Eucalyptus (Eucalyptus globulus)
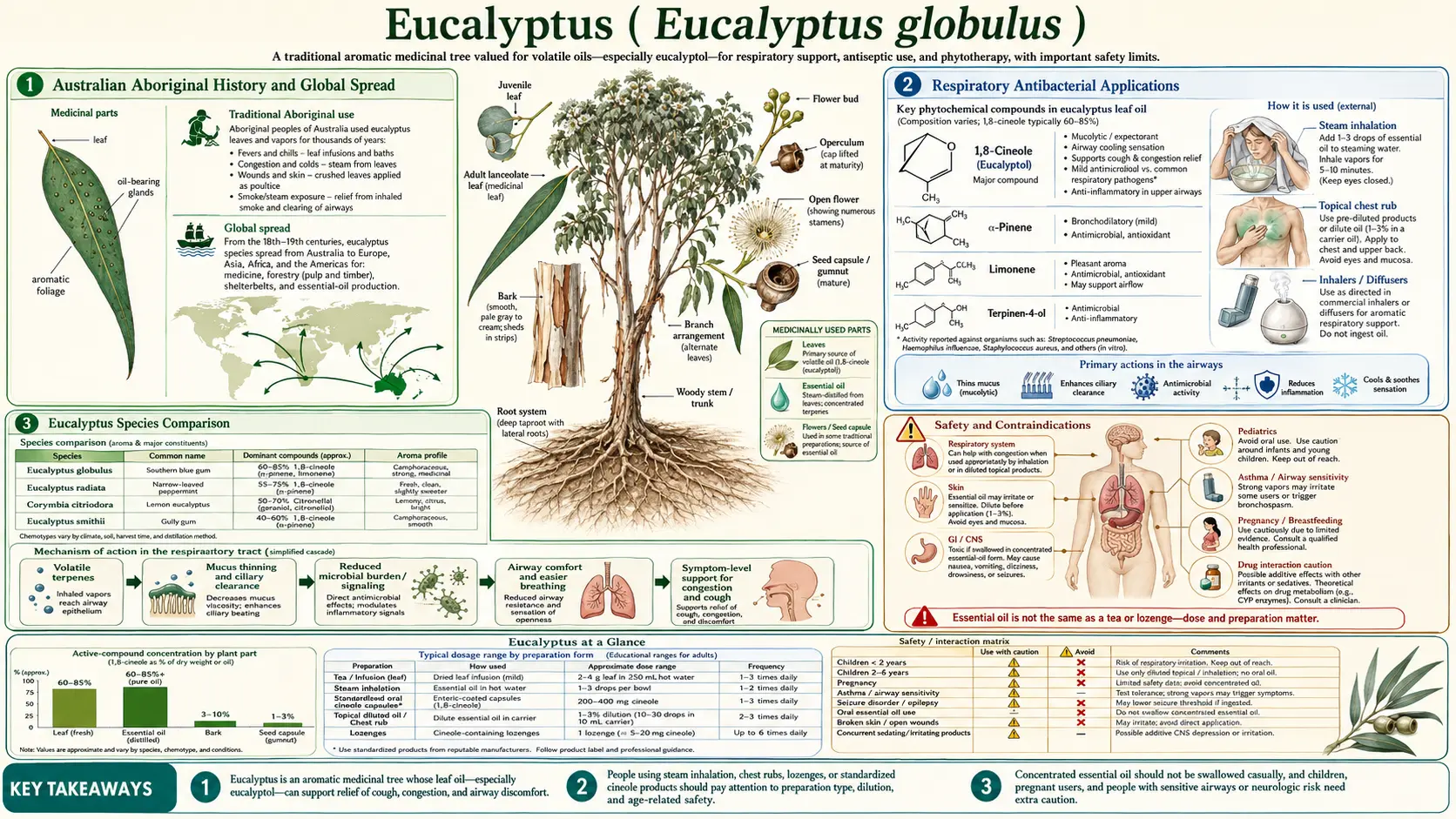
Table of Contents
- Australian Aboriginal History and Global Spread
- Key Antibacterial Compounds
- Mechanism of Antibacterial Action
- Bacteria Targeted
- Research Studies and Clinical Evidence
- Respiratory Antibacterial Applications
- Hospital and Clinical Use
- Wound Care and Topical Applications
- Oral Health
- Eucalyptus Species Comparison
- Synergistic Effects
- Other Health Benefits
- Forms and Preparations
- Recommended Dosage
- Safety and Contraindications
- Key Research Papers and References
- Featured Videos
Australian Aboriginal History and Global Spread
Eucalyptus has been a cornerstone of Australian Aboriginal medicine for tens of thousands of years — its red gum (kino) used as an astringent wound wash and its leaves infused for fevers, colds, and coughs. From the 1850s the German-Australian botanist Ferdinand von Mueller carried Eucalyptus globulus to Europe, Africa, Asia, and the Americas, the pharmacist Joseph Bosisto founded the first commercial eucalyptus-oil industry, and in 1870 the French chemist François Stanislas Cloez isolated and named its key compound, eucalyptol (1,8-cineole). — the fuller story is told in the dedicated History & Traditional Use article.
Key Antibacterial Compounds
The antibacterial potency of Eucalyptus globulus essential oil derives from a complex mixture of volatile terpenoid compounds. Each contributes to the overall antimicrobial effect through distinct biochemical mechanisms, and their combined action produces broad-spectrum antibacterial activity.
- 1,8-Cineole (Eucalyptol): The dominant compound in E. globulus essential oil, comprising 60–90% of total oil content depending on geographical origin, climate, and harvest timing. Eucalyptol is a bicyclic monoterpenoid ether with potent antibacterial, anti-inflammatory, and mucolytic properties. It is the single compound most responsible for eucalyptus oil's ability to penetrate mucus barriers and reach bacteria embedded in respiratory biofilms. Eucalyptol has been isolated and studied extensively as a standalone pharmaceutical compound, marketed under the trade name Soledum in Europe for respiratory infections.
- Alpha-Pinene: A bicyclic monoterpene that typically constitutes 2–10% of E. globulus oil. Alpha-pinene exhibits independent antibacterial activity against both Gram-positive and Gram-negative bacteria and enhances the penetration of other antimicrobial compounds through bacterial cell membranes. It also possesses bronchodilatory and anti-inflammatory properties that complement eucalyptol's respiratory effects.
- Limonene: A cyclic monoterpene present at 1–8% concentration. Limonene demonstrates antibacterial activity by disrupting bacterial membrane integrity and has been shown to enhance the effectiveness of conventional antibiotics when used in combination. It also contributes antioxidant and anti-inflammatory effects.
- p-Cymene: An aromatic monoterpene found at 1–5% concentration in E. globulus oil. While p-cymene alone shows modest direct antibacterial activity, its primary contribution is as a membrane-targeting agent that facilitates the entry of more potent compounds like eucalyptol and alpha-pinene into bacterial cells. p-Cymene inserts itself into the phospholipid bilayer of bacterial membranes, expanding and destabilizing the structure.
- Globulol: A sesquiterpene alcohol unique to eucalyptus species, present at 0.5–4% concentration. Globulol provides sustained antibacterial activity due to its lower volatility compared to monoterpenes, meaning it persists on surfaces and in tissues longer than the more rapidly evaporating primary compounds. It demonstrates particular effectiveness against Staphylococcus aureus and related Gram-positive pathogens.
The relative proportions of these compounds vary significantly based on the eucalyptus species, the geographical region of cultivation, altitude, soil composition, rainfall, and the time of year the leaves are harvested. Pharmacopoeia-grade E. globulus oil typically requires a minimum 1,8-cineole content of 70% to meet medicinal standards.
Mechanism of Antibacterial Action
Eucalyptus oil exerts its antibacterial effects through multiple simultaneous mechanisms, making it difficult for bacteria to develop resistance. Unlike single-target pharmaceutical antibiotics, eucalyptus attacks bacterial cells on several fronts at once.
Membrane Disruption
The primary antibacterial mechanism of eucalyptus oil involves the disruption of bacterial cell membrane integrity. The lipophilic terpenoid compounds in eucalyptus oil, particularly eucalyptol and alpha-pinene, integrate into the phospholipid bilayer of bacterial cell membranes. This integration causes expansion and destabilization of the membrane, increasing its permeability. As a result, essential intracellular contents including ions, ATP, and proteins leak out of the bacterial cell, collapsing the proton motive force and halting cellular energy production. The cell loses its ability to maintain homeostasis and dies.
Studies using electron microscopy have demonstrated visible morphological changes in bacteria exposed to eucalyptus oil, including membrane blebbing, cytoplasmic condensation, and complete cell lysis. The effect is concentration-dependent, with sub-inhibitory concentrations causing partial membrane damage that sensitizes bacteria to other antimicrobial agents.
Mucus Penetration
A property unique to eucalyptus among commonly used antibacterial herbs is its exceptional ability to penetrate mucus barriers. The respiratory tract is lined with a thick mucus layer that serves as a physical barrier against pathogens but also shields bacteria once they become embedded within it. Eucalyptol possesses powerful mucolytic activity, breaking down the disulfide bonds in mucin glycoproteins that give mucus its viscous, gel-like consistency. By liquefying and thinning the mucus layer, eucalyptol exposes embedded bacteria to both the immune system and to the oil's own antibacterial compounds.
This mucolytic action distinguishes eucalyptus from other antibacterial essential oils such as tea tree or oregano, which lack significant mucus-penetrating capacity. Clinical studies have demonstrated that inhaled eucalyptol reaches measurable concentrations in bronchial mucus within 20 minutes and maintains therapeutically active levels for several hours.
Respiratory Biofilm Disruption
Many respiratory pathogens, including Pseudomonas aeruginosa, Haemophilus influenzae, and Streptococcus pneumoniae, form biofilms on the epithelial surfaces of the airways. These biofilms are structured communities of bacteria encased in a self-produced matrix of polysaccharides, proteins, and extracellular DNA. Biofilm-embedded bacteria are 100 to 1,000 times more resistant to antibiotics than their free-floating (planktonic) counterparts.
Eucalyptus oil has demonstrated the ability to disrupt both the formation and the structural integrity of established biofilms. Eucalyptol interferes with quorum sensing, the chemical communication system bacteria use to coordinate biofilm formation and virulence factor production. By disrupting quorum sensing signals, eucalyptol prevents bacteria from establishing the cooperative behaviors necessary for biofilm development. Against pre-formed biofilms, the oil's lipophilic compounds penetrate the extracellular matrix, destabilizing its structure and exposing the resident bacteria to immune clearance and antibiotic treatment.
Bacteria Targeted
Eucalyptus oil has demonstrated antibacterial activity against a broad range of clinically significant pathogens. The following bacteria have been studied extensively in laboratory and, in some cases, clinical settings:
- Staphylococcus aureus: One of the most common causes of skin infections, wound infections, and hospital-acquired infections. Eucalyptus oil shows strong bactericidal activity against S. aureus at concentrations as low as 0.25–0.5% (v/v) in laboratory disc diffusion assays. Eucalyptol alone demonstrates significant inhibition zones against both methicillin-sensitive strains and resistant isolates.
- Methicillin-Resistant Staphylococcus aureus (MRSA): Of particular clinical importance, eucalyptus oil retains antibacterial activity against MRSA strains that are resistant to beta-lactam antibiotics. Multiple studies have reported minimum inhibitory concentrations (MICs) of eucalyptus oil against MRSA ranging from 0.125% to 1.0%, depending on the strain and oil chemotype. The multi-compound nature of the oil makes it effective even against bacteria that have developed resistance to single-compound drugs.
- Haemophilus influenzae: A major cause of otitis media, sinusitis, bronchitis, and community-acquired pneumonia. Eucalyptus oil demonstrates particular effectiveness against H. influenzae due to its ability to penetrate the mucoid environment in which this bacterium thrives. Clinical studies using cineole inhalation have shown significant reduction in H. influenzae colonization in patients with chronic sinusitis.
- Streptococcus pneumoniae: The leading cause of community-acquired pneumonia, bacterial meningitis, and acute otitis media. Eucalyptus oil and isolated eucalyptol show inhibitory activity against both penicillin-sensitive and penicillin-resistant strains of S. pneumoniae, with MIC values comparable to those observed against S. aureus.
- Moraxella catarrhalis: A significant respiratory pathogen responsible for otitis media, sinusitis, and exacerbations of chronic obstructive pulmonary disease. Eucalyptus oil is highly effective against M. catarrhalis, with inhibition zones consistently among the largest observed across all tested respiratory pathogens.
- Escherichia coli: A Gram-negative bacterium responsible for urinary tract infections, gastrointestinal infections, and sepsis. While Gram-negative bacteria are generally more resistant to essential oils due to their outer membrane barrier, eucalyptus oil demonstrates moderate to strong activity against E. coli, particularly when combined with membrane-permeabilizing agents or other essential oils.
- Pseudomonas aeruginosa: A notoriously resistant Gram-negative opportunistic pathogen that causes severe infections in immunocompromised patients and is a leading cause of ventilator-associated pneumonia. Eucalyptus oil alone shows moderate activity against P. aeruginosa, but its biofilm-disrupting properties make it a valuable adjunct to conventional antibiotic therapy against this organism.
- Mycobacterium tuberculosis: The causative agent of tuberculosis. Eucalyptus oil and eucalyptol have demonstrated inhibitory activity against M. tuberculosis in vitro, with particular interest in their potential role as adjunctive agents to standard tuberculosis therapy. The lipophilic nature of eucalyptol allows it to penetrate the waxy mycolic acid cell wall that makes mycobacteria inherently resistant to many antimicrobial agents.
Research Studies and Clinical Evidence
The antibacterial properties of eucalyptus have been documented in numerous peer-reviewed studies across microbiology, pharmacology, and clinical medicine journals.
Clinical Microbiology and Infection
Research published in Clinical Microbiology and Infection has examined the in vitro antibacterial activity of Eucalyptus globulus essential oil against panels of clinical bacterial isolates. These studies employed standardized broth microdilution and disc diffusion methods according to Clinical and Laboratory Standards Institute (CLSI) guidelines. Results demonstrated that eucalyptus oil exhibited bactericidal activity against all tested Gram-positive organisms and bacteriostatic to bactericidal activity against most Gram-negative organisms. The minimum bactericidal concentration (MBC) was typically within two dilutions of the MIC, indicating rapid killing rather than mere growth inhibition.
Phytomedicine
Studies published in Phytomedicine have investigated the mechanism of eucalyptus oil's antibacterial action at the molecular level. Using flow cytometry, fluorescence microscopy, and membrane permeability assays, researchers demonstrated that eucalyptol causes dose-dependent disruption of bacterial membrane potential and integrity. The journal has also published clinical trials evaluating oral cineole capsules (200 mg three times daily) for the treatment of acute sinusitis, showing statistically significant improvement in symptom scores compared to placebo at days 4 and 7 of treatment.
BMC Infectious Diseases
Research in BMC Infectious Diseases has explored the potential of eucalyptus oil as an adjunctive agent in the treatment of multidrug-resistant infections. Studies have documented synergistic interactions between eucalyptus oil and conventional antibiotics, including ampicillin, gentamicin, and ciprofloxacin, against clinical isolates of MRSA, extended-spectrum beta-lactamase (ESBL)-producing E. coli, and carbapenem-resistant P. aeruginosa. The fractional inhibitory concentration index (FICI) values in combination studies consistently fell below 0.5, indicating true synergism rather than additive effects.
Additional studies have examined the efficacy of eucalyptus oil vapor in reducing airborne bacterial counts in clinical environments, demonstrating significant reductions in colony-forming units (CFU) after 30 and 60 minutes of exposure to eucalyptus oil diffusion.
Respiratory Antibacterial Applications
The respiratory tract represents the primary therapeutic domain for eucalyptus-based antibacterial interventions. The combination of direct antibacterial activity, mucolytic action, and anti-inflammatory effects makes eucalyptus uniquely suited for respiratory infections.
Sinusitis
Acute and chronic sinusitis frequently involve bacterial infection with S. pneumoniae, H. influenzae, and M. catarrhalis. Multiple randomized controlled trials have demonstrated that oral cineole capsules (200 mg three times daily) significantly reduce sinusitis symptoms including nasal congestion, headache, and facial pain compared to placebo. In these trials, cineole was used as monotherapy without concurrent antibiotics, and patients treated with cineole showed faster symptom resolution and lower rates of antibiotic rescue therapy. The mucolytic action of cineole promotes drainage of infected sinus contents while its antibacterial properties directly combat the causative organisms.
Bronchitis
In acute bronchitis, eucalyptus-based preparations help by thinning bronchial secretions, facilitating expectoration of infected mucus, and exerting direct antibacterial effects against common causative organisms. Clinical trials using cineole capsules as adjunctive therapy alongside standard treatment for acute bronchitis have shown significant reductions in cough frequency, sputum production, and duration of illness. For chronic bronchitis and acute exacerbations of chronic obstructive pulmonary disease, cineole has demonstrated the ability to reduce exacerbation frequency when used as long-term maintenance therapy.
Pneumonia Support
While eucalyptus is not a substitute for antibiotic therapy in bacterial pneumonia, it serves a valuable supportive role. Steam inhalation with eucalyptus oil helps mobilize secretions in the lower respiratory tract, improving airway clearance and reducing the bacterial burden in bronchial mucus. The anti-inflammatory properties of eucalyptol reduce excessive inflammatory responses in the lung parenchyma, potentially limiting tissue damage. Some integrative medicine practitioners recommend eucalyptus steam inhalation as a complementary therapy alongside prescribed antibiotics for community-acquired pneumonia.
Cineole Clinical Trials
Pure 1,8-cineole has been the subject of over 20 randomized controlled clinical trials for respiratory conditions. The most extensively studied formulation is enteric-coated cineole capsules at 200 mg doses. Key findings across these trials include a 50–70% improvement in mucociliary clearance measured by saccharin transit time, significant reduction in inflammatory markers including leukotrienes, prostaglandins, and tumor necrosis factor-alpha in bronchial lavage fluid, and faster resolution of radiographic findings in patients with lower respiratory tract infections.
Steam Inhalation
Traditional steam inhalation with eucalyptus oil remains a widely used method of delivering antibacterial compounds directly to the respiratory mucosa. Adding 3–5 drops of eucalyptus essential oil to a bowl of hot water and inhaling the vapor for 10–15 minutes allows eucalyptol and other volatile compounds to reach the nasal passages, sinuses, pharynx, larynx, and upper bronchial tree. Studies using gas chromatography-mass spectrometry (GC-MS) have confirmed that therapeutically relevant concentrations of eucalyptol are achieved in bronchial mucus within 20 minutes of steam inhalation and persist for 2–4 hours.
Hospital and Clinical Use
Air Disinfection Research
Multiple studies have investigated the potential of eucalyptus oil vapor for reducing airborne bacterial contamination in clinical settings. Research conducted in hospital wards, operating theaters, and intensive care units has demonstrated that diffusion of eucalyptus oil into ambient air produces significant reductions in airborne bacterial colony counts. Studies using settle plate methodology and active air sampling have reported 40–70% reductions in total airborne bacterial CFU after 60 minutes of eucalyptus oil diffusion at concentrations of 0.05–0.1 mL per cubic meter of air. These findings have prompted interest in eucalyptus-based air disinfection as a complementary strategy for reducing hospital-acquired infections, particularly in resource-limited settings where advanced air filtration systems may be unavailable.
Surgical Wound Antiseptic History
Eucalyptus oil has a distinguished history in surgical antisepsis. Following Joseph Lister's pioneering work on antiseptic surgery in the 1860s, eucalyptus oil was adopted alongside carbolic acid as a wound disinfectant in operating theaters throughout the British Empire. Australian military surgeons used eucalyptus-based antiseptic preparations extensively during the Boer War and World War I, where they reported favorable wound healing outcomes compared to other available antiseptics. Eucalyptus oil's advantage lay in its combination of antibacterial activity with relatively low tissue toxicity compared to phenol and other chemical antiseptics of the era. By the early 20th century, eucalyptus oil was listed in the British Pharmacopoeia and multiple colonial pharmacopoeias as an approved wound antiseptic.
Hospital-Acquired Infection Studies
Contemporary research has evaluated eucalyptus oil's potential role in combating hospital-acquired infections (HAIs), which affect approximately 1 in 31 hospital patients in developed countries. Studies have examined eucalyptus oil-based surface disinfectants, hand hygiene formulations, and air purification systems. Results indicate that eucalyptus oil solutions at concentrations of 1–5% effectively eliminate common nosocomial pathogens including MRSA, vancomycin-resistant Enterococcus (VRE), and Clostridium difficile from hard surfaces within 10 minutes of contact. However, its relatively slow kill time compared to synthetic disinfectants limits its use as a primary hospital-grade disinfectant, positioning it more as a complementary or adjunctive agent.
Wound Care and Topical Applications
Burns
Eucalyptus oil has been investigated for use in burn wound management due to its combined antibacterial and anti-inflammatory properties. Burn wounds are highly susceptible to bacterial colonization, particularly by S. aureus, P. aeruginosa, and Acinetobacter baumannii. Studies using animal burn wound models have demonstrated that topical application of diluted eucalyptus oil (2–5% in a carrier) reduces bacterial colonization counts by 2–3 log units compared to untreated controls and promotes faster wound epithelialization. The anti-inflammatory action of eucalyptol helps reduce excessive inflammation in the burn wound bed, which can impede healing.
Ulcers
Chronic skin ulcers, including diabetic foot ulcers and venous leg ulcers, represent a significant clinical challenge due to persistent bacterial biofilm infection. Eucalyptus oil's biofilm-disrupting properties make it a promising adjunctive agent for chronic wound management. In vitro studies using wound-relevant biofilm models have demonstrated that eucalyptus oil penetrates and disrupts established biofilms of S. aureus and P. aeruginosa, the two most common colonizers of chronic wounds. Clinical case series have reported improved healing outcomes when eucalyptus-based wound dressings are used as part of a comprehensive wound care protocol.
Insect Bites
Diluted eucalyptus oil applied topically to insect bites provides both antibacterial protection against secondary infection and local analgesic and anti-inflammatory effects. The cooling sensation produced by eucalyptol activates TRPM8 cold-sensitive receptors in the skin, providing symptomatic relief from itching and pain. The antibacterial action prevents opportunistic infection of bite wounds, which is particularly important in tropical and subtropical regions where insect bites frequently become infected.
Surgical Dressings
Modern wound care research has explored the incorporation of eucalyptus oil into advanced wound dressing materials. Eucalyptus oil has been successfully incorporated into hydrogels, nanofiber mats, chitosan films, and alginate dressings, providing sustained-release antibacterial activity at the wound surface. These eucalyptus-impregnated dressings maintain antibacterial activity for 24–72 hours depending on the delivery system, reducing the frequency of dressing changes and associated wound disturbance. Studies have demonstrated that eucalyptus-loaded nanofiber dressings inhibit growth of wound-relevant pathogens while maintaining cytocompatibility with human fibroblasts and keratinocytes.
Oral Health
Mouthwash Studies
Eucalyptol is a key active ingredient in several commercially available antiseptic mouthwashes, most notably Listerine, where it is combined with thymol, menthol, and methyl salicylate. Clinical trials comparing eucalyptol-containing mouthwashes to placebo and to chlorhexidine (the gold-standard prescription mouthwash) have demonstrated significant reductions in plaque accumulation, gingivitis severity, and total oral bacterial counts. While eucalyptol-based mouthwashes are generally less potent than chlorhexidine for short-term plaque control, they offer advantages for long-term use due to their lack of tooth staining and taste disturbance side effects.
Dental Bacteria
Eucalyptus oil demonstrates antibacterial activity against the major oral pathogens responsible for dental caries and periodontal disease. In vitro studies have shown significant inhibition of Streptococcus mutans (the primary caries-causing bacterium), Porphyromonas gingivalis (a key periodontal pathogen), Fusobacterium nucleatum (involved in oral biofilm maturation), and Aggregatibacter actinomycetemcomitans (associated with aggressive periodontitis). The biofilm-disrupting properties of eucalyptus oil are particularly relevant in oral health, as dental plaque is a bacterial biofilm, and disruption of its matrix structure enhances the effectiveness of mechanical hygiene measures.
Halitosis
Eucalyptus oil is effective against the volatile sulfur compound-producing bacteria responsible for halitosis. The primary halitosis-causing organisms, including P. gingivalis, Prevotella intermedia, and Treponema denticola, are susceptible to eucalyptol at concentrations achieved in commercially available mouthwashes. Clinical studies have demonstrated significant reductions in organoleptic halitosis scores and volatile sulfur compound measurements following the use of eucalyptol-containing oral rinses. The fresh, mentholated character of eucalyptol also provides immediate masking of malodor while the antibacterial effect reduces odor-producing bacterial populations over time.
Eucalyptus Species Comparison
The genus Eucalyptus comprises over 700 species, but only a handful are used medicinally. The three most commonly employed species differ significantly in their chemical composition and antibacterial potency.
Eucalyptus globulus (Blue Gum)
E. globulus is the most widely used species in Western herbal medicine and pharmaceutical preparations. Its essential oil contains the highest concentration of 1,8-cineole among commonly cultivated species, typically 60–90%. This high eucalyptol content gives E. globulus the strongest overall antibacterial activity in standardized in vitro testing. It is the species most commonly referenced in pharmacopoeia monographs and the most extensively studied in clinical trials. E. globulus oil has the most potent mucolytic action and is considered the species of choice for respiratory antibacterial applications. Its aroma is strong, sharp, and camphoraceous.
Eucalyptus radiata (Narrow-Leaved Peppermint)
E. radiata contains a moderate concentration of 1,8-cineole, typically 60–75%, along with higher proportions of alpha-terpineol and other monoterpenols compared to E. globulus. While its direct antibacterial potency is somewhat lower than E. globulus in disc diffusion assays, E. radiata is better tolerated by children and individuals with sensitive respiratory tracts. It is often preferred by aromatherapists for pediatric applications and for patients who find E. globulus too stimulating. Its aroma is softer, more peppery, and less camphoraceous.
Eucalyptus citriodora (Lemon-Scented Gum)
E. citriodora has a fundamentally different chemical profile, with its oil dominated by citronellal (65–85%) rather than 1,8-cineole, which is present at only 1–5%. This gives it a distinctly lemony aroma quite unlike other eucalyptus species. While E. citriodora shows lower direct antibacterial activity against respiratory pathogens compared to E. globulus, it demonstrates stronger activity against certain Gram-negative bacteria and possesses superior antifungal properties. It is also a more effective insect repellent, with the CDC recognizing oil of lemon eucalyptus as an effective alternative to DEET. For antibacterial applications specifically, E. citriodora is generally considered the least potent of the three common medicinal species.
Synergistic Effects
One of the most promising areas of eucalyptus antibacterial research involves its synergistic interactions with other essential oils and with conventional antibiotic drugs. Synergism occurs when the combined effect of two agents exceeds the sum of their individual effects, allowing lower doses of each to achieve equivalent or superior antibacterial activity.
With Tea Tree Oil
The combination of eucalyptus oil and tea tree oil (Melaleuca alternifolia) produces consistently synergistic antibacterial effects against both Gram-positive and Gram-negative bacteria. Tea tree oil's primary compound, terpinen-4-ol, acts through membrane disruption mechanisms that complement eucalyptol's activity. Checkerboard assay studies have demonstrated FICI values of 0.25–0.50 against MRSA, indicating strong synergism. The combination is particularly effective for topical wound care applications, where the two oils together provide broader-spectrum coverage than either alone.
With Thyme Oil
Thyme oil (Thymus vulgaris), rich in thymol and carvacrol, demonstrates powerful synergism with eucalyptus oil. The phenolic compounds in thyme oil attack bacterial membranes through a different mechanism than eucalyptol's terpenoid ether structure, and the two attack modalities together produce rapid bactericidal effects. Studies have shown that the eucalyptus-thyme combination achieves kill times 2–4 times faster than either oil alone against common respiratory pathogens.
With Peppermint Oil
Peppermint oil (Mentha piperita), containing menthol and menthone, enhances eucalyptus oil's antibacterial activity while adding additional cooling and analgesic properties. The combination is particularly useful in respiratory applications, where menthol's bronchodilatory effects complement eucalyptol's mucolytic action. The two oils together improve both symptom relief and bacterial clearance in upper respiratory tract infections.
With Conventional Antibiotics
Perhaps the most clinically significant synergistic interactions involve eucalyptus oil combined with conventional antibiotic drugs. Research has demonstrated that sub-inhibitory concentrations of eucalyptus oil can restore the effectiveness of antibiotics against resistant organisms. For example, the combination of eucalyptus oil with ampicillin has shown synergistic effects against MRSA isolates that are fully resistant to ampicillin alone. Similar synergistic interactions have been documented with gentamicin against resistant P. aeruginosa and with ciprofloxacin against resistant E. coli. The proposed mechanism involves eucalyptus oil's disruption of bacterial membrane efflux pumps, which are a primary resistance mechanism through which bacteria actively pump antibiotics out of their cells.
Other Health Benefits
Beyond its antibacterial properties, eucalyptus offers a range of additional health benefits that contribute to its overall therapeutic value.
- Anti-Inflammatory: Eucalyptol inhibits the production of pro-inflammatory cytokines including tumor necrosis factor-alpha (TNF-alpha), interleukin-1-beta (IL-1-beta), and interleukin-6 (IL-6). It also suppresses the arachidonic acid cascade by inhibiting both cyclooxygenase-2 (COX-2) and 5-lipoxygenase (5-LOX), reducing production of both prostaglandins and leukotrienes. This dual anti-inflammatory mechanism is unusual among natural compounds and contributes significantly to eucalyptus's effectiveness in inflammatory respiratory conditions such as asthma, COPD, and allergic rhinitis.
- Analgesic: Topical application of eucalyptus oil produces localized pain relief through activation of TRPM8 cold receptors and inhibition of TRPA1 pain receptors. Clinical trials have demonstrated the effectiveness of eucalyptus oil formulations for musculoskeletal pain, tension headaches, and post-surgical pain. Inhaled eucalyptol has been shown to reduce the perception of pain in experimental settings through central nervous system modulation.
- Decongestant: Eucalyptol is one of the most effective natural nasal decongestants. It stimulates cold receptors in the nasal mucosa, producing a subjective sensation of improved airflow, while simultaneously reducing mucosal inflammation and promoting mucus drainage. These combined effects provide both immediate symptomatic relief and genuine improvement in nasal airway patency as measured by rhinomanometry.
- Antifungal: Eucalyptus oil demonstrates antifungal activity against dermatophytes (Trichophyton, Microsporum, Epidermophyton species), Candida albicans, and Aspergillus species. While not as potent an antifungal as tea tree or oregano oil, eucalyptus oil's antifungal properties complement its antibacterial activity in wound care and skin applications where mixed infections are common.
- Insect Repellent: Oil of lemon eucalyptus (E. citriodora) and its derivative p-menthane-3,8-diol (PMD) are recognized by the CDC and EPA as effective mosquito repellents with efficacy comparable to low-concentration DEET formulations. E. globulus oil also possesses insect repellent properties, though less potent than the lemon-scented species. Eucalyptus-based repellents provide 2–5 hours of protection against mosquitoes, ticks, and biting flies depending on concentration and formulation.
Forms and Preparations
- Essential Oil: Steam-distilled from the leaves and small branches of E. globulus. Pharmaceutical-grade oil should contain a minimum of 70% 1,8-cineole. Used for inhalation, topical application (always diluted), and as a starting material for isolated cineole production. Available in 10 mL, 30 mL, and 100 mL bottles from reputable essential oil suppliers. Must be stored in dark glass containers away from heat and light.
- Chest Rubs: Commercial vapor rubs containing eucalyptus oil, typically combined with menthol and camphor in a petrolatum or ointment base. Applied to the chest, throat, and back to deliver eucalyptol vapor through inhalation during sleep. Widely available over-the-counter products include Vicks VapoRub and similar formulations. Provide sustained low-level eucalyptol delivery over several hours.
- Lozenges: Eucalyptus-flavored throat lozenges deliver eucalyptol directly to the oral and pharyngeal mucosa. Available in various strengths, often combined with menthol, honey, or vitamin C. Provide localized antibacterial activity against pharyngeal pathogens while soothing sore throat symptoms.
- Steam Inhalation: The traditional method of respiratory eucalyptol delivery. Hot water (not boiling) in a bowl with 3–5 drops of eucalyptus essential oil, inhaled under a towel tent for 10–15 minutes. Delivers high concentrations of eucalyptol directly to the respiratory mucosa. Also available through purpose-built personal steam inhalers that control temperature and concentration.
- Ointments and Salves: Eucalyptus oil incorporated into beeswax, shea butter, or petroleum jelly-based preparations at concentrations of 2–5% for topical wound care and skin applications. Provide sustained-release antibacterial activity at the application site. May include additional herbs such as tea tree, lavender, or calendula for enhanced therapeutic effect.
- Cineole Capsules: Enteric-coated soft gelatin capsules containing purified 1,8-cineole (100 mg or 200 mg per capsule). Available as the branded product Soledum in Europe. The enteric coating prevents gastric irritation and ensures intestinal absorption. Used for systemic respiratory antibacterial and anti-inflammatory effects. Available by prescription in some countries and as dietary supplements in others.
Recommended Dosage
Inhalation Protocols
- Steam inhalation: Add 3–5 drops of eucalyptus essential oil to a bowl of hot water (approximately 70–80 degrees Celsius). Cover the head with a towel and inhale the vapor for 10–15 minutes. Repeat 2–3 times daily during acute respiratory infections. Keep eyes closed during inhalation to prevent eye irritation.
- Diffuser: Add 5–10 drops to an ultrasonic or nebulizing aromatherapy diffuser. Run for 30–60 minutes at a time in a well-ventilated room. Suitable for ambient air purification and mild respiratory support.
- Cineole capsules (oral): 200 mg of purified 1,8-cineole three times daily for acute sinusitis or bronchitis (as studied in clinical trials). 200 mg twice daily for maintenance therapy in chronic respiratory conditions. Take with meals to minimize gastrointestinal discomfort.
Topical Dilution
- General topical use: Dilute eucalyptus essential oil to 2–3% concentration in a carrier oil (such as jojoba, coconut, or sweet almond oil). This corresponds to approximately 12–18 drops of essential oil per 30 mL (1 ounce) of carrier oil.
- Wound care: Use a 1–2% dilution for application near open wounds. Consult a healthcare provider before applying to significant burns, deep wounds, or chronic ulcers.
- Muscle and joint pain: A 3–5% dilution may be used for topical analgesic applications on intact skin. Massage into the affected area 2–3 times daily.
Chest Rub Application
- Apply a generous layer of eucalyptus chest rub to the chest, throat, and upper back before bedtime.
- For daytime use, apply a thinner layer to the chest and throat area every 4–6 hours as needed.
- Do not apply to broken skin, nostrils, or mucous membranes.
- Wash hands thoroughly after application to avoid accidental contact with eyes.
Safety and Contraindications
While eucalyptus is widely considered safe when used appropriately in external and inhalation applications, several important safety considerations must be observed.
- NEVER ingest eucalyptus essential oil. Eucalyptus essential oil is toxic when taken internally. Ingestion of as little as 3.5 mL of pure eucalyptus oil has caused fatal poisoning in children, and as little as 5 mL has caused serious toxicity in adults. Symptoms of eucalyptus oil poisoning include nausea, vomiting, diarrhea, central nervous system depression, seizures, respiratory failure, and death. Only pharmaceutical-grade purified cineole in properly formulated enteric-coated capsules should ever be taken orally, and only under medical supervision. Essential oil and purified cineole capsules are entirely different preparations and must not be confused.
- Children under 6 years of age: Eucalyptus essential oil should not be applied to the face, chest, or near the nose of children under 6 years of age. Application of eucalyptus oil or mentholated products to the face of infants and young children can trigger laryngospasm and bronchospasm, potentially causing respiratory arrest. For children aged 6–12, use only products specifically formulated for pediatric use at reduced concentrations. E. radiata is generally considered safer than E. globulus for use with older children under professional guidance.
- Asthma patients: While eucalyptol has demonstrated anti-inflammatory benefits in some asthma studies, inhaled eucalyptus essential oil can trigger bronchospasm in susceptible individuals, particularly those with volatile airway hyperreactivity. Asthma patients should use eucalyptus inhalation only under medical supervision and should discontinue use immediately if wheezing, coughing, or chest tightness develops.
- Seizure history: High doses of eucalyptol and related monoterpenes can lower the seizure threshold. Individuals with epilepsy or other seizure disorders should avoid concentrated eucalyptus oil inhalation and should not take cineole capsules without explicit approval from their treating neurologist.
- Drug metabolism and CYP interactions: Eucalyptol is metabolized by cytochrome P450 enzymes, primarily CYP3A4 and CYP2B6, and can induce the activity of these enzymes. This induction can accelerate the metabolism of drugs that are substrates of the same enzyme pathways, potentially reducing their blood levels and therapeutic effectiveness. Medications at risk include certain immunosuppressants (cyclosporine, tacrolimus), anticoagulants (warfarin), anticonvulsants (carbamazepine, phenytoin), statins (atorvastatin, simvastatin), and some antidepressants and antipsychotics. Patients taking any prescription medications should consult their physician or pharmacist before using eucalyptus products, particularly oral cineole capsules.
- Pregnancy and breastfeeding: Insufficient safety data exists for eucalyptus use during pregnancy and lactation. While topical use at normal dilutions and brief steam inhalation are generally considered low-risk, oral cineole capsules should be avoided during pregnancy and breastfeeding. Pregnant women should consult their healthcare provider before using eucalyptus products.
- Skin sensitivity: Undiluted eucalyptus essential oil can cause contact dermatitis, skin irritation, and chemical burns. Always dilute to appropriate concentrations before topical application. Perform a patch test on a small area of skin 24 hours before widespread use. Discontinue use if redness, itching, or irritation develops.
Key Research Papers and References
- Sadlon, A.E. and Lamson, D.W. "Immune-modifying and antimicrobial effects of eucalyptus oil and simple inhalation devices." Alternative Medicine Review, 15(1): 33–47, 2010.
- Cermelli, C., Fabio, A., Fabio, G., and Quaglio, P. "Effect of eucalyptus essential oil on respiratory bacteria and viruses." Current Microbiology, 56(1): 89–92, 2008.
- Kehrl, W., Sonnemann, U., and Dethlefsen, U. "Therapy for acute nonpurulent rhinosinusitis with cineole: results of a double-blind, randomized, placebo-controlled trial." Laryngoscope, 114(4): 738–742, 2004.
- Juergens, U.R., Dethlefsen, U., Steinkamp, G., Gillissen, A., Repges, R., and Vetter, H. "Anti-inflammatory activity of 1,8-cineol (eucalyptol) in bronchial asthma: a double-blind placebo-controlled trial." Respiratory Medicine, 97(3): 250–256, 2003.
- Hendry, E.R., Worthington, T., Conway, B.R., and Lambert, P.A. "Antimicrobial efficacy of eucalyptus oil and 1,8-cineole alone and in combination with chlorhexidine digluconate against microorganisms grown in planktonic and biofilm cultures." Journal of Antimicrobial Chemotherapy, 64(6): 1219–1225, 2009.
- Bachir, R.G. and Benali, M. "Antibacterial activity of the essential oils from the leaves of Eucalyptus globulus against Escherichia coli and Staphylococcus aureus." Asian Pacific Journal of Tropical Biomedicine, 2(9): 739–742, 2012.
- Mulyaningsih, S., Sporer, F., Zimmermann, S., Reichling, J., and Wink, M. "Synergistic properties of the terpenoids aromadendrene and 1,8-cineole from the essential oil of Eucalyptus globulus against antibiotic-susceptible and antibiotic-resistant pathogens." Phytomedicine, 17(13): 1061–1066, 2010.
- Tyagi, A.K. and Malik, A. "Antimicrobial potential and chemical composition of Eucalyptus globulus oil in liquid and vapour phase against food spoilage microorganisms." Food Chemistry, 126(1): 228–235, 2011.
- Worth, H., Schacher, C., and Dethlefsen, U. "Concomitant therapy with cineole (eucalyptol) reduces exacerbations in COPD: a placebo-controlled double-blind trial." Respiratory Research, 10(1): 69, 2009.
- Serafino, A., Vallebona, P.S., Andreola, F., Zonfrillo, M., Mercuri, L., Federici, M., Rasi, G., Garaci, E., and Pierimarchi, P. "Stimulatory effect of eucalyptus essential oil on innate cell-mediated immune response." BMC Immunology, 9: 17, 2008.
- Trivedi, N.A. and Hotchandani, S.C. "A study of the antimicrobial activity of oil of Eucalyptus." Indian Journal of Pharmacology, 36(2): 93–95, 2004.
- Elaissi, A., Rouis, Z., Salem, N.A.B., Mabrouk, S., Salem, Y.B., Salah, K.B.H., Aouni, M., Farhat, F., Chemli, R., Harzallah-Skhiri, F., and Khouja, M.L. "Chemical composition of 8 eucalyptus species' essential oils and the evaluation of their antibacterial, antifungal and antiviral activities." BMC Complementary and Alternative Medicine, 12: 81, 2012.
Research Papers
The following PubMed topic searches aggregate the peer-reviewed literature underpinning the claims above. Each link opens a live PubMed query so the result set stays current as new research is published.
- PubMed — essential oil antimicrobial
- PubMed — 1,8-cineole eucalyptol bronchitis
- PubMed — respiratory clinical trial
- PubMed — sinusitis and rhinosinusitis
- PubMed — asthma and COPD
- PubMed — antifungal activity against Candida
- PubMed — anti-inflammatory mucolytic
- PubMed — analgesic and pain
- PubMed — insect repellent
- PubMed — systematic review
- PubMed — oil safety and toxicity
Connections
- All Herbs
- Eucalyptus Benefits Deep Dive
- Asthma
- Thyme
- Oregano
- Peppermint
- Rosemary
- Immune Boosting
- Sage
- Tea Tree
- Pneumonia
- Sinusitis
- COPD
- Tuberculosis
- Staphylococcus Aureus
- Urinary Tract Infections
- Vitamin C
- Inflammatory Markers
- Antibacterial Herbs
- Influenza
- Mullein