Tea Tree Oil for Antimicrobial Use & MRSA
Tea tree oil is one of the most extensively-studied botanical antimicrobials in the peer-reviewed literature. The Carson, Hammer & Riley 2006 Clinical Microbiology Reviews paper — an exhaustive 50-page review — documented in vitro activity against more than 60 distinct bacterial and fungal species, including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus, multi-drug-resistant Pseudomonas aeruginosa, and clinical strains of Candida albicans that had developed azole resistance. The principal antimicrobial constituent is terpinen-4-ol (30–48% of the oil), which disrupts microbial cell membranes through a biophysical mechanism that is exceptionally difficult for resistant strains to evade. The standardized topical concentration is 5%, embedded in a gel, cream, or carrier oil, applied to intact skin or to the anterior nares for MRSA decolonization. Multiple controlled hospital trials have compared 5% tea tree preparations to standard mupirocin nasal ointment for MRSA decolonization with comparable efficacy and a lower rate of antibiotic-resistance emergence over time.
Table of Contents
- The Carson 2006 Landmark Review
- Terpinen-4-ol and the Membrane-Disruption Mechanism
- Why MRSA Created the Modern Tea Tree Renaissance
- MRSA Decolonization Trials (Caelli, Dryden)
- Hospital Infection Control Applications
- The 5% Topical Concentration Standard
- Biofilm Activity and Wound Care
- Why Resistance Is Rare
- Practical Topical Use
- Cautions (Never Ingest, Oxidation, Contact Dermatitis)
- Key Research Papers
- Connections
- Featured Videos
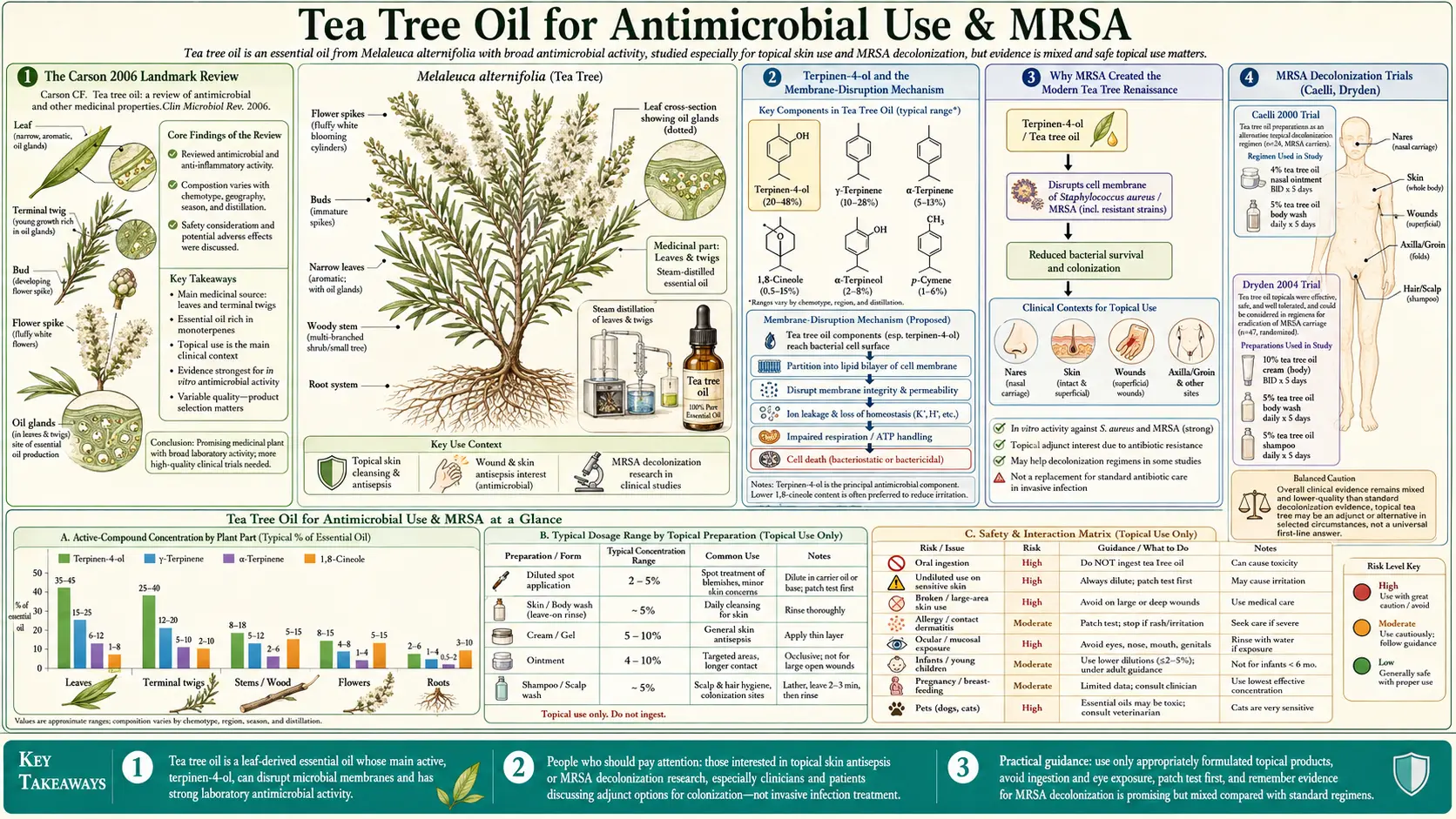
The Carson 2006 Landmark Review
The single most-cited paper on tea tree oil is the 2006 Clinical Microbiology Reviews review by Christine Carson, Katherine Hammer, and Thomas Riley — three microbiologists at the University of Western Australia who have spent careers studying the oil's pharmacology and microbiology. The review compiled essentially every published study on tea tree oil through 2005 into one comprehensive document, with a particular focus on antimicrobial spectrum, mechanism of action, clinical efficacy, and toxicity.
The headline findings:
- Documented in vitro inhibitory activity against more than 60 distinct bacterial species, including all clinically important gram-positive cocci (Staphylococcus, Streptococcus, Enterococcus), most gram-negative rods (E. coli, Klebsiella, Pseudomonas), anaerobes (Bacteroides), and acid-fast organisms (Mycobacterium smegmatis)
- Documented antifungal activity against dermatophytes (Trichophyton, Microsporum, Epidermophyton), yeasts (Candida, Malassezia), and filamentous fungi (Aspergillus)
- Documented antiviral activity against enveloped viruses including HSV-1, HSV-2, and influenza A
- Minimum inhibitory concentrations (MIC) typically in the 0.25–2% range for susceptible bacteria, well below the 5% concentration used in commercial topical products
- Synergy with conventional antibiotics in several combinations, particularly with vancomycin against MRSA
- An anti-inflammatory effect separate from the antimicrobial activity, mediated by suppression of histamine release and reduction of TNF-alpha and IL-1 production by activated monocytes
The review remains the standard reference. Subsequent research has filled in mechanistic details (membrane fluidity disruption confirmed by NMR, biofilm activity confirmed in flow cell models) but has not overturned any of the major findings. Anyone evaluating tea tree oil for serious clinical use should read the original Carson 2006 paper.
Terpinen-4-ol and the Membrane-Disruption Mechanism
The principal antimicrobial constituent of tea tree oil is terpinen-4-ol, a small lipophilic alcohol that accounts for 30–48% of the oil by ISO 4730 standard. Mechanistic studies by Carson and colleagues, and independently by groups in Italy and Germany, have established the membrane-disruption mechanism through several converging lines of evidence:
- Loss of intracellular potassium — treated bacteria release potassium ions, indicating direct membrane permeabilization. This happens within minutes of tea tree exposure and is dose-dependent
- Collapse of the proton-motive force — the electrochemical gradient across the bacterial inner membrane is required for ATP synthesis. Tea tree oil treatment dissipates this gradient, halting energy production
- Increased membrane fluidity — NMR studies show that terpinen-4-ol intercalates between membrane phospholipids and increases the rotational mobility of the lipid acyl chains, exactly as expected for a small lipophilic disruptor
- Inhibition of respiration — oxygen consumption by treated bacteria drops sharply, consistent with electron transport chain dysfunction secondary to membrane integrity loss
- Cell lysis at higher concentrations — at concentrations above the minimum bactericidal concentration, bacteria release cytoplasmic contents and become non-viable
The clinical significance of this mechanism is that it is fundamentally different from how conventional antibiotics work. Beta-lactams inhibit cell wall synthesis. Aminoglycosides inhibit ribosomes. Fluoroquinolones inhibit DNA gyrase. Each of these is a single-target inhibitor that bacteria can evade through a single mutation (PBP changes for beta-lactams, ribosomal modifications for aminoglycosides, gyrase mutations for fluoroquinolones). Tea tree oil's membrane disruption mechanism has no single target to mutate around — the bacterium would have to reinvent its membrane chemistry, which is essentially impossible without catastrophic loss of viability. This is why MRSA, which is resistant to nearly every beta-lactam antibiotic available, remains fully susceptible to tea tree oil.
Why MRSA Created the Modern Tea Tree Renaissance
Tea tree oil had a long history of folk and commercial use in Australia (particularly during World War II, when it was issued in soldier first-aid kits in the Pacific theater), but it largely fell out of mainstream medical use after the introduction of antibiotics in the late 1940s. The renaissance of clinical interest in tea tree oil dates to the late 1990s and is directly attributable to the emergence of methicillin-resistant Staphylococcus aureus as a major nosocomial pathogen.
By the mid-1990s, MRSA was the dominant cause of hospital-acquired skin and soft-tissue infection in most developed countries. Mupirocin nasal ointment was the standard agent for MRSA decolonization — eradication of nasal carriage in patients colonized but not infected, a step that demonstrably reduces subsequent surgical site infection and bloodstream infection in carriers. However, mupirocin resistance emerged within years of widespread use. By the early 2000s, hospitals were seeing mupirocin failure rates of 10–30% in MRSA decolonization protocols, and the resistance was spreading.
Australian researchers, with the long-established commercial tea tree industry providing standardized oil for study, began investigating tea tree as an alternative to mupirocin. The MIC data looked promising — tea tree oil was bactericidal against all tested MRSA isolates at concentrations far below its tolerable topical concentration. The mechanism argued for low resistance potential. And the cost was a fraction of mupirocin. A series of controlled trials followed.
MRSA Decolonization Trials (Caelli, Dryden)
The two pivotal early decolonization trials were Caelli et al. 2000 and Dryden et al. 2004:
Caelli 2000 randomized 30 MRSA-colonized hospitalized patients to either a standard regimen (2% mupirocin nasal ointment plus triclosan body wash) or a tea tree regimen (4% tea tree nasal ointment plus 5% tea tree body wash). Decolonization rates were 33% with mupirocin/triclosan vs 41% with tea tree — numerically favoring tea tree but underpowered for definitive comparison. Importantly, no patient receiving tea tree developed adverse reactions requiring discontinuation, and the cost was approximately one-quarter of the mupirocin regimen.
Dryden 2004 was a larger and better-powered trial: 224 MRSA-colonized hospitalized patients randomized to mupirocin nasal ointment plus chlorhexidine body wash vs 10% tea tree nasal cream plus 5% tea tree body wash. The primary outcome was clearance of MRSA at all body sites at 48 hours after completion of the 5-day regimen. Results: 49% clearance with the conventional regimen vs 41% clearance with tea tree. The difference was not statistically significant. Subgroup analysis suggested that tea tree was actually superior for skin site clearance but inferior for nasal clearance (where the cream formulation was harder to apply effectively than mupirocin ointment).
The Dryden trial established that tea tree was non-inferior to mupirocin for the overall decolonization task and is now incorporated into MRSA management guidelines in several UK and Australian hospital networks, particularly for patients with documented mupirocin-resistant MRSA. The Edmondson 2011 follow-up examined tea tree in active infection (impetigo, infected wounds, MRSA-colonized chronic wounds) and found good clinical response rates.
Hospital Infection Control Applications
Beyond MRSA decolonization, tea tree oil has been studied in several hospital infection control contexts:
- Hand hygiene — Messager 2005 evaluated tea tree-containing hand washes against artificially-contaminated volunteer hands and showed efficacy comparable to a 4% chlorhexidine wash for reducing transient organism counts. The tea tree formulation was better tolerated with less dermatitis on repeat use, an important consideration for healthcare workers who wash hands dozens of times per shift
- Pre-operative skin preparation — smaller studies have used tea tree-containing washes as preoperative skin preparation, with documented reduction in skin flora counts comparable to standard chlorhexidine. Tea tree is not yet incorporated into mainstream surgical-site-infection prevention guidelines but remains an active area of investigation
- Vascular catheter site care — small studies have used tea tree-containing dressings around central venous catheter exit sites, with reduction in colonization rates. Larger trials would be needed before this enters guidelines
- Wound care — tea tree-containing dressings have been studied for chronic ulcers, particularly diabetic foot ulcers and venous stasis ulcers, with documented improvement in bioburden and healing rates. The biofilm activity discussed below is particularly relevant in this setting
- Hospital cleaning — tea tree-containing surface disinfectants have shown bactericidal activity against hospital surface contamination at concentrations of 5–10%, though typical hospital cleaning protocols still rely on bleach or quaternary ammonium compounds for cost and standardization reasons
For broader context on MRSA and Staphylococcus management, see our Staphylococcus aureus page. For other natural antimicrobials with similar applications, see Manuka Honey (which has its own substantial MRSA literature) and Silver Nanoparticles.
The 5% Topical Concentration Standard
The most-studied topical concentration of tea tree oil is 5% in a gel, cream, or carrier oil base. This concentration emerged from the antimicrobial efficacy and tolerability data:
- Antimicrobial efficacy — the MIC against MRSA and most clinically important bacteria is 0.25–2% tea tree oil. The bactericidal concentration (MBC) is typically 2× the MIC. A 5% preparation therefore provides 2.5× to 20× the killing concentration at the application site, with adequate margin for dilution by skin moisture and inter-individual variation in skin chemistry
- Skin tolerability — controlled tolerability studies have shown that 5% preparations produce minimal irritation in the majority of users. Concentrations of 10% and above show progressively higher rates of stinging, redness, and contact dermatitis. Concentrations of 25% and above produce substantial discomfort in most users (the high-concentration studies in nail fungus, discussed on the antifungal page, accept this tradeoff because the nail itself is keratinized and not innervated)
- Cost — tea tree oil is comparatively inexpensive (approximately $0.50–$2 per mL for pharmaceutical-grade oil at retail), so a 5% preparation in a carrier base remains affordable. There is no economic pressure to use lower concentrations
Available commercial 5% preparations include Thursday Plantation Tea Tree Gel, Desert Essence Tea Tree Oil Gel, and various house-brand products from major drugstore chains. Compounding pharmacies can prepare custom-concentration tea tree creams when needed.
Biofilm Activity and Wound Care
One particularly clinically important property of tea tree oil is activity against bacterial biofilms. Biofilms are sessile, matrix-encased bacterial communities that form on surfaces (medical devices, chronic wound beds, the airways of cystic fibrosis patients) and exhibit 100–1000-fold reduced susceptibility to conventional antibiotics compared to planktonic bacteria of the same species. The biofilm matrix physically excludes antibiotics, the slow-growing biofilm bacteria are metabolically less vulnerable to most antibiotic mechanisms, and persister cells within biofilms survive even prolonged antibiotic exposure.
Brady et al. 2006 examined tea tree activity against established MRSA biofilms in vitro and showed concentration-dependent biofilm disruption at 5% tea tree concentrations — concentrations achievable in topical wound preparations. The mechanism is twofold: terpinen-4-ol penetrates the biofilm matrix more effectively than larger antibiotic molecules, and the membrane-disruption mechanism does not require active bacterial metabolism (so the slow-growing biofilm bacteria remain susceptible).
The clinical translation is the use of tea tree-containing wound dressings for chronic wounds, particularly diabetic foot ulcers, venous stasis ulcers, and pressure injuries with biofilm involvement. Small clinical trials have shown improved healing trajectories. Tea tree is not yet incorporated into mainstream wound care guidelines but is increasingly used in specialty wound centers, often in combination with conventional antimicrobial dressings.
Why Resistance Is Rare
One of the most reassuring features of tea tree oil from an antimicrobial stewardship perspective is the extreme rarity of clinically meaningful resistance. Hammer et al. 2008 conducted serial-passage experiments — growing bacteria in subinhibitory concentrations of tea tree oil and serially passaging to attempt to select for resistant mutants. After dozens of passages, MIC increases were modest (typically 2–4 fold) and the resistant strains showed substantial fitness costs — slower growth, lower competitive ability, and reversion to parental susceptibility within several generations in tea-tree-free medium.
The mechanistic explanation: bacterial cell membranes have been evolutionarily optimized over billions of years for stability and barrier function. Any mutation that would resist terpinen-4-ol intercalation also tends to compromise normal membrane function. There is no "free lunch" mutation that confers tea tree resistance without fitness penalty. This is fundamentally different from antibiotic resistance, where bypass mutations (efflux pumps, modifying enzymes, target alterations) can be acquired with relatively small fitness cost.
The practical implication: tea tree oil can be used repeatedly in the same patient (chronic acne, recurrent nail fungus, MRSA decolonization in carriers) without the resistance accumulation that limits long-term mupirocin or antibiotic use. This is particularly valuable for patients who are chronic MRSA carriers and require repeat decolonization courses over years.
Practical Topical Use
For the patient or family considering tea tree oil for an antimicrobial purpose, the practical guidelines are:
- Use a 5% preparation for routine topical antimicrobial use on intact or minimally compromised skin. Either purchase a commercial 5% gel/cream, or dilute 100% tea tree oil (5 mL) into 95 mL of a carrier oil (jojoba, sweet almond, fractionated coconut)
- Patch test before regular use — apply a small amount to the inner forearm and wait 24 hours before broader application. Discontinue if redness, itching, or stinging persists beyond a few minutes of initial application
- Use fresh, properly stored oil — oxidized tea tree oil is substantially more sensitizing than fresh oil. Buy small bottles, store in amber glass in a cool dark place, replace bottles within 12–18 months of opening
- Avoid mucous membranes — tea tree oil should not be applied to the eyes, the mouth, or the genitalia in concentrated form. For oral or genital infection management, work with a clinician who can advise on appropriate dilution and formulation
- For MRSA decolonization — if you or a family member is a known MRSA carrier and your physician is open to alternatives to mupirocin, the Dryden 2004 protocol of 10% tea tree nasal cream plus 5% tea tree body wash twice daily for 5 days is the best-studied regimen
- Combine with hand hygiene — tea tree is not a substitute for soap-and-water hand hygiene. It is an adjunct, particularly in healthcare workers and household contacts of MRSA carriers
Cautions (Never Ingest, Oxidation, Contact Dermatitis)
- NEVER ingest tea tree oil — this is the single most important caution. Oral ingestion of tea tree oil produces dose-dependent central nervous system depression, ataxia, vomiting, hallucination, coma, and in severe cases respiratory failure. Pediatric ingestion cases (Morris 2003, Jacobs 1994) have required intensive care. There is no oral therapeutic use for tea tree oil; it is a topical-only agent. Keep tea tree oil out of reach of children
- Pre-pubertal boys — controversial gynecomastia association — Henley et al. 2007 NEJM reported three pre-pubertal boys who developed gynecomastia (breast tissue growth) that resolved on discontinuation of topical lavender-and-tea-tree products. The proposed mechanism was endocrine disruption with weak estrogenic and anti-androgenic activity in vitro. Subsequent re-examination (Hammer 2012) has called the causal attribution into question — tea tree oil shows no estrogenic activity in standardized assays, and the original cases involved combined lavender/tea tree exposure. The current cautious recommendation is to avoid prolonged topical use of tea tree oil on pre-pubertal boys until the question is definitively resolved
- Allergic contact dermatitis — tea tree oil is the most common essential oil cause of allergic contact dermatitis in patch test referrals. The principal sensitizers are oxidation products (ascaridole, 1,2,4-trihydroxymenthane, peroxides) rather than the parent monoterpenes. Fresh oil sensitization rates are low (under 2% in patch test populations); oxidized oil sensitization rates are substantially higher. Patients with confirmed tea tree oil contact dermatitis should avoid the oil entirely
- Drug interactions — topical tea tree oil has minimal systemic absorption and few documented drug interactions. Patients with severely compromised skin (extensive burn, ulceration) may absorb enough oil to produce mild systemic effects and should use lower concentrations under medical supervision
- Pregnancy and breastfeeding — topical use at standard 5% concentrations on intact skin is generally considered acceptable, but data are limited. Avoid application to the nipple area during breastfeeding to prevent infant ingestion
- Pet safety — tea tree oil is significantly more toxic to cats and dogs than to humans. Even dilute topical application to pets has produced ataxia, hypothermia, depression, and death in cats. Do not use tea tree oil on or around pets
Key Research Papers
- Carson CF, Hammer KA, Riley TV (2006). Melaleuca alternifolia (Tea Tree) oil: a review of antimicrobial and other medicinal properties. Clinical Microbiology Reviews. — PubMed
- Carson CF, Mee BJ, Riley TV (2002). Mechanism of action of Melaleuca alternifolia (tea tree) oil on Staphylococcus aureus. Antimicrobial Agents and Chemotherapy. — PubMed
- Caelli M, Porteous J, Carson CF, Heller R, Riley TV (2000). Tea tree oil as an alternative topical decolonization agent for methicillin-resistant Staphylococcus aureus. Journal of Hospital Infection. — PubMed
- Dryden MS, Dailly S, Crouch M (2004). A randomized, controlled trial of tea tree topical preparations versus a standard topical regimen for the clearance of MRSA colonization. Journal of Hospital Infection. — PubMed
- Edmondson M, Newall N, Carville K, Smith J, Riley TV, Carson CF (2011). Uncontrolled, open-label, pilot study of tea tree oil solution in the decolonisation of MRSA-positive wounds and its influence on wound healing. International Wound Journal. — PubMed
- Brady A, Loughlin R, Gilpin D, Kearney P, Tunney M (2006). In vitro activity of tea-tree oil against clinical skin isolates of methicillin-resistant and -sensitive Staphylococcus aureus and coagulase-negative staphylococci. Journal of Medical Microbiology. — PubMed
- Hammer KA, Carson CF, Riley TV (2012). Effects of Melaleuca alternifolia (tea tree) essential oil and the major monoterpene component terpinen-4-ol on the development of single- and multistep antibiotic resistance and antimicrobial susceptibility. Antimicrobial Agents and Chemotherapy. — PubMed
- Loughlin R, Gilmore BF, McCarron PA, Tunney MM (2008). Comparison of the cidal activity of tea tree oil and terpinen-4-ol against clinical bacterial skin isolates and human fibroblast cells. Letters in Applied Microbiology. — PubMed
- Messager S, Hammer KA, Carson CF, Riley TV (2005). Effectiveness of hand-cleansing formulations containing tea tree oil assessed ex vivo on human skin and in vivo with volunteers using European standard EN 1499. Journal of Hospital Infection. — PubMed
- LaPlante KL (2007). In vitro activity of lysostaphin, mupirocin, and tea tree oil against clinical methicillin-resistant Staphylococcus aureus. Diagnostic Microbiology and Infectious Disease. — PubMed
- Hammer KA, Carson CF, Riley TV, Nielsen JB (2006). A review of the toxicity of Melaleuca alternifolia (tea tree) oil. Food and Chemical Toxicology. — PubMed
- Henley DV, Lipson N, Korach KS, Bloch CA (2007). Prepubertal gynecomastia linked to lavender and tea tree oils. New England Journal of Medicine. — PubMed
PubMed Topic Searches
- PubMed: Tea tree oil and MRSA
- PubMed: Terpinen-4-ol antimicrobial mechanism
- PubMed: Melaleuca decolonization protocols
- PubMed: Tea tree biofilm/wound
- PubMed: Contact dermatitis & oxidation
Connections
- Tea Tree Overview
- Tea Tree Benefits Hub
- Tea Tree for Acne
- Tea Tree for Nail Fungus
- Tea Tree for Head Lice
- Antibacterial Herbs
- Manuka Honey (MRSA)
- Oregano (Carvacrol)
- Thyme (Thymol)
- Garlic (Allicin)
- Olive Leaf (Oleuropein)
- Silver Nanoparticles
- Staphylococcus aureus (MRSA)
- Pseudomonas aeruginosa
- Cellulitis
- All Herbs