Fungal Infections
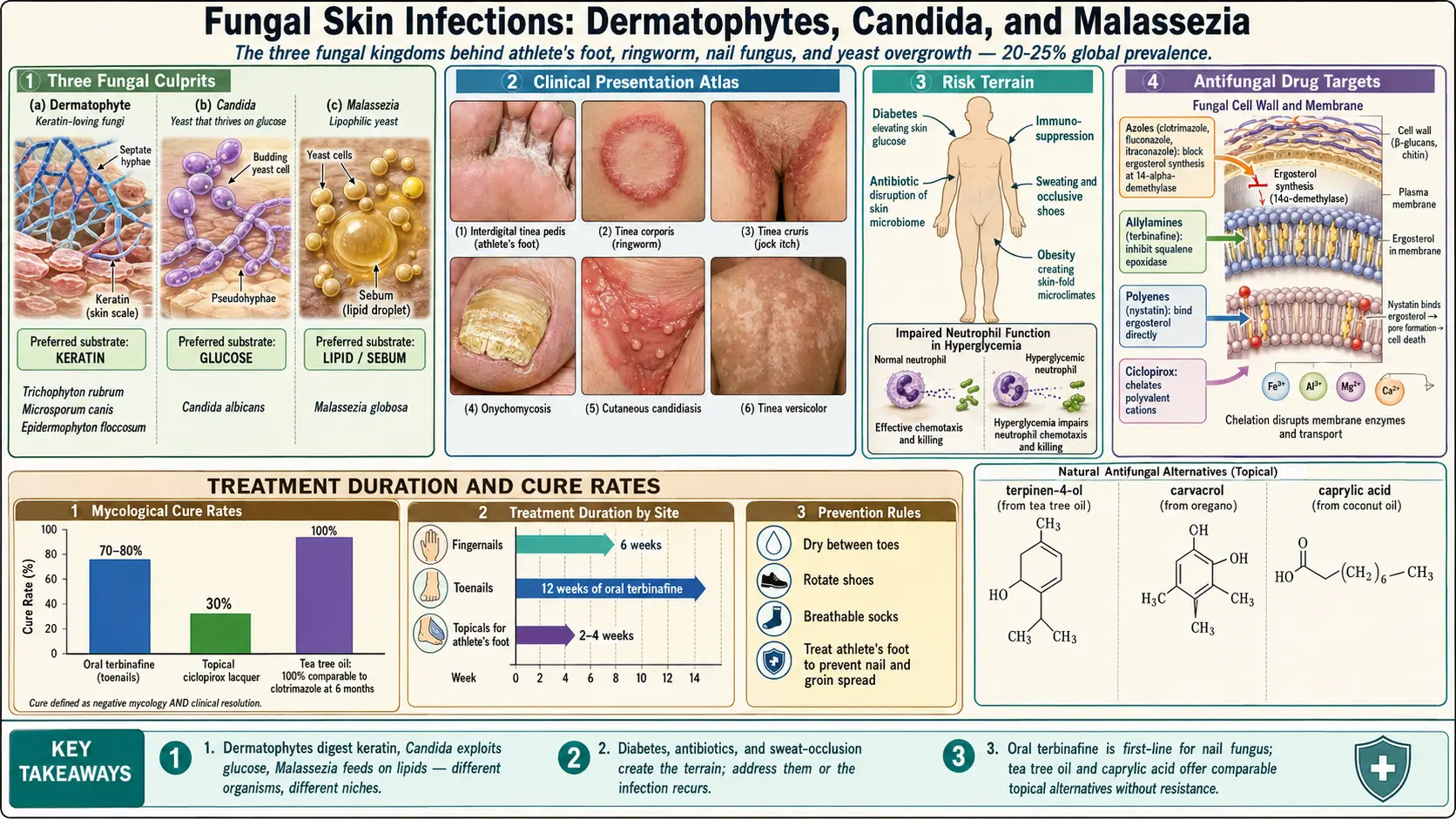
Table of Contents
- Overview of Fungal Skin Infections
- Types of Fungal Infections
- Causes and Organisms
- Risk Factors
- Symptoms by Type
- Conventional Treatments
- Natural Antifungal Approaches
- Candida Overgrowth and Systemic Connection
- Biofilm Disruption
- Anti-Fungal Diet
- Immune Support
- Prevention Strategies
- Cautions and Considerations
- References & Research
- Featured Videos
Overview of Fungal Skin Infections
Fungal skin infections (dermatomycoses) are among the most common infections worldwide, affecting an estimated 20-25% of the global population at any given time. These infections range from superficial, easily treated conditions to chronic, recurrent problems that significantly impact quality of life.
From a naturopathic perspective, fungal skin infections are not simply a matter of exposure to a pathogenic organism. They reflect an imbalance in the body's terrain — the internal environment that either supports or resists infection. Factors including immune function, blood sugar regulation, gut health, microbiome composition, and nutritional status all determine whether exposure to a fungal organism results in active infection.
While topical antifungal medications can address the surface infection, lasting resolution often requires addressing the underlying conditions that allowed the infection to take hold. This is particularly true for chronic or recurrent fungal infections, where the conventional approach of repeated antifungal courses fails to address the root cause.
Types of Fungal Infections
Athlete's Foot (Tinea Pedis)
Tinea pedis is the most common fungal infection, affecting up to 15-25% of the population. It typically begins between the toes and can spread to the soles and sides of the feet. Three clinical presentations exist:
- Interdigital — The most common form, with scaling, maceration, and fissuring between the toes, particularly the fourth and fifth toes
- Moccasin type — Chronic, dry, scaling infection covering the sole and sides of the foot in a "moccasin" distribution. Often caused by Trichophyton rubrum and can be difficult to eradicate.
- Vesicular (inflammatory) — Characterized by blisters and vesicles, typically on the instep. Often caused by Trichophyton mentagrophytes.
Ringworm (Tinea Corporis)
Tinea corporis is a fungal infection of the body skin that produces the characteristic ring-shaped lesion — a circular patch with a raised, scaly, red border and clearing in the center. Despite its name, no worm is involved. Ringworm is highly contagious and can be spread through direct skin contact, contaminated objects (fomites), and contact with infected animals, particularly cats and dogs.
Jock Itch (Tinea Cruris)
Tinea cruris affects the groin, inner thighs, and buttocks. It presents as a red, itchy rash with a well-defined, raised border that extends outward from the groin fold. It is more common in males and in warm, humid climates. Jock itch is frequently associated with concurrent athlete's foot, as the same organism infects both areas and can be spread by touching the feet and then the groin.
Nail Fungus (Onychomycosis)
Onychomycosis is a fungal infection of the nails that affects approximately 10% of the general population and up to 50% of adults over age 70. It causes the nail to become thickened, discolored (yellow, brown, or white), brittle, and sometimes painful. Toenails are affected far more frequently than fingernails. Onychomycosis is notoriously difficult to treat because the nail plate protects the fungus from topical medications, and the slow rate of nail growth means treatment must continue for months (6-12 months for toenails).
Candida Skin Infections (Cutaneous Candidiasis)
Candida skin infections occur in warm, moist areas of the body — skin folds (under the breasts, abdominal folds, groin), diaper area in infants, and corners of the mouth (angular cheilitis). They present as bright red, moist patches with satellite pustules at the borders. Candida infections are distinct from dermatophyte infections and are particularly common in individuals with diabetes, obesity, or who take antibiotics or immunosuppressive medications.
Tinea Versicolor (Pityriasis Versicolor)
Tinea versicolor is caused by overgrowth of Malassezia yeast, a commensal organism that normally lives on human skin. It produces patches of skin that are lighter or darker than the surrounding area, typically on the trunk, shoulders, and upper arms. The patches may be slightly scaly and can be pink, tan, brown, or white. The color change results from Malassezia producing azelaic acid, which inhibits melanin production. Tinea versicolor is not contagious and tends to recur in warm, humid conditions.
Causes and Organisms
Three main groups of fungi cause skin infections:
Dermatophytes
Dermatophytes are a group of closely related fungi that have evolved to digest keratin, the structural protein in skin, hair, and nails. They are responsible for the "tinea" infections (athlete's foot, ringworm, jock itch, nail fungus, scalp ringworm). The three genera of dermatophytes are:
- Trichophyton — The most common cause of fungal skin infections. T. rubrum causes the majority of athlete's foot, jock itch, and nail fungus. T. mentagrophytes causes inflammatory tinea.
- Microsporum — Commonly causes scalp ringworm (tinea capitis), particularly in children. M. canis is frequently transmitted from cats and dogs.
- Epidermophyton — E. floccosum causes jock itch and athlete's foot but does not infect hair or nails.
Candida
Candida is a genus of yeasts that normally inhabit the gastrointestinal tract, mouth, and vaginal area. Candida albicans is the most common species causing skin infections, though non-albicans species such as C. glabrata, C. tropicalis, and C. parapsilosis are increasingly recognized. Candida causes infection when the normal balance of microorganisms is disrupted or when the immune system is compromised.
Malassezia
Malassezia is a lipophilic (fat-loving) yeast that is part of the normal skin flora. It requires lipids for growth and thrives in sebum-rich areas. Malassezia globosa and M. furfur are the primary species involved in tinea versicolor and Malassezia folliculitis (fungal acne). Overgrowth occurs when conditions favor the yeast — high humidity, excess sebum, and immunosuppression.
Risk Factors
Understanding risk factors is essential for both treatment and prevention of fungal infections.
Environmental Factors
- Warmth and moisture — Fungi thrive in warm, damp environments. Sweating, occlusive footwear, tight clothing, and humid climates all increase risk.
- Communal areas — Locker rooms, swimming pools, shared showers, and gyms are common sources of dermatophyte exposure
- Contaminated objects — Towels, shoes, socks, and clothing can harbor fungal spores
Immune Suppression
- HIV/AIDS and other immunodeficiency conditions
- Immunosuppressive medications (corticosteroids, chemotherapy, biologics)
- Chronic stress — Suppresses immune surveillance and increases susceptibility
- Nutrient deficiencies — Particularly zinc, vitamin D, vitamin A, and iron
Antibiotic Use
Antibiotics disrupt the normal microbiome, killing beneficial bacteria that compete with fungi for resources and produce natural antifungal compounds. This creates ecological space for fungal overgrowth. Broad-spectrum and prolonged antibiotic courses pose the greatest risk. This is one of the most common precipitating factors for Candida infections.
Diabetes and Blood Sugar
Diabetes mellitus significantly increases the risk of all fungal infections. Elevated blood glucose provides a ready food source for fungi, impairs white blood cell function (particularly neutrophil activity), and damages blood vessel integrity, reducing delivery of immune cells to infected tissues. Even pre-diabetes and insulin resistance increase fungal infection risk.
Other Risk Factors
- Obesity — Creates skin folds with warmth and moisture, ideal for Candida
- Peripheral vascular disease — Poor circulation to extremities, particularly relevant for nail fungus
- Advancing age — Reduced immune function, slower nail growth, and increased prevalence of diabetes
- Hyperhidrosis (excessive sweating) — Creates persistently moist conditions
Symptoms by Type
Athlete's Foot
- Itching, burning, and stinging between the toes or on the soles
- Peeling, cracking, and scaling skin
- Redness and inflammation
- Blisters that ooze or crust (vesicular type)
- Dry, chronic scaling on the soles (moccasin type)
- Unpleasant odor in severe cases
Ringworm
- Circular or ring-shaped red patches with raised, scaly borders
- Central clearing as the ring expands outward
- Itching and irritation
- Multiple rings that may overlap
- Possible blister formation at the advancing edge
Jock Itch
- Red, itchy rash in the groin folds, extending to the inner thighs
- Well-defined, raised border that may have small vesicles
- Burning and chafing sensation
- Typically spares the scrotum (unlike Candida, which often involves the scrotum)
- Worsens with sweating and physical activity
Nail Fungus
- Thickened, distorted nail shape
- Yellow, brown, or white discoloration
- Crumbling or ragged nail edges
- Debris accumulation under the nail
- Separation of the nail from the nail bed (onycholysis)
- Possible pain with pressure or tight footwear
- Foul odor in severe cases
Candida Skin Infections
- Bright red, moist, glistening patches in skin folds
- Satellite pustules (small pustules beyond the main rash border)
- Itching, burning, and soreness
- Maceration (softening and whitening) of surrounding skin
- Angular cheilitis: cracking and redness at the corners of the mouth
Tinea Versicolor
- Patches of skin lighter or darker than the surrounding area
- Fine, powdery scale when scratched
- Typically located on the trunk, shoulders, and upper arms
- More noticeable after sun exposure (affected areas do not tan)
- Mild itching, often worse with sweating
- Patches may be pink, tan, brown, or white
Conventional Treatments
Topical Antifungals
Topical agents are the first-line treatment for most superficial fungal infections:
- Clotrimazole (1%) — A broad-spectrum azole antifungal available over the counter. Effective for athlete's foot, ringworm, jock itch, and Candida infections. Applied twice daily for 2-4 weeks.
- Terbinafine (1%) — An allylamine antifungal that is fungicidal (kills fungi) rather than just fungistatic. Highly effective against dermatophytes. Available over the counter. Applied once or twice daily for 1-2 weeks for athlete's foot.
- Miconazole (2%) — Another azole antifungal effective against dermatophytes and Candida. Applied twice daily.
- Ketoconazole (2%) — Available as cream or shampoo. The shampoo form is particularly useful for tinea versicolor and seborrheic dermatitis.
- Ciclopirox (8% nail lacquer) — A topical treatment for mild to moderate nail fungus. Applied daily to affected nails for up to 48 weeks. Cure rates are modest (approximately 30%).
- Nystatin — Specifically effective against Candida. Available as cream, powder, and oral suspension. Not effective against dermatophytes.
Oral Antifungals
Oral medications are necessary for more extensive infections and for nail fungus:
- Terbinafine (oral) — The most effective oral treatment for dermatophyte nail fungus. Taken daily for 6 weeks (fingernails) or 12 weeks (toenails). Cure rates of 70-80%. Side effects include GI upset, taste disturbance, headache, and rarely liver toxicity. Liver function monitoring is recommended.
- Fluconazole — An azole antifungal used for Candida infections and sometimes as pulse therapy for nail fungus (150-300 mg once weekly). Generally well-tolerated but can interact with many medications through CYP450 enzyme inhibition.
- Itraconazole — A broad-spectrum azole used for dermatophytes and Candida. Can be given as continuous or pulse therapy for nail fungus. Drug interactions are common and must be carefully evaluated.
- Griseofulvin — An older antifungal used primarily for scalp ringworm in children. Requires a longer treatment course and has been largely replaced by newer agents for most indications.
Natural Antifungal Approaches
Numerous natural substances have demonstrated antifungal activity in laboratory and clinical studies. A naturopathic approach often combines multiple agents to address the infection from different angles.
Tea Tree Oil
Tea tree oil (Melaleuca alternifolia) is one of the most well-studied natural antifungals. Its active compounds, terpinen-4-ol and 1,8-cineole, have broad-spectrum activity against dermatophytes, Candida, and Malassezia. Clinical studies have demonstrated:
- A 25-50% tea tree oil solution applied twice daily is effective for athlete's foot
- 100% tea tree oil applied twice daily for 6 months showed comparable improvement to clotrimazole for nail fungus
- 5% tea tree oil body wash helps prevent recurrence of tinea corporis and tinea pedis
Always perform a patch test before widespread use, as contact allergy can develop. Do not ingest tea tree oil.
Oregano Oil
Oregano oil (Origanum vulgare) contains carvacrol and thymol, potent antifungal compounds that disrupt fungal cell membranes. Both topical and oral oregano oil have antifungal applications:
- Topical application (diluted in a carrier oil) for skin fungal infections
- Oral supplementation (enteric-coated capsules, 200 mg 2-3 times daily) for systemic Candida overgrowth
- Effective against Candida species, including azole-resistant strains
Caprylic Acid
Caprylic acid is a medium-chain fatty acid found naturally in coconut oil and palm kernel oil. It has potent antifungal activity against Candida species by disrupting the fungal cell membrane. Supplemental caprylic acid (500-1,000 mg three times daily with meals) is commonly used in naturopathic Candida protocols. It is well-tolerated and does not contribute to antibiotic resistance.
Undecylenic Acid
Undecylenic acid is a naturally occurring fatty acid derived from castor oil. It has been used as an antifungal agent for decades and is the active ingredient in several over-the-counter antifungal products. It is effective against dermatophytes and Candida and is available as topical liquids, powders, and creams. Particularly useful for athlete's foot and nail fungus when applied consistently.
Coconut Oil and Monolaurin
Coconut oil contains lauric acid, which is converted in the body to monolaurin, a compound with antifungal, antibacterial, and antiviral properties. Monolaurin disrupts fungal cell membranes and has demonstrated activity against Candida, including biofilm-forming strains. Coconut oil can be applied topically to affected skin areas and consumed as part of an anti-fungal diet. Supplemental monolaurin (600-1,800 mg daily) provides more concentrated antifungal support.
Garlic and Allicin
Garlic (Allium sativum) contains allicin, a sulfur compound with broad-spectrum antimicrobial activity. Allicin has demonstrated antifungal effects against dermatophytes, Candida species, and Aspergillus. Both topical application (crushed raw garlic or garlic extract) and oral supplementation (aged garlic extract or allicin-standardized supplements at 300-600 mg daily) can be used. Raw garlic applied directly to skin should be diluted or used briefly, as it can cause irritation or chemical burns.
Grapefruit Seed Extract
Grapefruit seed extract (GSE) has demonstrated antifungal activity against Candida and dermatophyte species in laboratory studies. It is available as liquid drops (for internal use, diluted in water, 10-15 drops 2-3 times daily) and as a topical solution. GSE is often included in comprehensive antifungal protocols alongside other agents. Some controversy exists regarding whether the antifungal activity is due to natural compounds or preservatives used in commercial preparations, so sourcing a high-quality product is important.
Pau d'Arco
Pau d'arco (Tabebuia impetiginosa) is a South American tree bark with a long history of traditional use for infections. The active compounds, lapachol and beta-lapachone, have antifungal activity against Candida, dermatophytes, and other fungi. Pau d'arco is typically consumed as a tea (1-2 tablespoons of dried bark simmered in water for 15-20 minutes, 2-3 cups daily) or as a standardized extract in capsule form.
Black Walnut
Black walnut (Juglans nigra) hull contains juglone, a naphthoquinone compound with antifungal, antibacterial, and antiparasitic properties. Black walnut tincture or capsules are commonly used in naturopathic antifungal protocols, particularly for Candida overgrowth. The hull extract is also available in topical form for skin infections. Typical oral dosing is 500-1,000 mg of black walnut hull extract daily.
Candida Overgrowth and Systemic Connection
Recurrent fungal skin infections, particularly Candida infections, often point to an underlying systemic Candida overgrowth originating in the gastrointestinal tract.
What Is Candida Overgrowth?
Candida is a normal inhabitant of the human gut, mouth, and vaginal tract. In a healthy microbiome, Candida is kept in check by beneficial bacteria and a functioning immune system. When this balance is disrupted — by antibiotics, high-sugar diets, chronic stress, immunosuppression, or oral contraceptives — Candida can overgrow and transition from its benign yeast form to an invasive hyphal (filamentous) form that can penetrate the intestinal lining.
Signs of Systemic Candida Overgrowth
- Recurrent skin fungal infections or vaginal yeast infections
- Oral thrush (white coating on the tongue)
- Digestive symptoms — bloating, gas, constipation or diarrhea
- Sugar and carbohydrate cravings
- Brain fog and fatigue
- Joint pain
- Mood disturbances — anxiety, depression, irritability
The Gut-Skin Connection
Candida overgrowth in the gut contributes to skin fungal infections through several mechanisms:
- Intestinal permeability — Invasive Candida hyphae physically damage the intestinal lining, allowing fungal metabolites, toxins, and food particles to enter the bloodstream
- Immune dysregulation — Chronic Candida overgrowth shifts the immune response from Th1 (cell-mediated, anti-fungal) to Th2 (antibody-mediated), paradoxically reducing the body's ability to fight fungal infections
- Acetaldehyde production — Candida produces acetaldehyde as a metabolic byproduct, which impairs liver detoxification, damages tissues, and causes many of the systemic symptoms associated with Candida overgrowth
- Nutrient depletion — Candida competes for nutrients (particularly B vitamins, zinc, and iron) that are essential for immune function and skin health
Biofilm Disruption
One of the most important and often overlooked aspects of treating fungal infections is addressing biofilms — structured communities of fungal cells encased in a self-produced matrix of polysaccharides, proteins, and DNA.
What Are Biofilms?
Fungi, particularly Candida species, can form biofilms on living tissues and medical devices. Biofilms are highly resistant to antifungal agents — up to 1,000 times more resistant than free-floating (planktonic) fungal cells. This is a primary reason why some fungal infections, especially nail fungus and chronic Candida, are so difficult to eradicate with standard antifungal treatments.
Biofilm Disrupting Agents
Incorporating biofilm-disrupting agents alongside antifungal treatment can significantly improve outcomes:
- N-acetylcysteine (NAC) — 600-1,200 mg daily. NAC disrupts the structural matrix of fungal biofilms and has been shown to enhance the effectiveness of antifungal drugs against Candida biofilms.
- Enzymes — Proteolytic enzymes (serrapeptase, nattokinase) and polysaccharide-degrading enzymes (cellulase, hemicellulase) can break down components of the biofilm matrix. Take on an empty stomach for systemic effect.
- Lactoferrin — An iron-binding protein found in colostrum and whey that disrupts Candida biofilms by sequestering the iron that Candida needs for biofilm formation.
- EDTA — A chelating agent that disrupts biofilm structure by removing calcium and other divalent cations. Used in some professional protocols.
- Xylitol — A sugar alcohol that interferes with biofilm adhesion and has shown activity against Candida biofilms
Practical Biofilm Protocol
For chronic or recurrent fungal infections, a biofilm disruption protocol typically involves:
- Phase 1 (Days 1-3): Biofilm-disrupting enzymes and NAC on an empty stomach to break open established biofilms
- Phase 2 (Days 4-30+): Antifungal agents (natural or pharmaceutical) combined with continued biofilm disruptors
- Ongoing: Probiotics (taken at a separate time from antifungals) to recolonize with beneficial organisms
Anti-Fungal Diet
Dietary modification is a cornerstone of naturopathic treatment for fungal infections, particularly for Candida-related conditions.
Foods to Eliminate or Strictly Limit
- Sugar in all forms — Refined sugar, honey, maple syrup, agave, fruit juice, and dried fruit. Sugar directly feeds Candida and promotes its growth.
- Refined carbohydrates — White bread, pasta, pastries, and other products made with white flour are rapidly converted to glucose
- Alcohol — Feeds yeast, impairs immune function, and burdens the liver
- Yeast-containing foods — Bread made with yeast, beer, wine, and nutritional yeast (during active treatment phase)
- Mushrooms and fungi — Some practitioners recommend avoidance during active Candida treatment, though evidence is limited
- Vinegar (except apple cider vinegar, which some practitioners include) — Produced through fermentation
- Processed and packaged foods — Often contain hidden sugars and additives that promote inflammation
Foods to Emphasize
- Non-starchy vegetables — Broccoli, cauliflower, spinach, kale, zucchini, asparagus, and Brussels sprouts provide nutrients and fiber without feeding yeast
- Quality proteins — Wild-caught fish, organic poultry, grass-fed meat, and eggs
- Healthy fats — Coconut oil (antifungal), olive oil, avocado, nuts, and seeds
- Anti-fungal foods — Raw garlic, coconut oil, ginger, turmeric, and rutabaga (contains antifungal compounds)
- Low-sugar fruits — Berries, green apples, and citrus in moderate amounts
- Fermented foods (introduced gradually) — Sauerkraut, kimchi, and coconut kefir provide beneficial bacteria that compete with Candida
- Bone broth — Supports gut lining repair and provides easily absorbed minerals
Duration
A strict anti-fungal diet is typically maintained for 4-12 weeks, depending on the severity of the infection and individual response. Foods are then gradually reintroduced while monitoring for symptom recurrence. Long-term, maintaining a low-sugar, whole-foods diet helps prevent recurrence.
Immune Support
A well-functioning immune system is the body's primary defense against fungal infections. Supporting immune function is essential for both resolving active infections and preventing recurrence.
Key Nutrients for Antifungal Immunity
- Vitamin D — Vitamin D receptors are present on immune cells and play a critical role in activating antimicrobial peptides (cathelicidins and defensins) that fight fungal infections. Deficiency is extremely common and significantly impairs antifungal immunity. Optimal serum levels of 50-70 ng/mL are recommended. Supplementation of 2,000-5,000 IU daily is typical, with dosing guided by blood levels.
- Zinc — Essential for T-cell function, neutrophil activity, and the integrity of skin and mucous membrane barriers. Zinc deficiency increases susceptibility to all types of infections, including fungal. Supplement 25-30 mg daily as zinc picolinate or bisglycinate.
- Vitamin C — Supports white blood cell function and acts as an antioxidant. 1,000-2,000 mg daily in divided doses supports immune function during active infection.
- Vitamin A — Critical for maintaining the integrity of skin and mucosal barriers that serve as the first line of defense against fungal invasion. 5,000-10,000 IU daily from retinol sources.
- Selenium — Supports glutathione production and enhances neutrophil and natural killer cell function. 200 mcg daily from selenomethionine.
- Iron — Iron deficiency impairs immune function, but iron supplementation should only be done when deficiency is confirmed by lab testing, as excess iron can actually feed fungal organisms.
Immune-Supporting Herbs
- Astragalus — Enhances white blood cell production and activity. Suitable for long-term immune support.
- Medicinal mushrooms (reishi, maitake, shiitake extracts) — Contain beta-glucans that enhance macrophage and natural killer cell activity. Beta-glucans specifically upregulate antifungal immune responses.
- Echinacea — Short-term immune stimulant that enhances phagocyte activity and white blood cell production
Gut Health and Immunity
Approximately 70% of the immune system resides in the gut. Maintaining a healthy gut microbiome through probiotics, prebiotics, and gut-healing nutrients (L-glutamine, zinc carnosine) is one of the most effective strategies for supporting the antifungal immune response. Saccharomyces boulardii, a beneficial yeast, is particularly useful — it competes with Candida for binding sites, produces antifungal compounds, and stimulates secretory IgA production.
Prevention Strategies
Prevention is particularly important for individuals with a history of recurrent fungal infections.
Skin Hygiene
- Keep skin clean and dry, especially in skin folds, between toes, and in the groin area
- Dry thoroughly after bathing, paying special attention to web spaces between toes
- Change sweaty clothing promptly after exercise
- Use antifungal powder (natural or conventional) in shoes and on feet if prone to athlete's foot
- Avoid sharing personal items — towels, socks, shoes, nail clippers, and combs
Footwear
- Wear breathable shoes made of natural materials (leather, canvas) rather than synthetic materials that trap moisture
- Alternate shoes daily to allow them to dry completely between wearings
- Wear sandals or shower shoes in communal areas (locker rooms, pool decks, shared showers)
- Choose moisture-wicking socks made of wool or synthetic blends designed to keep feet dry
Clothing
- Wear loose-fitting, breathable clothing, especially in warm weather
- Choose cotton or moisture-wicking undergarments
- Avoid prolonged wearing of wet swimsuits or exercise clothing
Internal Prevention
- Maintain optimal blood sugar — Essential for reducing fungal infection risk, especially in diabetic or pre-diabetic individuals
- Support the gut microbiome with probiotics, especially during and after antibiotic use
- Maintain adequate vitamin D, zinc, and other immune-supporting nutrients
- Follow a low-sugar, whole-foods diet that does not promote fungal overgrowth
- Manage stress to support immune function
Cautions and Considerations
- Proper diagnosis is important — Many skin conditions can mimic fungal infections (eczema, psoriasis, contact dermatitis, bacterial infections). If a presumed fungal infection does not respond to treatment within 2-4 weeks, professional evaluation with possible KOH preparation, fungal culture, or skin biopsy may be needed.
- Oral antifungal medications carry risks of liver toxicity and drug interactions. Liver function tests should be monitored during treatment with oral terbinafine, itraconazole, or ketoconazole.
- Herxheimer reactions (die-off) — When treating systemic Candida overgrowth, the rapid killing of large numbers of yeast organisms can release endotoxins that temporarily worsen symptoms (fatigue, headache, brain fog, GI disturbance). Starting treatment gradually, supporting liver detoxification (milk thistle, NAC, adequate hydration), and using binders (activated charcoal, bentonite clay) can help manage die-off reactions.
- Nail fungus requires patience — Even with effective treatment, toenails grow slowly (approximately 1 mm per month). Full replacement of a fungal toenail may take 12-18 months. Treatment should continue until a completely new, healthy nail has grown in.
- Diabetic foot infections require careful medical attention. Fungal infections in diabetic patients can serve as entry points for bacterial infections and may lead to serious complications including cellulitis and osteomyelitis.
- Pregnancy and breastfeeding — Many oral antifungals (both conventional and herbal) are contraindicated in pregnancy. Topical treatments are generally safer but should still be verified for safety. Consult a qualified healthcare provider.
- Children — Dosing for natural antifungal supplements should be adjusted for children. Some herbal antimicrobials are not appropriate for young children.
- Drug interactions — Herbal antifungals such as oregano oil and berberine can affect liver enzyme activity (CYP450 system) and may interact with prescription medications. Review all supplements with a knowledgeable practitioner.
14. References & Research
Historical Background
The fungal origin of skin infections was first demonstrated in 1841 by David Gruby, a Hungarian-French physician, who identified the dermatophyte responsible for favus (tinea capitis). Robert Remak had independently observed fungal elements in favus lesions in 1837, but Gruby was the first to prove causation through inoculation experiments. Raymond Sabouraud further advanced medical mycology in the early 20th century, developing culture media and classification systems for dermatophytes that remain in use today.
Key Research Papers
- Havlickova B, Czaika VA, Friedrich M. Epidemiological trends in skin mycoses worldwide. Mycoses. 2008;51(Suppl 4):2-15.
- Lipner SR, Scher RK. Onychomycosis: clinical overview and diagnosis. J Am Acad Dermatol. 2019;80(4):835-851.
- Gupta AK, Ryder JE, Johnson AM. Cumulative meta-analysis of systemic antifungal agents for the treatment of onychomycosis. Br J Dermatol. 2004;150(3):537-544.
- Pappas PG, Kauffman CA, Andes DR, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;62(4):e1-e50.
- Ely JW, Rosenfeld S, Seabury Stone M. Diagnosis and management of tinea infections. Am Fam Physician. 2014;90(10):702-710.
- Ramage G, Rajendran R, Sherry L, Williams C. Fungal biofilm resistance. Int J Microbiol. 2012;2012:528521.
- Warnock DW. Trends in the epidemiology of invasive fungal infections. Nihon Ishinkin Gakkai Zasshi. 2007;48(1):1-12.
- Falkow S, White TC, Oliver BG. Candida albicans pathogenesis: fitting within the host-microbe damage response framework. Clin Microbiol Rev. 2010;23(4):884-911.
- Martinez-Rossi NM, Peres NT, Rossi A. Antifungal resistance mechanisms in dermatophytes. Mycopathologia. 2008;166(5-6):369-383.
- Gold MH, Bridges T, Bradshaw VL, et al. AHA-BHA, tea tree oil, and salicylic acid as topical antifungal therapies. J Clin Aesthet Dermatol. 2014;7(3):19-24.
- White TC, Findley K, Dawson TL, et al. Fungi on the skin: dermatophytes and Malassezia. Cold Spring Harb Perspect Med. 2014;4(8):a019802.
- de Hoog GS, Dukik K, Monod M, et al. Toward a novel multilocus phylogenetic taxonomy for the dermatophytes. Mycopathologia. 2017;182(1-2):5-31.
Research Papers
Curated PubMed topic searches of peer-reviewed literature on Fungal Skin Infections. Each link opens a live PubMed query so you always see the most current studies.
- PubMed: Tinea pedis treatment
- PubMed: Tinea corporis
- PubMed: Onychomycosis and terbinafine
- PubMed: Cutaneous candidiasis
- PubMed: Tinea versicolor
- PubMed: Dermatophyte epidemiology
- PubMed: Antifungal resistance
- PubMed: Fungal infections in immunocompromised
- PubMed: Tea tree oil antifungal
- PubMed: Tinea capitis in children
- PubMed: Topical azole therapy
- PubMed: Laser and PDT therapy
Connections
- Tea Tree
- Garlic
- Zinc
- Oregano
- Acne
- Eczema
- Psoriasis
- Gut Healing
- SIBO
- Iron
- Diabetes
- Gut-Brain Axis
- NAC
- Probiotics
- Vitamin A
- Blood Sugar
- Honey
- Obesity
- Yeast Infections