Tea Tree — Benefits Deep Dive
Tea tree oil is the steam-distilled essential oil of Melaleuca alternifolia, a small paperbark tree native to the swampy northeast coast of New South Wales, Australia. Despite the common name, the plant has no botanical or chemical relationship to the tea plant (Camellia sinensis) — the name comes from 18th-century British sailors who brewed a tea-like infusion from the leaves. The Aboriginal Bundjalung people of northern New South Wales used crushed leaves topically for wounds, skin infections, and insect bites for thousands of years before European contact. The oil's principal antimicrobial compound is terpinen-4-ol (30–48% of the oil by international standard ISO 4730), supported by alpha-terpineol, 1,8-cineole, and other monoterpenes. Modern commercial production is centered in northern New South Wales, with global annual output of approximately 600 tonnes. Four benefit pages below cover the conditions where tea tree oil has the largest body of peer-reviewed clinical evidence — antimicrobial activity against MRSA and hospital-acquired pathogens, acne, fungal infections including onychomycosis and tinea pedis, and head lice / scabies infestation.
Deep-Dive Articles
Antimicrobial & MRSA
The Carson, Hammer & Riley 2006 Clinical Microbiology Reviews landmark review documenting in vitro activity against >60 bacterial and fungal species, MRSA decolonization trials comparing 5% tea tree to mupirocin, the terpinen-4-ol membrane-disruption mechanism, hospital infection control protocols, the standardized 5% topical concentration, and why bacteria rarely develop resistance.
Acne
The pivotal Bassett, Pannowitz & Barnetson 1990 Medical Journal of Australia head-to-head trial of 5% tea tree gel vs 5% benzoyl peroxide lotion in 124 patients — similar efficacy at reducing inflammatory lesions, with substantially less scaling, dryness, and irritation. Mechanism via Cutibacterium acnes membrane disruption plus anti-inflammatory cytokine modulation, commercial 5% tea tree gels, and how it compares to retinoids.
Antifungal & Nail Fungus
The Buck, Nidorf & Addino 1994 Journal of Family Practice onychomycosis trial of 100% tea tree oil vs 1% clotrimazole solution, athlete's foot (tinea pedis) trials, the slow-but-effective profile of topical antifungals for nail infection, why 6–12 months of daily application is realistic, and how tea tree compares to oral terbinafine.
Head Lice & Scabies
The Barker & Altman 2010 randomized head-lice trial comparing tea tree + lavender vs permethrin (with tea tree showing superior pediculicidal and ovicidal activity in vitro), the scabies pilot data using 5% tea tree, terpene insecticidal mechanism against arthropod nervous systems, and the relevance for permethrin-resistant infestations now common worldwide.
Table of Contents
- Deep-Dive Articles
- Why Tea Tree Produces Antimicrobial, Antifungal, and Insecticidal Effects
- Research Papers: Antimicrobial & MRSA
- Research Papers: Acne
- Research Papers: Antifungal & Nail Fungus
- Research Papers: Head Lice & Scabies
- Research Papers: Cross-Cutting (Chemistry, Safety, Toxicity)
- External Authoritative Resources
- Connections
- Featured Videos
Why Tea Tree Produces Antimicrobial, Antifungal, and Insecticidal Effects
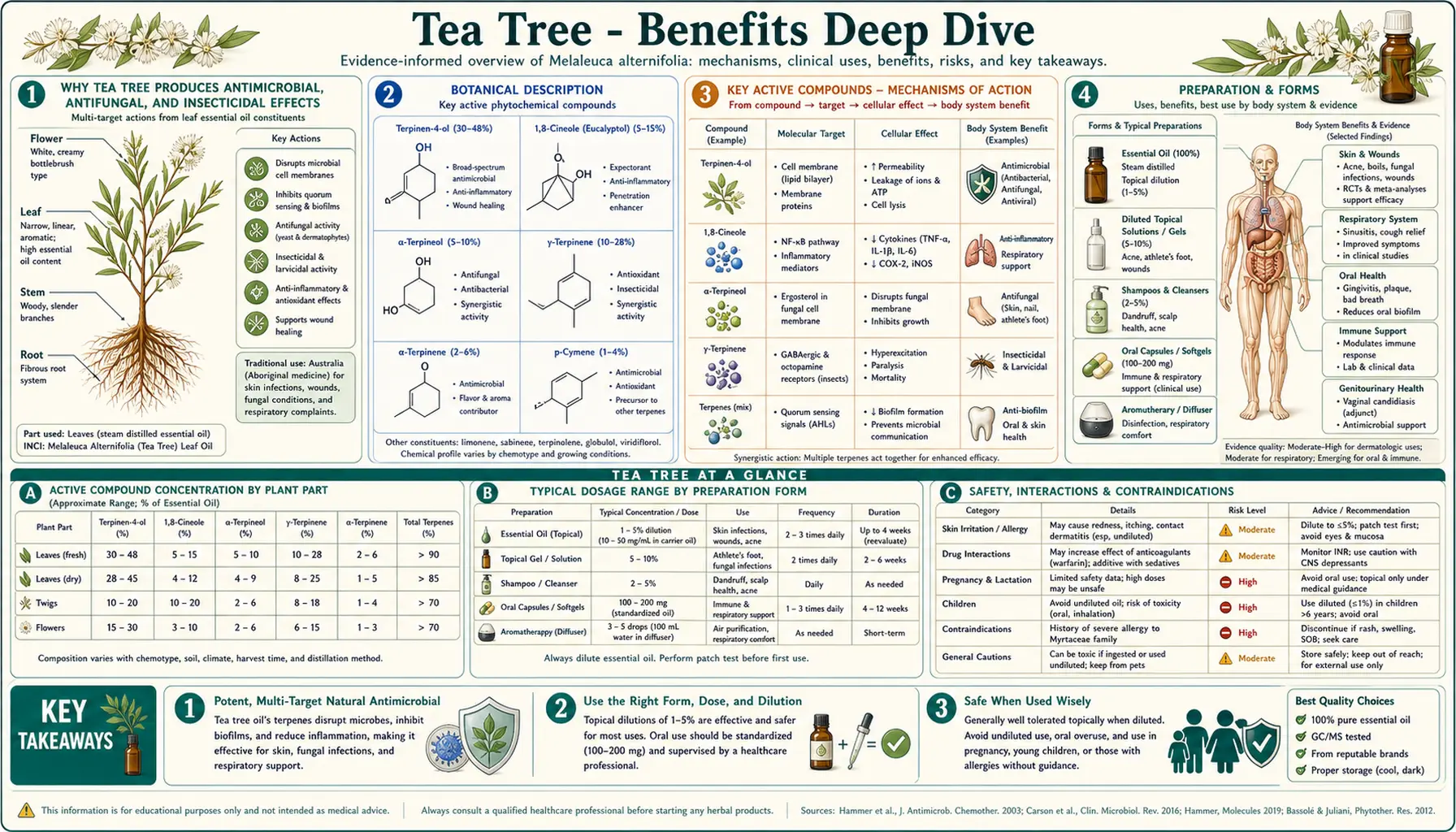
Tea tree oil is a complex mixture of approximately 100 distinct monoterpenes, sesquiterpenes, and their associated alcohols. The international standard ISO 4730 specifies the principal components and minimum/maximum percentages for an oil that can legally be labeled "tea tree oil" — an attempt to prevent the dilution and adulteration that plagued the early commercial industry. The three components that account for most of the biological activity are:
- Terpinen-4-ol (30–48%) — the principal antimicrobial constituent and the most-studied component. Terpinen-4-ol is a small lipophilic alcohol that intercalates into bacterial and fungal cell membranes, increasing membrane fluidity and disrupting the proton-motive force that drives ATP synthesis. It also inhibits respiration and depolarizes the membrane potential. Because the mechanism is purely biophysical — membrane disruption rather than enzyme inhibition — resistance is rare and difficult to evolve. Strains of MRSA, vancomycin-resistant Enterococcus (VRE), and multi-drug-resistant Pseudomonas aeruginosa remain susceptible. See the antimicrobial deep-dive for the full Carson 2006 review and MRSA decolonization data.
- Alpha-terpineol (1.5–8%) — structurally similar to terpinen-4-ol with comparable antimicrobial activity but slightly lower potency on a weight basis. Contributes to the oil's overall activity profile and to the characteristic camphor-like aroma.
- 1,8-cineole (eucalyptol, ≤15%) — the same compound that is the principal constituent of eucalyptus oil. Has its own antimicrobial activity but is also the primary skin irritant in tea tree oil — the ISO 4730 standard caps 1,8-cineole at 15% precisely because higher concentrations produce contact dermatitis. The lower the 1,8-cineole content (down to about 3% in premium oils), the better the topical tolerability without sacrificing antimicrobial effect.
This three-compound mechanism explains why tea tree has activity against such a broad target spectrum — gram-positive bacteria (including MRSA), gram-negative bacteria, yeasts (Candida albicans), filamentous fungi (Trichophyton species causing nail and skin infection), enveloped viruses (HSV-1, influenza), and arthropods (Pediculus humanus capitis head lice, Sarcoptes scabiei scabies mites). Cell membranes are the universal target, and almost every infectious agent has a membrane that monoterpenes can disrupt.
The therapeutic complications are also chemistry-driven. Oxidized tea tree oil — oil that has been exposed to air, light, or heat for prolonged periods — develops elevated concentrations of ascaridole, 1,2,4-trihydroxymenthane, and peroxides that are substantially more sensitizing than the parent oil. Old or improperly stored tea tree oil is the principal cause of allergic contact dermatitis. Fresh, properly stored oil (amber glass, cool dark storage, used within 12 months of opening) has a much lower sensitization rate. The other clinical caution — covered in detail on each sub-article — is that tea tree oil should never be ingested. Oral ingestion produces central nervous system depression, ataxia, coma, and in severe cases respiratory failure. There is no oral therapeutic use for tea tree oil; it is a topical-only agent.
Research Papers: Antimicrobial & MRSA
- Carson CF, Hammer KA, Riley TV (2006). Melaleuca alternifolia (Tea Tree) oil: a review of antimicrobial and other medicinal properties — the landmark review — PubMed: Carson 2006 review
- Carson CF, Mee BJ, Riley TV (2002). Mechanism of action of Melaleuca alternifolia (tea tree) oil on Staphylococcus aureus: membrane disruption — PubMed: Membrane mechanism
- Dryden MS et al. (2004). A randomized, controlled trial of tea tree topical preparations versus a standard topical regimen for the clearance of MRSA — PubMed: Dryden MRSA decolonization
- Caelli M et al. (2000). Tea tree oil as an alternative topical decolonization agent for MRSA — PubMed: Caelli MRSA
- Edmondson M et al. (2011). Tea tree oil and impetigo, infected wounds, and MRSA — PubMed: Wound infection
- May J et al. (2000). Time-kill studies of tea tree oils on clinical isolates — PubMed: Time-kill kinetics
- Hammer KA, Carson CF, Riley TV (2002). In vitro activity of Melaleuca alternifolia oil against dermatophytes and other filamentous fungi — PubMed: Dermatophyte activity
- Brady A et al. (2006). Tea tree oil inhibits viability and growth of methicillin-resistant Staphylococcus aureus biofilms — PubMed: MRSA biofilms
- Loughlin R et al. (2008). Comparison of the cidal activity of tea tree oil and terpinen-4-ol against clinical bacterial skin isolates — PubMed: Loughlin terpinen-4-ol
- Messager S et al. (2005). Effectiveness of hand-cleansing formulations containing tea tree oil — PubMed: Hand-cleansing
- LaPlante KL (2007). In vitro activity of lysostaphin, mupirocin, and tea tree oil against clinical MRSA isolates — PubMed: vs mupirocin in vitro
- Hammer KA et al. (2008). Frequencies of resistance to tea tree oil and antibiotic resistance — PubMed: Resistance frequencies
Research Papers: Acne
- Bassett IB, Pannowitz DL, Barnetson RS (1990). A comparative study of tea-tree oil versus benzoylperoxide in the treatment of acne — the landmark RCT — PubMed: Bassett 1990
- Enshaieh S et al. (2007). The efficacy of 5% topical tea tree oil gel in mild to moderate acne vulgaris: a randomized, double-blind, placebo-controlled study — PubMed: Enshaieh placebo-controlled
- Malhi HK et al. (2017). Tea tree oil gel for mild to moderate acne — an open-label uncontrolled efficacy trial — PubMed: Malhi gel trial
- Raman A et al. (1995). Antimicrobial effects of tea-tree oil and its major components on Propionibacterium acnes — PubMed: P. acnes activity
- Hammer KA (2015). Treatment of acne with tea tree oil (melaleuca) products: a review of efficacy, tolerability and potential modes of action — PubMed: Hammer 2015 review
- Najafi-Taher R et al. (2018). A topical gel of tea tree oil nanoemulsion containing adapalene versus adapalene marketed gel in patients with acne vulgaris — PubMed: Tea tree + adapalene nanoemulsion
Research Papers: Antifungal & Nail Fungus
- Buck DS, Nidorf DM, Addino JG (1994). Comparison of two topical preparations for the treatment of onychomycosis: Melaleuca alternifolia (tea tree) oil and clotrimazole — the foundational nail fungus trial — PubMed: Buck 1994
- Tong MM, Altman PM, Barnetson RS (1992). Tea tree oil in the treatment of tinea pedis — PubMed: Tong tinea pedis
- Satchell AC et al. (2002). Treatment of interdigital tinea pedis with 25% and 50% tea tree oil solution: a randomized, placebo-controlled, blinded study — PubMed: Satchell tinea pedis
- Satchell AC et al. (2002). Treatment of oral candidiasis with topical Melaleuca alternifolia (tea tree) oil gel — PubMed: Oral candidiasis
- Hammer KA, Carson CF, Riley TV (2003). Antifungal activity of the components of Melaleuca alternifolia (tea tree) oil — PubMed: Component antifungal activity
- Mertas A et al. (2015). The influence of tea tree oil on fluconazole activity against fluconazole-resistant Candida albicans — PubMed: Fluconazole synergy
- Nenoff P et al. (1996). Antifungal activity of the essential oil of Melaleuca alternifolia against pathogenic fungi in vitro — PubMed: Nenoff in vitro
- Concha JM, Moore LS, Holloway WJ (1998). 5% Melaleuca oil cream for tinea pedis: comparative trial — PubMed: Concha 5% cream
Research Papers: Head Lice & Scabies
- Barker SC, Altman PM (2010). A randomised, assessor blind, parallel group comparative efficacy trial of three products for the treatment of head lice in children — melaleuca oil and lavender oil, pyrethrins and piperonyl butoxide, and a "suffocation" product — PubMed: Barker 2010 head lice
- Barker SC, Altman PM (2011). An ex vivo, assessor blind, randomised, parallel group, comparative efficacy trial of the ovicidal activity of three head lice treatments — PubMed: Barker ovicidal ex vivo
- Walton SF, McKinnon M, Pizzutto S, et al. (2004). Acaricidal activity of Melaleuca alternifolia (tea tree) oil: in vitro sensitivity of Sarcoptes scabiei var hominis to terpinen-4-ol — PubMed: Walton scabies in vitro
- Mills C, Cleary BJ, Gilmer JF, Walsh JJ (2004). Inhibition of acetylcholinesterase by tea tree oil — insecticidal mechanism — PubMed: AChE mechanism
- Williamson EM et al. (2007). The activity of tea-tree oil and lavender oil on head-lice — PubMed: Williamson tea tree/lavender
- Thomas J et al. (2016). Head lice: a review of clinical features, treatment, and emerging pediculicide resistance — PubMed: Pediculicide resistance review
- Pasay C et al. (2010). Acaricidal activity of eugenol based compounds and tea tree oil against permethrin-resistant head lice and scabies mites — PubMed: Permethrin-resistant lice
- Greive KA, Barnes TM (2018). The efficacy of Australian essential oils for the treatment of head lice — PubMed: Australian essential oils review
Research Papers: Cross-Cutting (Chemistry, Safety, Toxicity)
- ISO 4730:2017 international standard for Melaleuca alternifolia (tea tree) oil chemical composition — PubMed: ISO 4730 chemistry
- Hammer KA, Carson CF, Riley TV, Nielsen JB (2006). A review of the toxicity of Melaleuca alternifolia (tea tree) oil — PubMed: Toxicity review
- Henley DV, Lipson N, Korach KS, Bloch CA (2007). Prepubertal gynecomastia linked to lavender and tea tree oils — NEJM case series — PubMed: Henley NEJM 2007
- Hammer KA et al. (2012). Tea tree oil and gynecomastia: re-examination of the evidence — PubMed: Gynecomastia re-examination
- Morris MC, Donoghue A, Markowitz JA, Osterhoudt KC (2003). Ingestion of tea tree oil by a 4-year-old boy: acute toxicity case report — PubMed: Pediatric ingestion
- Jacobs MR, Hornfeldt CS (1994). Melaleuca oil poisoning — clinical and animal toxicology — PubMed: Jacobs poisoning
- Hausen BM, Reichling J, Harkenthal M (1999). Degradation products of monoterpenes are the sensitizing agents in tea tree oil — PubMed: Oxidation and sensitization
- Larson D, Jacob SE (2012). Tea tree oil — allergic contact dermatitis review — PubMed: Contact dermatitis
- Christoffers WA et al. (2014). Patch testing with tea tree oil — oxidized vs unoxidized — PubMed: Oxidation patch test
- Carson CF, Riley TV (1995). Antimicrobial activity of the major components of the essential oil of Melaleuca alternifolia — PubMed: Component activity
External Authoritative Resources
- NCCIH (NIH) — Tea Tree Oil Fact Sheet — the US National Center for Complementary and Integrative Health overview
- MedlinePlus / NIH — Tea Tree Oil — clinical evidence ratings by condition
- ISO 4730:2017 — Essential Oil of Melaleuca, terpinen-4-ol type (tea tree oil) — the international compositional standard
- Australian Tea Tree Industry Association — producer and research consortium
- PubMed — All research on Melaleuca alternifolia / tea tree oil (~2,500+ papers)
Connections
- Tea Tree (Main Page)
- Tea Tree for Antimicrobial & MRSA
- Tea Tree for Acne
- Tea Tree for Antifungal & Nail Fungus
- Tea Tree for Head Lice & Scabies
- All Herbs
- Antibacterial Herbs
- Eucalyptus (1,8-cineole)
- Oregano
- Thyme
- Lavender
- Manuka Honey
- Neem
- Olive Leaf
- Acne
- Fungal Infections
- Eczema
- Staphylococcus aureus (MRSA)
- Pseudomonas aeruginosa
- Cellulitis
- Silver Nanoparticles