioavailability and free-curcumin pharmacokinetics.
- Comparator: Matched placebo
- Duration: 18 months — long enough to detect modification of the slowly-progressive Alzheimer's neuropathology
- Primary endpoints: SVLT (Buschke Selective Reminding Test) for verbal memory; BVMT-R (Brief Visuospatial Memory Test-Revised) for visual memory; FDDNP-PET for amyloid and tau brain accumulation
Results at 18 months:
- SVLT Long-Term Retrieval and Long-Term Storage scores improved significantly in the curcumin group compared to placebo, with effect sizes corresponding to ~28% improvement in verbal memory
- BVMT-R visual memory scores also improved significantly in the curcumin group
- Attention scores improved on Trails A testing
- FDDNP-PET binding decreased significantly in amygdala and hypothalamus in the curcumin group — physical evidence of reduced amyloid and tau accumulation in regions involved in memory and stress regulation
- Mood improved on the Beck Depression Inventory in the curcumin group
- No serious adverse events attributable to curcumin
The trial was small and a single-center study, and FDDNP is no longer the dominant amyloid-PET tracer (florbetapir, florbetaben, and flutemetamol have replaced it for clinical Alzheimer's imaging). But the combination of memory improvement and corresponding PET-imaging signal — in a population without dementia, over 18 months, with a bioavailability-enhanced curcumin formulation — is the most rigorous demonstration to date that curcumin can modify the trajectory of age-related cognitive decline and may engage genuine Alzheimer's pathology mechanisms.
FDDNP-PET Imaging — Direct Visualization of Amyloid and Tau
FDDNP (2-(1-{6-[(2-[18F]fluoroethyl)(methyl)amino]-2-naphthyl}ethylidene)malononitrile) is a small-molecule radiotracer developed at UCLA in the early 2000s that binds both amyloid-beta plaques and tau neurofibrillary tangles in vivo. It was the first PET tracer to visualize Alzheimer's-disease pathology in living humans, predating the later amyloid-specific tracers florbetapir and Pittsburgh Compound B.
FDDNP has both an advantage and a limitation versus the modern amyloid-specific tracers. The advantage is that it picks up both amyloid and tau, the two hallmark Alzheimer's lesions; the limitation is that it cannot distinguish them. In the Small 2018 trial, the FDDNP signal reduction in amygdala and hypothalamus could reflect amyloid reduction, tau reduction, or both — the imaging modality cannot tell.
What the imaging does establish is that the cognitive effect of curcumin in the trial corresponds to a measurable change in something biological happening in the brain. This is unusual for supplement trials, which typically report cognitive endpoints alone without biomarker confirmation. The Small trial therefore stands as one of the more rigorous pieces of evidence that any dietary intervention — not just curcumin — can produce detectable changes in Alzheimer's-relevant brain biomarkers in non-demented older adults.
Subsequent imaging research has continued to investigate curcumin's amyloid-binding properties in vivo. Curcumin itself has been investigated as a potential amyloid-PET tracer because of its high binding affinity to beta-sheet amyloid structures, though its physical chemistry has not made it suitable for clinical PET use compared to the established F-18 labeled tracers.
The Indian Dementia Epidemiology Observation
The cross-cultural epidemiology of Alzheimer's disease and other dementias has long included a puzzling observation: age-adjusted dementia prevalence in rural India is among the lowest in the world, perhaps one-quarter to one-third of age-adjusted rates in North America or Western Europe. The Ballabgarh study in northern India (Chandra V et al. 2001) found Alzheimer's prevalence of 0.62% in adults over 55, compared to roughly 2% in age-matched US populations. Several other Indian rural cohort studies have reported similar findings.
The Indian dementia low-prevalence observation is part of the original motivation for the modern curcumin neurology research program. The hypothesis advanced by Frautschy, Cole, and others at UCLA in the early 2000s was that the high turmeric content of traditional Indian cuisine (curry powders, sambar, dal preparations) contributed to the reduced dementia rate. Turmeric is not the only candidate explanation — differences in education, life expectancy, dementia diagnostic capture, cardiovascular risk burden, social and family support structures, and other diet-pattern factors all confound the comparison — but the curcumin hypothesis is biologically plausible and has now been substantially developed through both animal and human studies.
The transgenic mouse models of Alzheimer's disease developed by the Cole lab at UCLA (TgCRND8, APP/PS1, and others) showed that low-dose dietary curcumin reduced amyloid plaque burden by 40–50% in the cortex and hippocampus of older mice. The mechanism in the mouse models proved to involve all of the pathways discussed below: BDNF upregulation, microglial polarization to the anti-inflammatory M2 phenotype, direct amyloid-beta binding and disaggregation, and reduced tau hyperphosphorylation.
An important practical caveat: the dietary turmeric exposure of Indian populations comes primarily from food-based curcumin, not bioavailability-enhanced supplements, and at modest daily milligram quantities. The protection (if real) develops over decades of cumulative exposure starting in childhood, not over months of supplement use in adulthood. The animal-model and human-trial doses required to demonstrate measurable effects on dementia biomarkers in adults are substantially higher than what is achievable through diet alone.
BDNF Upregulation
Brain-derived neurotrophic factor (BDNF) is a 14-kDa protein in the neurotrophin family that supports the survival, growth, and synaptic plasticity of neurons throughout the central and peripheral nervous system. BDNF signals through the tropomyosin receptor kinase B (TrkB) receptor, activating the PI3K/Akt and MAPK pathways that promote dendritic arborization, long-term potentiation (the cellular basis of learning), and adult neurogenesis in the hippocampal dentate gyrus.
BDNF levels decline with age and are reduced in major depressive disorder, schizophrenia, Alzheimer's disease, and several other neurological and psychiatric conditions. Restoration of BDNF signaling is one of the principal hypothesized mechanisms of action of SSRI antidepressants, exercise, intermittent fasting, and ketogenic diet on mood and cognition. Animal studies consistently show that curcumin increases hippocampal and cortical BDNF mRNA and protein expression, with effect sizes comparable to those seen with antidepressant treatment.
The Sanmukhani 2014 randomized controlled trial in Phytotherapy Research compared curcumin 1000 mg/day vs fluoxetine 20 mg/day in 60 patients with major depressive disorder over 6 weeks. The curcumin group showed comparable Hamilton Depression Rating Scale improvement to the fluoxetine group, and the combination produced the largest effect. While the trial did not measure BDNF directly in humans, the parallel between curcumin and SSRI efficacy is consistent with the BDNF-mediated mechanism.
For the broader picture on BDNF in cognitive and mood applications, see our Brain Aging page.
Neuroinflammation and Microglial Activation
Microglia are the resident macrophages of the central nervous system, surveillant cells that detect tissue injury, misfolded protein aggregates, and infection. Activated microglia secrete cytokines (TNF-alpha, IL-1beta, IL-6), reactive oxygen species, and complement proteins, and they phagocytose dying neurons and protein aggregates. In acute settings this is protective; in chronic settings of slowly-accumulating amyloid plaques or tau tangles, persistent microglial activation produces a low-grade neuroinflammatory state that damages neighboring neurons and accelerates neurodegeneration.
The Alzheimer's field has increasingly recognized microglial dysregulation as a central pathogenic mechanism. Genetic risk loci identified by genome-wide association studies (TREM2, CR1, CD33, ABCA7) cluster around microglial function. The amyloid cascade hypothesis has been refined to include the role of microglial response to amyloid as a major determinant of whether amyloid accumulation translates to clinical dementia.
Curcumin's effects on microglia have been studied extensively in vitro and in animal models. It promotes the polarization of microglia from the pro-inflammatory M1 phenotype (TNF-alpha, IL-1beta, iNOS, MHC-II) toward the anti-inflammatory and tissue-repair M2 phenotype (IL-10, TGF-beta, arginase, IGF-1). Curcumin also inhibits NLRP3 inflammasome activation in microglia, reducing IL-1beta and IL-18 production. The net effect is reduced chronic neuroinflammation around amyloid plaques and reduced bystander injury to neighboring neurons.
The neuroinflammation effect overlaps mechanistically with the joint-inflammation effect — the same NF-kB inhibition that calms synovial macrophages also calms microglia. This is why a single curcumin intervention can plausibly produce effects on arthritis, NAFLD, and dementia risk simultaneously.
Amyloid-Beta Binding and Disaggregation
Beyond its anti-inflammatory effects, curcumin has direct biophysical effects on amyloid-beta peptide aggregation. The curcumin molecule has a conjugated planar structure that binds preferentially to the beta-sheet fibrillar form of amyloid-beta, the structure that accumulates in senile plaques. In vitro, curcumin both inhibits the polymerization of amyloid-beta monomers into fibrils and disaggregates pre-formed amyloid fibrils back to smaller species.
The seminal work was by Yang F et al. 2005 in the Journal of Biological Chemistry, demonstrating both effects with purified amyloid-beta peptide. Subsequent work showed that orally-administered curcumin reduces amyloid plaque burden in transgenic Alzheimer's mouse models (TgAPPsw, Tg2576, APP/PS1) by 30–50% over months of dietary administration. The combination of direct anti-amyloid action and the anti-neuroinflammatory effect distinguishes curcumin from purely symptomatic cognitive interventions.
Whether the same anti-amyloid effect operates in humans at achievable supplement doses is the central uncertainty. The Small 2018 FDDNP-PET data are suggestive but limited to a small sample in two specific brain regions. Larger trials with the modern amyloid-PET tracers (florbetapir, florbetaben) and longer follow-up will be needed to firmly establish whether human chronic curcumin supplementation reduces brain amyloid burden over years to decades.
Blood-Brain Barrier Crossing
The blood-brain barrier (BBB) is a major obstacle to any therapy aimed at the central nervous system. Tight junctions between brain capillary endothelial cells, the basal lamina, astrocytic end-feet, and efflux transporters (P-glycoprotein, BCRP) limit which molecules can enter the brain parenchyma. Most polyphenols, including most flavonoids and most resveratrol metabolites, have minimal BBB penetration — the molecules either fail to enter the brain or are actively pumped back out by efflux transporters.
Curcumin is one of the few dietary polyphenols with documented measurable BBB penetration. Its modest molecular weight (368 Da), high lipophilicity (logP around 3.3), and lack of strong P-glycoprotein substrate behavior allow it to cross into brain tissue. The Begum AN et al. 2008 paper measured curcumin in mouse brain tissue after oral dosing, confirming BBB penetration — albeit at very low concentrations compared to plasma.
The brain-penetration question is particularly important for choice of curcumin formulation. The Longvida SLCP (solid lipid curcumin particle) formulation was specifically engineered for free unconjugated curcumin in plasma rather than the glucuronide-conjugated form — because free curcumin has substantially better BBB penetration than glucuronide-curcumin. This is the rationale for Longvida being the most-favored formulation in cognitive research, despite Meriva and Theracurmin having stronger trial data in joint and liver applications.
For the detailed comparison of curcumin formulations, see the Bioavailability and Forms page.
Depression and Mood
Major depressive disorder shares several pathogenic features with cognitive aging: reduced BDNF, increased neuroinflammation, microglial dysregulation, and HPA axis dysregulation. The same curcumin mechanisms that support cognitive function therefore also have antidepressant effects.
Clinical evidence:
- Sanmukhani 2014 — randomized 60 MDD patients to curcumin 1000 mg/day vs fluoxetine 20 mg/day vs combination for 6 weeks. Curcumin equivalent to fluoxetine on HAM-D; combination produced largest response.
- Lopresti 2014 — randomized 56 MDD patients to BCM-95 curcumin 1000 mg/day vs placebo for 8 weeks. Curcumin produced significantly greater improvement in IDS-SR30 (Inventory of Depressive Symptomatology) and STAI (anxiety) than placebo. A subsequent 2015 paper from the same group extended to 12 weeks with sustained effect.
- Yu 2015 — randomized 108 elderly patients with depression to curcumin 1000 mg/day or placebo as adjunct to existing antidepressant for 6 weeks. Curcumin group had significantly better HAM-D improvement.
- Ng 2017 meta-analysis — pooled six trials with 377 patients; curcumin showed significant antidepressant effect, with effect size comparable to standard antidepressants in mild-to-moderate depression.
Curcumin is not a substitute for evidence-based antidepressant therapy in moderate-to-severe major depression, but the data support it as a reasonable adjunct to SSRI/SNRI therapy or as monotherapy in mild depression and seasonal mood symptoms. The favorable side-effect profile compared to SSRIs (no sexual dysfunction, no GI distress, no weight gain, no discontinuation syndrome) makes it attractive for patients who tolerate antidepressants poorly.
Vascular Cognitive Impairment and Stroke
A substantial fraction of dementia in aging populations is vascular rather than Alzheimer's — small-vessel ischemic disease, lacunar infarcts, and the cumulative impact of chronic hypertension and atherosclerosis on cerebral perfusion. The Akazawa N et al. 2012 trial in Nutrition Research studied curcumin's effect on endothelial function in postmenopausal women, showing significant improvement in flow-mediated dilation (a measure of vascular endothelial health) after 8 weeks of curcumin 150 mg/day.
The mechanism for cerebrovascular benefit overlaps with curcumin's general cardiovascular effects: improved endothelial function via increased nitric oxide bioavailability, reduced oxidized LDL, anti-inflammatory effects on the vascular endothelium, and modest reductions in blood pressure and lipids. The cumulative effect of these is reduced small-vessel ischemic burden in the brain, which translates to reduced vascular cognitive impairment in observational studies.
In acute ischemic stroke, animal models show that curcumin pre-treatment reduces infarct volume and improves neurological outcomes through reduction of post-ischemic neuroinflammation. Human stroke prevention or treatment trials with curcumin are not yet conclusive, but the mechanistic basis is reasonable and the cardiovascular risk-factor improvements documented in metabolic trials translate plausibly to reduced stroke risk.
Parkinson's and Other Neurodegenerative Conditions
Parkinson's disease involves accumulation of misfolded alpha-synuclein protein in Lewy bodies, with selective neurodegeneration of dopaminergic neurons in the substantia nigra. Curcumin has been shown in vitro and in animal models to inhibit alpha-synuclein aggregation (analogous to its anti-amyloid effect) and to protect dopaminergic neurons from MPTP-induced and rotenone-induced injury. Human clinical trials of curcumin in established Parkinson's disease are limited, and curcumin is not currently considered a disease-modifying therapy — but it is plausibly useful as adjunct neuroprotection in the broader Parkinson's integrative-medicine approach.
Other neurological applications with mechanistic support but limited human trial data include:
- Multiple sclerosis — animal models of experimental autoimmune encephalomyelitis show curcumin reduces disease severity through Th17/Treg shift, similar to the mechanism discussed in the immune section
- Traumatic brain injury — animal models show curcumin reduces secondary neuroinflammation after TBI
- Chemotherapy-induced cognitive impairment — "chemo brain" — suggestive small studies
- Epilepsy — animal models show anticonvulsant effect through glutamate modulation; not enough human data for clinical recommendation
Dosing for Cognitive Applications
For cognitive support and brain-health applications, the formulations with the best blood-brain barrier penetration are preferred:
- Longvida SLCP 400–1000 mg/day — the highest free-curcumin pharmacokinetics; favored for cognitive applications based on BBB penetration data. Typical starting dose 400 mg/day, titrate to 800–1000 mg/day if well tolerated.
- Theracurmin 90 mg twice daily — matches the Small 2018 UCLA trial. The most direct evidence for cognitive outcomes.
- BCM-95 (curcumin + turmeric essential oil) 500 mg twice daily — matches the Lopresti depression trials.
- Meriva 1000 mg/day — well documented for joint and liver applications; reasonable also for cognitive support though less BBB-penetration data.
Cognitive benefits develop slowly — the Small UCLA trial used 18 months. Allow at least 3–6 months before assessing effect on subjective memory or mood. Combination with other cognitive-support interventions is synergistic: omega-3 fatty acids (DHA) for membrane structural support and SPM precursors; vitamin D for neuroprotective signaling; B12 and folate for homocysteine reduction; regular aerobic exercise for the most-evidence-supported BDNF stimulus.
Key Research Papers
- Small GW et al. (2018). Memory and brain amyloid and tau effects of a bioavailable form of curcumin in non-demented adults: A double-blind, placebo-controlled 18-month trial. American Journal of Geriatric Psychiatry. — PubMed
- Chandra V et al. (2001). Incidence of Alzheimer's disease in a rural community in India: The Indo-US study. Neurology. — PubMed
- Yang F et al. (2005). Curcumin inhibits formation of amyloid beta oligomers and fibrils, binds plaques, and reduces amyloid in vivo. Journal of Biological Chemistry. — PubMed
- Begum AN et al. (2008). Curcumin structure-function, bioavailability, and efficacy in models of neuroinflammation and Alzheimer's disease. Journal of Pharmacology and Experimental Therapeutics. — PubMed
- Lim GP et al. (2001). The curry spice curcumin reduces oxidative damage and amyloid pathology in an Alzheimer transgenic mouse. Journal of Neuroscience. — PubMed
- Sanmukhani J et al. (2014). Efficacy and safety of curcumin in major depressive disorder: A randomized controlled trial. Phytotherapy Research. — PubMed
- Lopresti AL et al. (2014). Curcumin for the treatment of major depression: A randomised, double-blind, placebo controlled study. Journal of Affective Disorders. — PubMed
- Ng QX et al. (2017). Clinical use of curcumin in depression: A meta-analysis. Journal of the American Medical Directors Association. — PubMed
- Cox KH et al. (2015). Investigation of the effects of solid lipid curcumin on cognition and mood in a healthy older population. Journal of Psychopharmacology. — PubMed
- Akazawa N et al. (2012). Curcumin ingestion and exercise training improve vascular endothelial function in postmenopausal women. Nutrition Research. — PubMed
- Voulgaropoulou SD et al. (2019). The effect of curcumin on cognition in Alzheimer's disease and healthy aging: A systematic review of pre-clinical and clinical studies. Brain Research. — PubMed
- Frautschy SA, Cole GM (2010). Why pleiotropic interventions are needed for Alzheimer's disease. Molecular Neurobiology. — PubMed
PubMed Topic Searches
- PubMed: Curcumin cognition trials
- PubMed: Curcumin Alzheimer's
- PubMed: Curcumin depression / BDNF
- PubMed: Curcumin BBB penetration
- PubMed: Curcumin neuroinflammation
- PubMed: Longvida SLCP cognitive
- PubMed: Curcumin Parkinson's / alpha-synuclein
Connections
- Turmeric Benefits Hub
- Turmeric Overview
- Turmeric for Joint Health
- Turmeric for Liver Health
- Bioavailability & Forms
- Bacopa Monnieri
- Lion's Mane Mushroom
- Ashwagandha
- Omega-3 Fatty Acids (DHA)
- Vitamin D3
- Vitamin B12
- Alzheimer's Disease
- Parkinson's Disease
- Depression
- Brain Aging
- Dementia — the broader cognitive-decline syndrome whose low prevalence in India first motivated curcumin neurology research.