Turmeric for Anti-Inflammatory and Joint Health
Joint pain — particularly osteoarthritis of the knee — is where the curcumin clinical evidence base is strongest and most consistent. The pivotal Daily et al. 2016 meta-analysis pooled eight randomized controlled trials (n=606 participants) and concluded that turmeric extracts at approximately 1000 mg/day curcumin produced pain and function improvements comparable to NSAIDs (ibuprofen, diclofenac) on validated osteoarthritis outcome measures (VAS pain score, WOMAC, Lequesne index), with a markedly lower rate of gastrointestinal side effects. The Henrotin 2013 review reached similar conclusions for rheumatoid arthritis, where curcumin produced reductions in DAS-28 disease activity, swollen joint count, and tender joint count comparable to diclofenac in a controlled trial. The multi-target mechanism — NF-kB inhibition, COX-2 and LOX suppression, downregulation of TNF-alpha and IL-6, and inhibition of cartilage-degrading matrix metalloproteinases — explains both why curcumin works on multiple inflammatory joint conditions and why most clinical trials use bioavailability-enhanced formulations like Meriva (curcumin phytosome) rather than crude turmeric powder.
Table of Contents
- Why Joint Conditions Respond to Curcumin
- NF-kB Inhibition — The Master Anti-Inflammatory Switch
- COX-2 and LOX Inhibition — NSAID-Like Activity Without GI Toxicity
- Cytokine Suppression (TNF-alpha, IL-1beta, IL-6)
- Matrix Metalloproteinase Inhibition and Cartilage Preservation
- The Daily 2016 Meta-Analysis (Osteoarthritis)
- The Henrotin 2013 Review and Chandran RA Trial
- The Belcaro Meriva Long-Term Osteoarthritis Trials
- Curcumin vs Ibuprofen and Diclofenac Head-to-Head
- Dosing Protocols for Joint Conditions
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
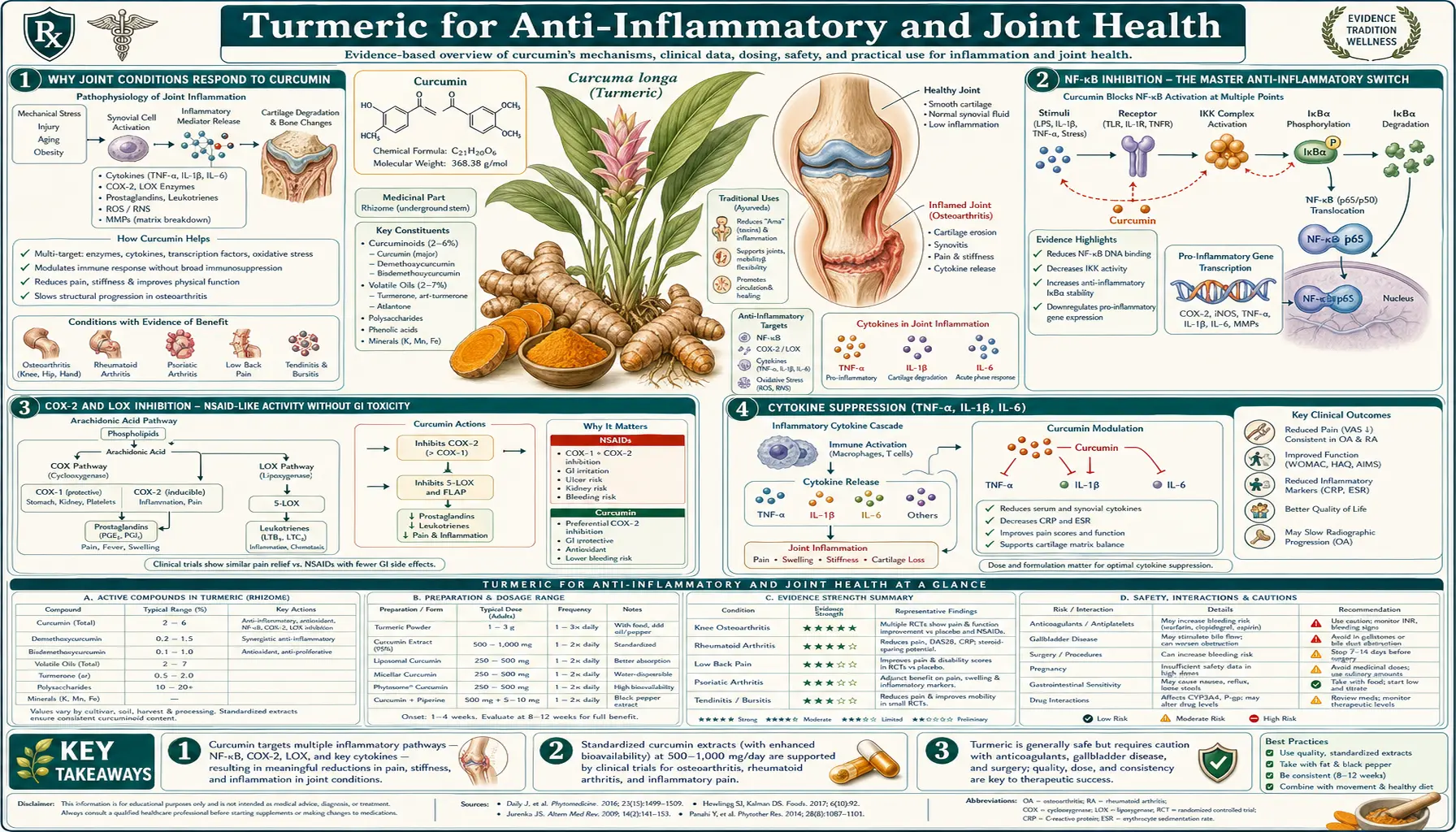
Why Joint Conditions Respond to Curcumin
Osteoarthritis (OA) and rheumatoid arthritis (RA), despite their different pathogenesis, share a common downstream pathway of joint destruction driven by inflammatory cytokines, prostaglandins, and matrix-degrading enzymes. In OA, the initiating insult is typically mechanical — cartilage wear that triggers a chondrocyte stress response, releasing IL-1beta and IL-6, which in turn drive matrix metalloproteinase (MMP-3, MMP-13) production and further cartilage breakdown. In RA, the initiating insult is autoimmune, with synovial fibroblasts and T cells driving TNF-alpha and IL-17 production, recruiting neutrophils, and producing pannus tissue that erodes cartilage and bone.
Standard pharmacotherapy targets specific nodes of this cascade: NSAIDs block COX-1 and COX-2 to reduce prostaglandin-mediated pain and inflammation; biologics (etanercept, infliximab, adalimumab) directly neutralize TNF-alpha; IL-6 inhibitors (tocilizumab) block the IL-6 receptor; JAK inhibitors (tofacitinib, baricitinib) interrupt cytokine signaling. The single-target precision of these drugs is also their vulnerability — blocking one cytokine often shifts the inflammatory program to another pathway, requiring drug rotation or combination therapy.
Curcumin's appeal in this context is its multi-target action. The same molecule that inhibits NF-kB also inhibits COX-2 and 5-LOX, suppresses TNF-alpha and IL-6 production, downregulates MMP-3 and MMP-13, and activates Nrf2-mediated antioxidant defenses. No single mechanism is as potent as a targeted biologic, but the combined effect on the inflammatory cascade is clinically meaningful in osteoarthritis and modestly effective in rheumatoid arthritis as monotherapy — with a side-effect profile that resembles placebo rather than ibuprofen or methotrexate.
NF-kB Inhibition — The Master Anti-Inflammatory Switch
NF-kB (nuclear factor kappa-light-chain-enhancer of activated B cells) is the master transcription factor controlling inflammatory gene expression. In the resting state, NF-kB is held in the cytoplasm by its inhibitor IkB. When a cell receives an inflammatory signal — via TLR receptors, TNF receptor, IL-1 receptor, or oxidative stress — IkB is phosphorylated by the IKK complex and tagged for proteasomal degradation. Free NF-kB then translocates to the nucleus and binds promoter regions of hundreds of inflammatory target genes: TNF-alpha, IL-1beta, IL-6, IL-8, COX-2, iNOS, MMP-9, ICAM-1, VCAM-1, and many more.
Curcumin blocks this cascade at multiple points. Most importantly, curcumin inhibits IKK activation, preventing IkB phosphorylation and keeping NF-kB sequestered in the cytoplasm. The downstream effect is broad suppression of inflammatory gene transcription — not just one cytokine but the entire NF-kB-controlled program. The Singh 1995 paper in Journal of Biological Chemistry was an early demonstration; the Aggarwal group has published dozens of mechanistic papers since.
This NF-kB inhibition is what unifies curcumin's effects across osteoarthritis, rheumatoid arthritis, inflammatory bowel disease, atopic dermatitis, and several other chronic inflammatory conditions. The same molecular switch is dysregulated in all of them.
COX-2 and LOX Inhibition — NSAID-Like Activity Without GI Toxicity
Beyond gene transcription, curcumin directly inhibits the enzymes that produce inflammatory lipid mediators. Cyclooxygenase-2 (COX-2) converts arachidonic acid to prostaglandin H2, the precursor of PGE2, PGI2, and thromboxane — the prostanoid family that drives pain, fever, and vasodilation in inflamed tissue. NSAIDs (aspirin, ibuprofen, naproxen, diclofenac, celecoxib) work through COX inhibition. Curcumin produces similar prostaglandin reductions but through a different binding mode that does not appear to compromise the gastric mucosal protective effect of COX-1.
5-Lipoxygenase (5-LOX) is the parallel enzyme that converts arachidonic acid to the leukotriene family (LTB4, LTC4, LTD4, LTE4) — mediators of bronchoconstriction, neutrophil chemotaxis, and vascular permeability. Curcumin inhibits 5-LOX in addition to COX-2, giving it a broader anti-inflammatory profile than purely COX-targeted NSAIDs. (Boswellia is a more potent and selective 5-LOX inhibitor; the combination of curcumin and boswellia is a common synergistic anti-inflammatory pairing — see our Boswellia page.)
The crucial clinical distinction from NSAIDs: curcumin does not cause gastric mucosal injury and does not increase cardiovascular risk. In fact, curcumin appears mildly protective to gastric mucosa in animal models, possibly through its antioxidant and Nrf2-mediated cytoprotective effects. The gastrointestinal bleeding, ulceration, and renal toxicity that limit chronic NSAID use are not features of curcumin therapy. The trade-off is that curcumin's analgesic potency per dose is lower than NSAIDs — it works but takes longer and requires higher daily milligram quantities.
Cytokine Suppression (TNF-alpha, IL-1beta, IL-6)
Through its NF-kB inhibition and additional direct effects, curcumin reduces production of the three cytokines most central to chronic inflammatory disease:
- TNF-alpha (tumor necrosis factor alpha) — the central cytokine in rheumatoid arthritis pathogenesis. Anti-TNF biologics (etanercept, infliximab, adalimumab) revolutionized RA treatment in the 1990s. Curcumin produces dose-dependent TNF-alpha reductions in human peripheral blood mononuclear cells and reduces serum TNF-alpha in RA patients in controlled trials.
- IL-1beta (interleukin-1 beta) — the primary driver of chondrocyte stress in osteoarthritis. IL-1beta directly induces MMP-3 and MMP-13 production by chondrocytes, accelerating cartilage breakdown. Curcumin suppresses IL-1beta production in synovial macrophages and chondrocytes.
- IL-6 (interleukin-6) — the principal acute-phase cytokine, driving liver production of C-reactive protein. Elevated serum IL-6 and CRP are biomarkers of chronic inflammation and predictors of cardiovascular events. Curcumin reduces both IL-6 and CRP in multiple meta-analyses of cardiometabolic trials.
The Sahebkar 2014 meta-analysis of 9 randomized trials in 690 patients found curcumin reduced circulating CRP by an average of 6.4 mg/L, a clinically meaningful drop comparable to what statins achieve. The effect was larger with bioavailability-enhanced formulations and with longer treatment duration.
Matrix Metalloproteinase Inhibition and Cartilage Preservation
Articular cartilage is composed of type II collagen and aggrecan (a large proteoglycan) embedded in a network of glycosaminoglycans. When chondrocytes are stressed — by mechanical loading in OA or by inflammatory cytokines in RA — they upregulate production of matrix metalloproteinases (MMPs) and aggrecanases (ADAMTS-4, ADAMTS-5) that cleave the cartilage extracellular matrix. MMP-13 is particularly destructive because it has high specific activity against type II collagen, and once collagen network integrity is lost, cartilage cannot regenerate.
Curcumin directly inhibits MMP-3 and MMP-13 transcription in chondrocyte cultures, both at the protein production level and at the enzymatic activity level. This effect distinguishes curcumin from pure analgesic therapy — symptomatic NSAIDs reduce pain perception without slowing cartilage loss, while curcumin may modestly slow the structural progression of OA in addition to its symptomatic effect. Long-term radiographic outcome data are still limited, but the mechanism is biologically plausible and consistent with the favorable WOMAC-Function scores in the longer Meriva trials.
The Daily 2016 Meta-Analysis (Osteoarthritis)
The Daily JW, Yang M, Park S meta-analysis published in the Journal of Medicinal Food in 2016 is the most widely cited consolidation of curcumin osteoarthritis data. The authors pooled eight randomized controlled trials totaling 606 participants, all of whom had clinically diagnosed knee osteoarthritis (Kellgren-Lawrence grade II-III on radiographs in most studies). Interventions varied across the trials but the median curcumin dose was approximately 1000 mg/day, often in the form of standardized 95%-curcuminoid extracts with piperine, or as Meriva phytosome at equivalent curcumin content.
Key findings:
- Pain reduction — curcumin produced statistically significant pain reductions on the visual analog scale (VAS) versus placebo, with an effect size comparable to that seen with ibuprofen in head-to-head trials.
- Function improvement — WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) function and stiffness subscales both showed significant improvement.
- NSAID equivalence — in the four trials with active NSAID comparators (ibuprofen 1200–1800 mg/day or diclofenac 100 mg/day), curcumin produced equivalent pain and function outcomes.
- Side-effect advantage — gastrointestinal adverse events were markedly lower with curcumin than with NSAID comparators; dropout rates due to side effects were lower.
- Time to effect — clinical benefit became measurable after approximately 4 weeks, slower than NSAIDs (which work within hours) but cumulative through 12 weeks of treatment.
The authors' conclusion was cautious but supportive: "Eight RCTs met the eligibility criteria. The meta-analysis result suggested that turmeric extracts may be more effective for relieving pain and improving function compared with placebo. ... The number of identified trials and the methodological quality of these trials are not yet sufficient to draw definitive conclusions."
Practically, the Daily meta-analysis is the citation most rheumatologists and integrative-medicine clinicians point to when discussing curcumin as an evidence-based first-line option for mild-to-moderate knee OA, particularly in patients who cannot tolerate NSAIDs because of GI bleeding history, renal insufficiency, or cardiovascular risk.
The Henrotin 2013 Review and Chandran RA Trial
For rheumatoid arthritis, the Henrotin Y, Priem F, Mobasheri A 2013 review in SpringerPlus consolidated the curcumin RA literature, drawing on both controlled clinical trials and mechanistic studies. The most clinically informative single trial referenced is the Chandran B and Goel A 2012 study in Phytotherapy Research, a small (n=45) randomized active-comparator trial of curcumin 500 mg twice daily vs diclofenac 50 mg twice daily vs the combination, in patients with active rheumatoid arthritis.
Chandran results at 8 weeks:
- The curcumin-only group had the largest reduction in DAS-28 (Disease Activity Score in 28 joints), the gold-standard composite RA disease activity measure
- Curcumin produced significant reductions in swollen joint count and tender joint count, both individual components of DAS-28
- ACR-20 response rate (American College of Rheumatology criteria for 20% improvement) was higher in the curcumin arm than the diclofenac arm
- Side effects in the curcumin group were minimal; the diclofenac arm had the expected NSAID GI effects
The study was small and short, and curcumin should not be considered a replacement for DMARD therapy (methotrexate, biologics) in moderate-to-severe RA — the disease-modifying outcomes that prevent joint destruction require the more aggressive therapies. But for mild RA, for adjunct therapy to a DMARD regimen, and for patients in the early symptomatic period awaiting DMARD effect, the Chandran data support curcumin as a reasonable option.
See our Rheumatoid Arthritis page for the broader treatment landscape.
The Belcaro Meriva Long-Term Osteoarthritis Trials
The longest-duration human curcumin trials in osteoarthritis are the Belcaro G et al. studies of Meriva (Indena's curcumin-phosphatidylcholine phytosome complex). The Belcaro 2010 Alternative Medicine Review study followed 50 patients with knee OA on Meriva 1000 mg/day (delivering ~200 mg curcumin) for 3 months; the Belcaro 2014 follow-up extended observation to 8 months in a larger cohort.
Findings:
- Mean WOMAC score decreased by approximately 58% over 3 months in the Belcaro 2010 cohort
- Walking distance on treadmill testing increased substantially (mean ~1300% in some subgroups, though baseline was very low)
- Concomitant NSAID use dropped by 63%
- Significant reductions in inflammatory biomarkers (CRP, ESR, plasma peroxide)
- No serious adverse events; the Meriva formulation was well tolerated for the 8-month period
The Belcaro trials were not blinded and did not have a placebo comparator, which limits the strength of the conclusions — some of the magnitude of improvement is likely placebo effect plus regression to the mean. But the long duration and the consistency with the smaller randomized trials lend support to Meriva as a well-tolerated long-term option, and the trials provide the practical observation that bioavailability-enhanced curcumin can reduce NSAID requirement in OA patients.
Meriva-format clinical trials continue to dominate the published OA literature because Indena collaborates with multiple academic centers and the formulation has reliable bioavailability characteristics. Other phytosome and submicron-particle formulations have similar mechanisms but less long-term human safety and efficacy data.
Curcumin vs Ibuprofen and Diclofenac Head-to-Head
Several randomized active-comparator trials have pitted curcumin directly against NSAIDs in OA:
- Kuptniratsaikul 2014 — the largest head-to-head, randomized 367 patients with knee OA to Curcuma domestica extract 1500 mg/day vs ibuprofen 1200 mg/day for 4 weeks. WOMAC scores improved equivalently in both groups. Gastrointestinal adverse events were significantly more common in the ibuprofen arm.
- Kuptniratsaikul 2009 — the earlier 107-patient version of the same comparison reached essentially identical conclusions: equivalent pain and function outcomes, fewer GI side effects with curcumin.
- Shep 2019 — randomized 139 knee OA patients to curcumin 500 mg three times daily vs diclofenac 50 mg twice daily for 28 days. Both groups showed similar reductions in VAS pain; the curcumin group reported fewer adverse events and zero serious adverse events vs four in the diclofenac arm.
- Madhu 2013 — smaller crossover-design study, curcumin (BCM-95) 500 mg twice daily vs naproxen 500 mg twice daily; comparable efficacy with better tolerability for curcumin.
The pooled message across these trials is consistent: for knee OA, curcumin at 1000–1500 mg/day of standardized 95%-curcuminoid extract (or bioavailability-equivalent doses of Meriva, Theracurmin, or BCM-95) produces pain and function outcomes equivalent to standard-dose ibuprofen or diclofenac, with substantially fewer adverse events. This is unusual in nutritional and herbal medicine and is largely what has made curcumin a mainstream integrative-medicine option rather than a fringe choice.
The caveat that requires repeating: this evidence base is largely with bioavailability-enhanced formulations or with piperine co-administration. Plain turmeric powder in food does not achieve these effects.
Dosing Protocols for Joint Conditions
Common evidence-supported regimens for osteoarthritis or rheumatoid arthritis:
- Meriva (curcumin phytosome) 500 mg twice daily — delivering ~100 mg actual curcumin per dose. Used in the Belcaro long-term OA trials. Typical effect onset 2–4 weeks.
- Theracurmin 90 mg twice daily — equivalent systemic curcumin exposure to higher milligram doses of standard extract. Less long-duration joint-specific data than Meriva, but proven absorption.
- 95% curcuminoid extract 500 mg + 5–20 mg piperine, three times daily — the most cost-effective regimen. Mimics the Kuptniratsaikul trials. Take with fatty meal for optimal absorption.
- BCM-95 (curcumin + turmeric essential oil) 500 mg twice daily — the turmeric essential oil fraction acts as a self-emulsifying absorption enhancer. Used in the Chandran RA trial and Madhu OA trial.
- Longvida SLCP 400–1000 mg/day — the highest free-curcumin bioavailability formulation. More commonly used for cognitive applications; growing OA literature.
Allow 4–8 weeks for full effect. Curcumin is not an acute analgesic like ibuprofen — it does not relieve pain within an hour. The mechanism is progressive reduction of joint inflammation, and the pain reduction is consequence rather than direct effect.
Combination with other anti-inflammatory herbs may be synergistic: boswellia for additional 5-LOX inhibition, ginger for COX-2 inhibition and prokinetic gut effect, and omega-3 fatty acids for resolvin and protectin production that actively resolves inflammation. Many commercial joint-support formulations combine these.
Cautions and Drug Interactions
- Anticoagulants and antiplatelets — curcumin has mild antiplatelet effect in vitro and may potentiate warfarin, clopidogrel, aspirin, and DOAC anticoagulants. Patients on therapeutic anticoagulation should discuss curcumin with their prescriber; INR monitoring is appropriate when starting curcumin on warfarin. The interaction is modest but real.
- Pre-surgical discontinuation — stop curcumin supplements at least 1–2 weeks before any planned surgery to allow platelet function to normalize, consistent with general bleeding-risk practice for fish oil, garlic extract, and ginkgo.
- Gallbladder disease — curcumin is a cholagogue (it stimulates gallbladder contraction). Patients with symptomatic gallstones or bile duct obstruction should avoid high-dose curcumin, which could precipitate biliary colic.
- Iron absorption interference — very high doses of curcumin chelate iron in the gut and may worsen iron-deficiency anemia. Separate curcumin and iron supplements by 2–4 hours.
- Drug metabolism (CYP3A4, P-glycoprotein) — curcumin inhibits CYP3A4 and P-glycoprotein at higher doses, which can elevate plasma levels of drugs that depend on these pathways for clearance (some statins, calcium channel blockers, immunosuppressants). Clinically meaningful at gram-scale daily doses; minor at typical supplement doses.
- Pregnancy and breastfeeding — culinary turmeric is safe in normal food quantities. High-dose curcumin supplements are not recommended in pregnancy due to insufficient safety data and theoretical uterine-stimulant concerns.
- Rare DILI cases — see the Liver Health page for discussion of the rare drug-induced liver injury reports with high-dose bioavailability-enhanced curcumin formulations. This appears to be idiosyncratic rather than dose-related, with the highest signal in patients with the HLA-B*35:01 allele.
Key Research Papers
- Daily JW, Yang M, Park S (2016). Efficacy of turmeric extracts and curcumin for alleviating the symptoms of joint arthritis: A systematic review and meta-analysis of randomized clinical trials. Journal of Medicinal Food. — PubMed
- Henrotin Y, Priem F, Mobasheri A (2013). Curcumin: A new paradigm and therapeutic opportunity for the treatment of osteoarthritis. SpringerPlus. — PubMed
- Chandran B, Goel A (2012). A randomized, pilot study to assess the efficacy and safety of curcumin in patients with active rheumatoid arthritis. Phytotherapy Research. — PubMed
- Belcaro G et al. (2010). Product-evaluation registry of Meriva, a curcumin-phosphatidylcholine complex, for the complementary management of osteoarthritis. Alternative Medicine Review. — PubMed
- Belcaro G et al. (2014). A controlled study of a lecithinized delivery system of curcumin (Meriva) to alleviate the adverse effects of cancer treatment. Phytotherapy Research. — PubMed
- Kuptniratsaikul V et al. (2014). Efficacy and safety of Curcuma domestica extracts compared with ibuprofen in patients with knee osteoarthritis: A multicenter study. Clinical Interventions in Aging. — PubMed
- Kuptniratsaikul V et al. (2009). Efficacy and safety of Curcuma domestica extracts in patients with knee osteoarthritis. Journal of Alternative and Complementary Medicine. — PubMed
- Shep D et al. (2019). Safety and efficacy of curcumin versus diclofenac in knee osteoarthritis: A randomized open-label parallel-arm study. Trials. — PubMed
- Sahebkar A (2014). Are curcuminoids effective C-reactive protein-lowering agents in clinical practice? Evidence from a meta-analysis. Phytotherapy Research. — PubMed
- Singh S, Aggarwal BB (1995). Activation of transcription factor NF-kappa B is suppressed by curcumin (diferuloylmethane). Journal of Biological Chemistry. — PubMed
- Madhu K et al. (2013). Safety and efficacy of Curcuma longa extract in the treatment of painful knee osteoarthritis: A randomized placebo-controlled trial. Inflammopharmacology. — PubMed
- Panahi Y et al. (2014). Curcuminoid treatment for knee osteoarthritis: A randomized double-blind placebo-controlled trial. Phytotherapy Research. — PubMed
- Aggarwal BB, Harikumar KB (2009). Potential therapeutic effects of curcumin against neurodegenerative, cardiovascular, pulmonary, metabolic, autoimmune and neoplastic diseases. International Journal of Biochemistry & Cell Biology. — PubMed
PubMed Topic Searches
- PubMed: Curcumin knee OA meta-analyses
- PubMed: Curcumin rheumatoid arthritis trials
- PubMed: Curcumin NF-kB inhibition
- PubMed: Curcumin TNF-alpha / IL-6 suppression
- PubMed: Meriva phytosome osteoarthritis
- PubMed: Curcumin COX-2 inhibition
- PubMed: Curcumin vs ibuprofen
Connections
- Turmeric Benefits Hub
- Turmeric Overview
- Turmeric for Liver Health
- Turmeric for Brain Health
- Bioavailability & Forms
- Boswellia (5-LOX Inhibitor)
- Ginger
- Black Pepper (Piperine)
- Omega-3 Fatty Acids
- Arthritis
- Rheumatoid Arthritis
- Osteoarthritis — the joint condition behind the Daily 2016 curcumin meta-analysis.
- Anti-Inflammatory Diet
- Aspirin (NSAID Comparison)
- All Herbs