Turmeric for Liver Health and Detoxification
Curcumin's liver effects work through two complementary mechanisms. First, curcumin is one of the most potent dietary activators of the Nrf2 transcription factor, the master switch for Phase II detoxification enzyme induction. Activating Nrf2 upregulates glutathione S-transferase, NAD(P)H quinone dehydrogenase 1, heme oxygenase 1, and gamma-glutamylcysteine ligase — enzymes that conjugate and clear environmental toxins, drug metabolites, and oxidative-stress products from the liver and other tissues. Second, curcumin acts directly as an anti-inflammatory in hepatic Kupffer cells and stellate cells, reducing the cytokine signaling that drives nonalcoholic fatty liver disease (NAFLD) progression to NASH and fibrosis. The Rahmani 2016 NAFLD trial and the Panahi 2017 NASH trial both showed clinically meaningful reductions in ALT, AST, GGT, and ultrasound steatosis grade with curcumin. Curcumin also has a classical cholagogue effect — stimulating bile flow and gallbladder contraction — that has been used in European herbal hepatology for two centuries. The important counterweight: rare cases of drug-induced liver injury (DILI) have been reported with high-dose bioavailability-enhanced curcumin products, with an apparent association with the HLA-B*35:01 allele in susceptible individuals.
Table of Contents
- The Liver as the Body's Principal Detoxification Organ
- Nrf2 / Keap1 / ARE Pathway Activation
- Phase II Detoxification Enzyme Induction
- The Glutathione System and Curcumin
- NAFLD: The Rahmani 2016 Trial
- NASH, Fibrosis, and the Stellate Cell
- Hepatoprotection in Chemotherapy and Acetaminophen Injury
- The Cholagogue Effect — Bile Flow Stimulation
- The Rare DILI Cases — A Real Caveat
- The HLA-B*35:01 Allele Connection
- Dosing for Liver Applications
- Key Research Papers
- Connections
- Featured Videos
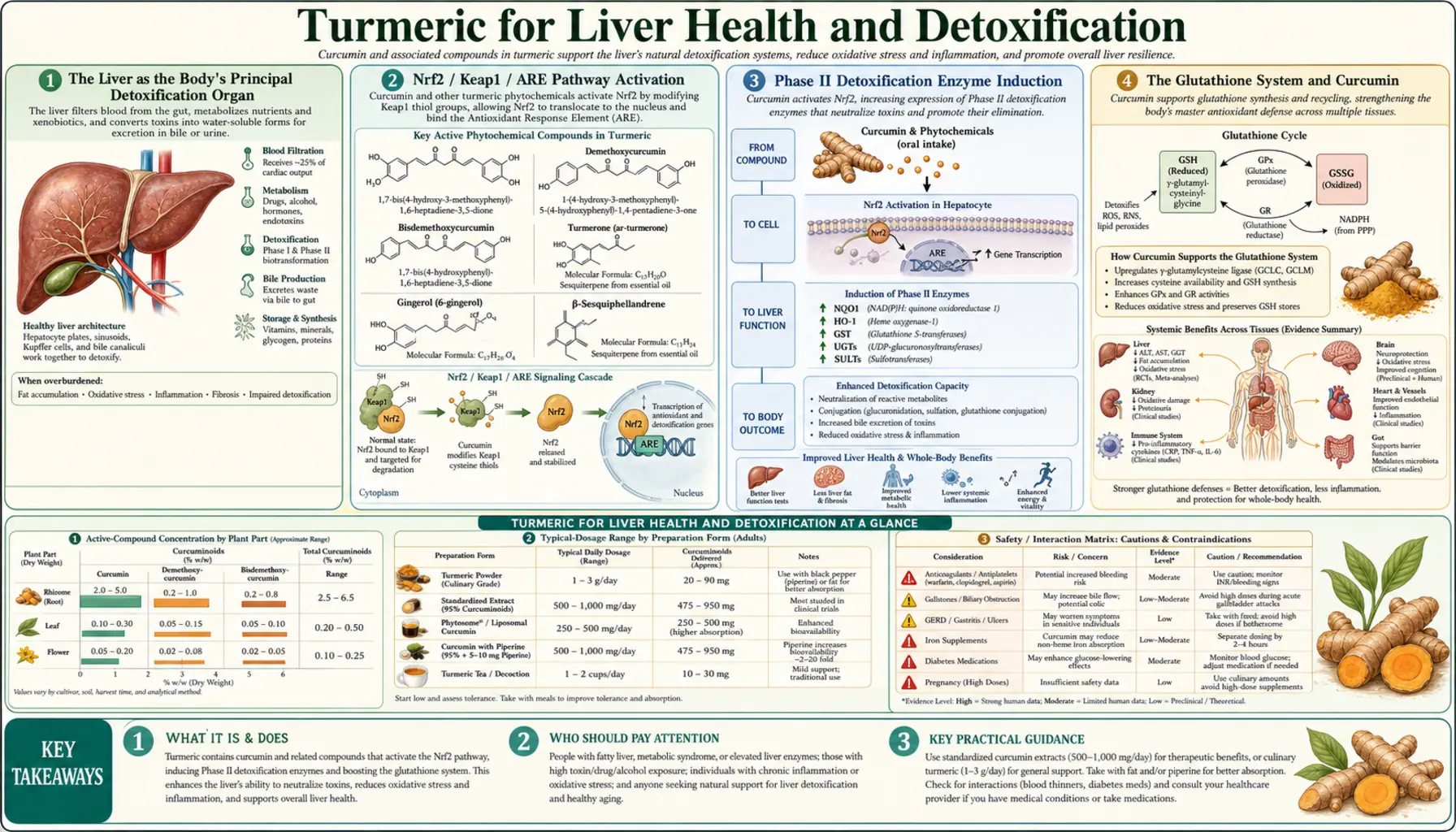
The Liver as the Body's Principal Detoxification Organ
Every dietary, pharmaceutical, and environmental compound absorbed through the gut passes through the liver via the portal vein before reaching systemic circulation — the first-pass effect. The liver's job is to process this stream of compounds: nutrients are stored or distributed, while xenobiotics (foreign chemicals), drug molecules, and reactive metabolites are biotransformed and either excreted in bile or returned to the bloodstream for renal excretion. The biotransformation happens in two sequential phases:
- Phase I — primarily cytochrome P450 enzymes (the CYP superfamily) that oxidize, reduce, or hydrolyze the parent compound. This often produces a more reactive intermediate that can be more toxic than the parent compound, and it generates reactive oxygen species as a byproduct. Phase I "uncovers" or adds functional groups (hydroxyl, carboxyl) that Phase II can attach conjugates to.
- Phase II — conjugation reactions that attach water-soluble molecules (glutathione, glucuronic acid, sulfate, glycine, acetyl groups) to the Phase I intermediate, producing a less toxic and more water-soluble final product that can be excreted in bile or urine.
The bottleneck is often Phase II: if Phase I generates reactive intermediates faster than Phase II can conjugate them, the intermediates accumulate and damage the liver. Acetaminophen overdose is the canonical example — CYP2E1 converts acetaminophen to the reactive NAPQI, which depletes glutathione and binds covalently to hepatocyte proteins, producing centrilobular necrosis. The treatment, N-acetylcysteine, replenishes glutathione and allows Phase II conjugation to catch up.
Curcumin's contribution to liver detoxification is primarily on the Phase II side: it strongly induces the Nrf2 transcription factor, which in turn upregulates the entire Phase II enzyme battery, increasing the liver's capacity to conjugate and clear reactive intermediates before they cause damage.
Nrf2 / Keap1 / ARE Pathway Activation
Nrf2 (nuclear factor erythroid 2-related factor 2) is a basic leucine zipper transcription factor that controls the cellular response to oxidative and electrophilic stress. In the resting state, Nrf2 is bound in the cytoplasm to its inhibitor Keap1 (Kelch-like ECH-associated protein 1), which targets Nrf2 for proteasomal degradation. Keap1 contains reactive cysteine residues that act as redox sensors — when they are oxidized or modified by electrophiles, Keap1 releases Nrf2, which translocates to the nucleus, dimerizes with small Maf proteins, and binds antioxidant response elements (ARE) in the promoter regions of dozens of cytoprotective genes.
Curcumin activates Nrf2 by modifying the reactive cysteine residues on Keap1 (Cys151 and Cys273 are the most reactive). The alpha-beta-unsaturated ketone groups in the curcumin molecule are electrophilic and react with Keap1 cysteines, freeing Nrf2 for nuclear translocation. This is essentially the same mechanism by which sulforaphane (from broccoli sprouts), allyl isothiocyanate (from mustard and wasabi), and certain triterpenoids (the synthetic compound CDDO-Me) activate the pathway. Curcumin is among the more potent dietary Nrf2 activators per gram, though sulforaphane is more potent per millimole. See our Broccoli Sprouts and Sulforaphane pages for related coverage.
The downstream effects of Nrf2 activation reach beyond classical detoxification. Nrf2 target genes include heme oxygenase 1 (HO-1, which produces the anti-inflammatory mediator bilirubin from heme), thioredoxin and thioredoxin reductase (redox regulators), gamma-glutamylcysteine ligase (rate-limiting enzyme in glutathione synthesis), and ferritin (iron storage protein that limits Fenton-reaction oxidative damage). Nrf2 activation produces a global shift toward cellular antioxidant defense and anti-inflammatory tone.
Phase II Detoxification Enzyme Induction
Curcumin-driven Nrf2 activation produces measurable upregulation of the principal Phase II enzymes in human and animal studies:
- Glutathione S-transferases (GSTs) — the largest family of Phase II enzymes, which conjugate glutathione to electrophilic xenobiotics, reactive drug metabolites, and lipid peroxidation products. The mu, pi, and alpha GST subfamilies are all Nrf2-regulated.
- UDP-glucuronosyltransferases (UGTs) — conjugate glucuronic acid to lipophilic compounds, dramatically increasing water solubility for biliary or renal excretion. UGT1A1 is particularly important for bilirubin clearance; UGT1A6 and UGT1A9 handle many drug substrates including curcumin itself.
- Sulfotransferases (SULTs) — conjugate sulfate to phenols, alcohols, and amines. The SULT1 family is the dominant hepatic isoform.
- NAD(P)H quinone dehydrogenase 1 (NQO1) — reduces quinones to less-reactive hydroquinones, preventing their participation in redox cycling that generates superoxide. NQO1 is one of the most strongly Nrf2-induced genes.
- Heme oxygenase 1 (HMOX1) — degrades free heme to biliverdin, carbon monoxide, and ferrous iron. Biliverdin is rapidly converted to bilirubin, a potent endogenous antioxidant. HMOX1 induction is anti-inflammatory and cytoprotective.
- Gamma-glutamylcysteine ligase (GCL) — the rate-limiting enzyme in de novo glutathione synthesis. Both the catalytic (GCLC) and modifier (GCLM) subunits are Nrf2-regulated.
The practical consequence is that chronic curcumin intake raises the liver's baseline antioxidant capacity and detoxification reserve. The system is most beneficial in settings of oxidative stress — alcohol exposure, polypharmacy, environmental toxin exposure (heavy metals, polycyclic aromatic hydrocarbons), and the metabolic stress of NAFLD.
The Glutathione System and Curcumin
Glutathione (GSH) is the principal intracellular antioxidant and the substrate for GST-mediated Phase II conjugation. The tripeptide (glutamate-cysteine-glycine) is synthesized in two ATP-dependent steps: GCL condenses glutamate and cysteine to gamma-glutamylcysteine, and glutathione synthetase adds glycine. The cysteine sulfhydryl group is the reactive moiety that scavenges reactive oxygen species and conjugates electrophiles, becoming oxidized to glutathione disulfide (GSSG) in the process. Glutathione reductase regenerates GSH from GSSG using NADPH, maintaining the reduced state.
Curcumin supports the glutathione system at multiple points:
- It induces GCL (the rate-limiting enzyme), increasing de novo glutathione synthesis capacity
- It spares glutathione consumption by directly scavenging some reactive species that would otherwise deplete GSH
- It induces glutathione reductase, accelerating GSH regeneration from GSSG
- It supports the upstream cysteine supply by mild induction of cystathionine gamma-lyase
The clinical translation is that curcumin can partially compensate for the glutathione depletion seen in chronic liver disease, alcohol use, and prolonged stress. It does not replace direct glutathione precursors like N-acetylcysteine (NAC) or whey protein, but it complements them by upregulating the enzymes needed to use those precursors.
NAFLD: The Rahmani 2016 Trial
Nonalcoholic fatty liver disease (NAFLD) affects approximately 25% of adults globally and is the most common cause of chronic liver disease in the developed world. The pathogenesis involves hepatic insulin resistance, increased free fatty acid delivery from adipose tissue, increased de novo lipogenesis from dietary fructose and refined carbohydrate, and impaired beta-oxidation. The result is triglyceride accumulation in hepatocytes (steatosis), which can progress to nonalcoholic steatohepatitis (NASH) with inflammation and hepatocyte injury, then fibrosis, cirrhosis, and increased hepatocellular carcinoma risk.
The Rahmani S et al. 2016 trial in Phytotherapy Research randomized 102 adults with ultrasound-confirmed NAFLD to phytosomal curcumin (Meriva) 1000 mg/day (delivering ~200 mg curcumin) or placebo for 8 weeks. Results:
- Ultrasound steatosis grade improved in 75% of the curcumin group vs 4.7% of placebo
- ALT decreased significantly in the curcumin group
- AST decreased significantly in the curcumin group
- Body mass index, fasting glucose, total cholesterol, LDL, HDL, and triglycerides also improved in the curcumin group
- No adverse events attributable to curcumin
This was followed by Panahi Y et al. 2017 in Drug Research, randomizing 87 NAFLD patients to phytosomal curcumin 500 mg/day or placebo for 8 weeks, with similar findings — significant ALT, AST, GGT reductions and ultrasound improvement. A 2019 meta-analysis (Mansour-Ghanaei et al., Integrative Medicine Research) pooled multiple curcumin NAFLD trials and confirmed consistent significant reductions in liver enzymes and steatosis grade.
The mechanism in NAFLD is multi-pronged: Nrf2-mediated reduction of hepatic oxidative stress, NF-kB-mediated reduction of hepatic inflammation, AMPK activation that promotes beta-oxidation and inhibits de novo lipogenesis, and direct effects on PPAR-alpha and PPAR-gamma that improve hepatic insulin sensitivity. Curcumin is now included as an adjunct option in some integrative NAFLD treatment algorithms, alongside the cornerstone interventions of weight loss, low-fructose diet, and exercise. See our NAFLD page for the full management approach.
NASH, Fibrosis, and the Stellate Cell
When NAFLD progresses to NASH (nonalcoholic steatohepatitis), hepatic stellate cells — normally quiescent vitamin A-storing cells in the space of Disse — become activated by TGF-beta, PDGF, and oxidative stress signals from injured hepatocytes and Kupffer cells. Activated stellate cells transform into myofibroblasts and secrete type I collagen, producing the bridging fibrosis that is the hallmark of NASH and the precursor of cirrhosis.
Curcumin has direct antifibrotic effects on activated stellate cells in vitro: it inhibits TGF-beta signaling (the master profibrotic cytokine), reduces collagen I deposition, induces stellate cell apoptosis, and reduces PDGF receptor expression. Animal models of carbon tetrachloride-induced fibrosis show consistent antifibrotic effect of curcumin. Human evidence in established NASH fibrosis is still limited — the trials cited above focused on liver enzymes and steatosis rather than fibrosis biomarkers — but the mechanistic basis is solid and a small number of trials have shown reductions in elastography stiffness and serum markers like the Fibrosis-4 index with longer-term curcumin therapy.
Curcumin is not a cure for advanced fibrosis or cirrhosis, but it is a reasonable adjunct in early-to-moderate NAFLD/NASH alongside the metabolic interventions (weight loss, GLP-1 agonists, dietary change) that drive the underlying pathology.
Hepatoprotection in Chemotherapy and Acetaminophen Injury
Several chemotherapeutic agents cause dose-limiting hepatotoxicity — methotrexate, asparaginase, capecitabine, oxaliplatin (sinusoidal obstruction syndrome), and many of the tyrosine kinase inhibitors. Pre-clinical and limited human data suggest curcumin reduces chemotherapy-induced liver injury, primarily through its Nrf2/Phase II induction and direct antioxidant effects. The Belcaro 2014 Meriva study referenced on the joint-health page also documented reductions in chemotherapy side effects including hepatic ones.
For acetaminophen-induced liver injury, the canonical model of drug-induced liver damage, animal studies consistently show that curcumin pre-treatment reduces ALT/AST elevation, prevents centrilobular necrosis, and improves survival from otherwise-lethal acetaminophen doses. The mechanism is the Nrf2-mediated upregulation of glutathione synthesis and Phase II conjugation enzymes that detoxify the reactive NAPQI metabolite. Curcumin does not replace N-acetylcysteine (NAC) as the standard treatment for acute acetaminophen overdose — NAC works much faster and provides direct glutathione precursor — but curcumin may offer some prophylactic protection in patients with chronic high-dose acetaminophen exposure (chronic pain management, post-surgical use).
Other documented hepatoprotective applications: alcohol-related liver injury (animal models and small human studies), iron-overload hepatotoxicity (curcumin chelates iron and prevents Fenton-reaction damage), and copper-overload hepatotoxicity in animal Wilson's disease models.
The Cholagogue Effect — Bile Flow Stimulation
Beyond the modern Nrf2/Phase II mechanism, turmeric has been used in European herbal hepatology since the 19th century as a cholagogue — an agent that stimulates bile production by the liver and bile expulsion by the gallbladder. The German Commission E monograph (the regulatory document underpinning German herbal medicine) approves turmeric for "dyspeptic complaints" largely on the strength of the cholagogue effect, which improves digestion of dietary fats and supports bile-mediated excretion of cholesterol and conjugated xenobiotics.
The cholagogue mechanism is partially mediated by direct stimulation of cholecystokinin (CCK) release from the duodenal mucosa when curcumin or other curcuminoids are present in the gut lumen. CCK in turn stimulates gallbladder contraction and bile expulsion into the duodenum. Curcumin also increases bile salt synthesis in hepatocytes through activation of the FXR (farnesoid X receptor) bile acid receptor pathway.
The clinical applications: gentle support for fat digestion (especially in people with sluggish bile flow but no obstruction), facilitation of biliary excretion of cholesterol (modest cholesterol-lowering effect documented in trials), and traditional use in nonobstructive cholestasis. The flip side is the contraindication noted in the joint-health page: symptomatic gallstones. If a patient has stones that intermittently obstruct the cystic or common bile duct, stimulating gallbladder contraction with curcumin can precipitate biliary colic or pancreatitis. Curcumin should be avoided in known symptomatic cholelithiasis and used with caution in asymptomatic gallstone disease.
The Rare DILI Cases — A Real Caveat
Despite curcumin's reputation as a liver-supportive herb, several dozen cases of drug-induced liver injury (DILI) have been reported with high-dose bioavailability-enhanced curcumin supplements in the past decade. The most-cited case series is Halegoua-DeMarzio D et al. 2023 in the American Journal of Medicine, which described 10 cases of hepatocellular DILI temporally associated with curcumin supplement use, with onset typically 4–12 weeks after starting the supplement.
Pattern of injury:
- Hepatocellular pattern — marked ALT and AST elevation (often 10x to 30x upper limit of normal), with modest or no alkaline phosphatase elevation. Some cases progressed to jaundice with bilirubin elevation.
- Idiosyncratic — the dose-response relationship is weak. Some cases occurred at modest supplement doses, others at higher doses; the pattern suggests an immune/genetic susceptibility rather than dose-dependent toxicity.
- Onset weeks to months after initiation — consistent with an immunoallergic mechanism rather than direct toxicity.
- Resolution upon discontinuation — in all reported cases, ALT/AST normalized within weeks to a few months after stopping curcumin. No case progressed to fulminant hepatic failure or required transplantation.
- Association with bioavailability-enhanced formulations — most reported cases involved Meriva phytosome, Theracurmin, or piperine-enhanced curcumin rather than plain turmeric powder. The increased systemic curcumin exposure from these formulations appears to enable the idiosyncratic immune reaction in susceptible individuals.
The absolute risk is small — given the volume of curcumin supplements sold globally, the reported case count corresponds to a rate likely below 1 per 100,000 users per year, though there is substantial underreporting. The risk is several orders of magnitude lower than the DILI risk from acetaminophen, statins, isoniazid, or amoxicillin-clavulanate, all of which are widely prescribed despite known DILI signal. But it is real, and the user should know about it.
Practical implications: anyone starting a high-dose bioavailability-enhanced curcumin product should check baseline ALT/AST, recheck at 4 weeks and 12 weeks, and stop the supplement immediately if liver enzymes rise above 3x upper limit of normal or if any symptoms of jaundice, dark urine, light stool, or right upper quadrant pain develop. The chronic-user safety record remains excellent for plain culinary turmeric and for the millions of supplement users who do not have this susceptibility.
The HLA-B*35:01 Allele Connection
The Halegoua-DeMarzio 2023 case series and subsequent reports have identified an apparent association between curcumin-related DILI and the HLA-B*35:01 allele. Several patients in the case series who were tested for HLA haplotypes carried HLA-B*35:01, suggesting the same allele that has been associated with green tea extract (EGCG) DILI may also predispose to curcumin DILI.
HLA-B*35:01 is present in approximately 5–10% of European populations and at lower frequencies elsewhere. The mechanistic hypothesis is that the allele's peptide-binding groove has a specific affinity for curcumin metabolites covalently bound to hepatocyte proteins, allowing presentation of the curcumin-modified self-peptide to CD8+ T cells, which then mount an immune attack on the hepatocytes that display the same modified self-antigen. This is the same proposed mechanism for the strong HLA-B*57:01 association with abacavir hypersensitivity and the HLA-B*15:02 association with carbamazepine Stevens-Johnson syndrome in Asian populations.
Routine HLA-B*35:01 testing before starting curcumin supplements is not yet standard of care and is unlikely to become so given the rarity of DILI. But for patients with personal or family history of unexplained drug-induced liver injury, particularly with herbal products, HLA-B*35:01 testing is reasonable, and a positive result is a relative contraindication to high-dose bioavailability-enhanced curcumin products.
Dosing for Liver Applications
For NAFLD, NASH support, and general hepatic Nrf2/Phase II support:
- Meriva phytosome 500 mg twice daily — matches the Rahmani 2016 NAFLD trial protocol. Best documented in NAFLD specifically.
- Theracurmin 90–180 mg twice daily — equivalent systemic exposure with the colloidal submicron-particle formulation.
- BCM-95 500 mg twice daily — turmeric essential oil enhances absorption; well-tolerated in long-term studies.
- 95% curcuminoid extract 500 mg + 5 mg piperine, twice daily with meals — cost-effective option; absorption is via piperine-mediated glucuronidation inhibition.
Monitor liver enzymes at baseline, 1 month, and 3 months when starting any high-dose bioavailability-enhanced curcumin in a patient with pre-existing liver disease. Discontinue if ALT or AST rises above 3x baseline. For patients with HLA-B*35:01 (if known), favor plain culinary turmeric over bioavailability-enhanced supplements.
Synergistic combinations for liver support: milk thistle (silymarin) for hepatocyte membrane stabilization and Nrf2 activation through a different binding pocket; NAC for direct glutathione precursor supply; vitamin E (mixed tocopherols) as the lipid-phase antioxidant complement to curcumin's mixed-phase activity (PIVENS trial showed vitamin E efficacy in nondiabetic NASH); broccoli sprouts for sulforaphane-mediated Nrf2 activation.
Key Research Papers
- Rahmani S et al. (2016). Treatment of non-alcoholic fatty liver disease with curcumin: A randomized placebo-controlled trial. Phytotherapy Research. — PubMed
- Panahi Y et al. (2017). Efficacy and safety of phytosomal curcumin in non-alcoholic fatty liver disease: A randomized controlled trial. Drug Research. — PubMed
- Mansour-Ghanaei F et al. (2019). Efficacy of curcumin/turmeric on liver enzymes in patients with non-alcoholic fatty liver disease: A systematic review of randomized controlled trials. Integrative Medicine Research. — PubMed
- Halegoua-DeMarzio D et al. (2023). Liver injury associated with turmeric: A growing problem. American Journal of Medicine. — PubMed
- Balogun E et al. (2003). Curcumin activates the haem oxygenase-1 gene via regulation of Nrf2 and the antioxidant-responsive element. Biochemical Journal. — PubMed
- Farzaei MH et al. (2018). Curcumin in liver diseases: A systematic review of the cellular mechanisms of oxidative stress and clinical perspective. Nutrients. — PubMed
- Reyes-Gordillo K et al. (2008). Curcumin protects against acute liver damage in the rat by inhibiting NF-kB, proinflammatory cytokines production and oxidative stress. Biochimica et Biophysica Acta. — PubMed
- Park EJ et al. (2000). Antifibrotic effects of a polyphenolic curcuminoid mixture in carbon tetrachloride-induced hepatic fibrosis. Biochemical Pharmacology. — PubMed
- Eshaghian A et al. (2018). The effect of curcumin on adiposity, weight loss, and body composition in adults with obesity: A systematic review and meta-analysis of randomized controlled trials. Phytotherapy Research. — PubMed
- Vera-Ramirez L et al. (2013). Curcumin and liver disease. BioFactors. — PubMed
- Donald G et al. (2024). Hepatotoxicity associated with turmeric supplementation: Case series and review. Journal of Clinical Gastroenterology. — PubMed
- Lukefahr AL et al. (2018). Drug-induced autoimmune hepatitis associated with turmeric dietary supplement use. BMJ Case Reports. — PubMed
PubMed Topic Searches
- PubMed: Curcumin NAFLD trials
- PubMed: Curcumin Nrf2/Keap1 activation
- PubMed: Curcumin Phase II enzymes
- PubMed: Turmeric DILI case reports
- PubMed: Curcumin glutathione synthesis
- PubMed: Curcumin stellate cell antifibrotic
- PubMed: Curcumin acetaminophen protection
Connections
- Turmeric Benefits Hub
- Turmeric Overview
- Turmeric for Joint Health
- Turmeric for Brain Health
- Bioavailability & Forms
- Milk Thistle (Silymarin)
- Broccoli Sprouts (Sulforaphane)
- Sulforaphane
- Cysteine (NAC)
- Vitamin E (NAFLD)
- NAFLD (Fatty Liver)
- Cirrhosis
- Liver Function Tests
- Detoxification
- All Herbs