Tea Tree Oil for Antifungal Use & Nail Fungus
Nail fungus (onychomycosis) is one of the most frustrating dermatologic conditions to treat. The infecting organisms — Trichophyton rubrum, Trichophyton mentagrophytes, and several non-dermatophyte molds — live inside the nail plate, a hard keratin structure that conventional antifungal creams penetrate poorly. Oral terbinafine is the most effective therapy but requires 3–6 months of daily oral dosing with potential hepatotoxicity. Topical alternatives have historically been disappointing. The Buck, Nidorf & Addino 1994 Journal of Family Practice trial offered hope by comparing 100% tea tree oil applied twice daily for six months against 1% clotrimazole solution: both groups showed cure rates of approximately 18% with partial improvement in 60–70% of patients. This was modest absolute efficacy but established tea tree as essentially equivalent to the conventional topical antifungal then in use. Subsequent trials (Satchell 2002) confirmed activity against tinea pedis (athlete's foot) at 25% and 50% concentrations. Tea tree oil is a slow-but-effective topical antifungal: realistic users should plan on 6–12 months of consistent daily application for nail fungus, and 4–8 weeks for skin fungal infections.
Table of Contents
- The Buck 1994 Onychomycosis Trial vs Clotrimazole
- The Satchell 2002 Tinea Pedis Trials
- Antifungal Mechanism (Membrane Disruption + Ergosterol)
- Why Onychomycosis Is So Difficult to Treat
- The 100% Tea Tree Topical Application
- How Tea Tree Compares to Oral Terbinafine
- Athlete's Foot (Tinea Pedis) and Skin Fungal Infections
- Oral Candidiasis and Vaginal Candida
- Practical 6–12 Month Topical Regimen
- Cautions (Never Ingest, Contact Dermatitis, Pediatric)
- Key Research Papers
- Connections
- Featured Videos
The Buck 1994 Onychomycosis Trial vs Clotrimazole
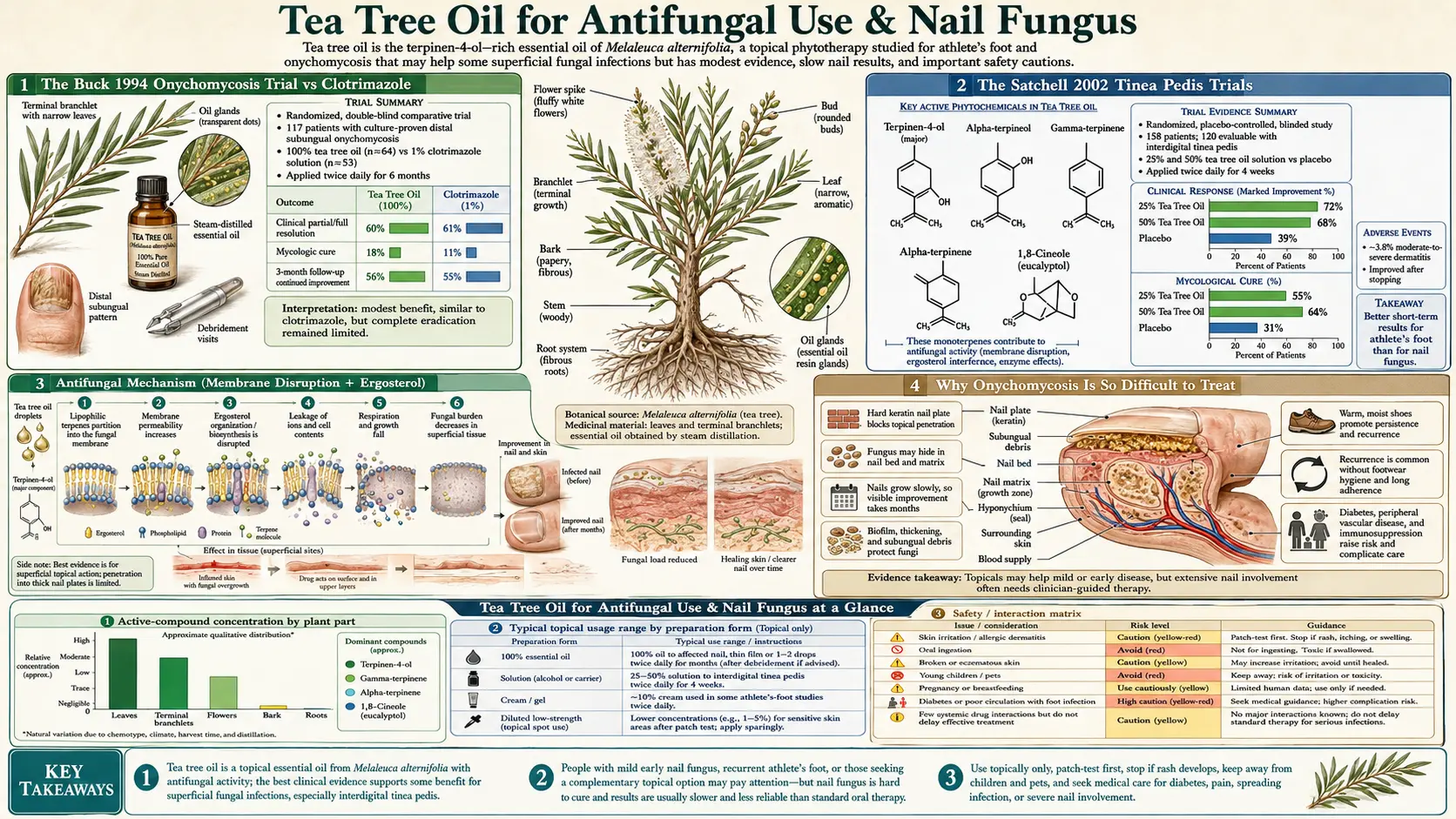
The Buck, Nidorf & Addino 1994 paper in the Journal of Family Practice is the foundational clinical trial of tea tree oil for nail fungus. The investigators randomized 117 patients with culture-proven distal subungual onychomycosis to one of two topical regimens applied twice daily for six months:
- 100% tea tree oil, applied directly to the affected nail with a cotton swab twice daily
- 1% clotrimazole solution (a standard topical azole antifungal), applied to the affected nail twice daily
The duration of treatment (six months) reflects the slow growth rate of toenails and the time needed for a non-diseased nail to grow out from the matrix and replace the infected nail. The double-blind design used identically-appearing dropper bottles with each agent.
Results at six months:
- Mycologic cure (negative KOH preparation plus negative culture) — 18% in the tea tree group, 11% in the clotrimazole group. Difference not statistically significant given the modest sample
- Clinical assessment — 60% of tea tree patients and 61% of clotrimazole patients reported either partial or full resolution of nail discoloration, thickening, and brittleness
- Adverse effects — both groups well-tolerated. Three patients in the tea tree group reported transient mild redness of the surrounding cuticle, resolving on continuation
The conclusion: tea tree oil at 100% concentration was approximately equivalent to 1% clotrimazole solution for topical management of distal subungual onychomycosis. Both produced modest absolute cure rates — reflecting the inherent difficulty of penetrating the nail plate, not any specific failure of either agent. For the patient who cannot or will not take oral antifungal therapy, tea tree was a credible alternative to clotrimazole.
The Buck trial used the maximum-concentration topical formulation (undiluted oil), which would not be tolerable on most other skin sites. The nail plate itself is keratinized and not innervated, so the high concentration produces no discomfort. The surrounding cuticle and periungual skin can develop transient irritation, addressed by careful application that minimizes spread beyond the nail surface.
The Satchell 2002 Tinea Pedis Trials
Two Satchell 2002 trials extended the tea tree antifungal evidence to tinea pedis (athlete's foot) and to oral candidiasis. The tinea pedis trial randomized 158 patients with interdigital tinea pedis to one of three preparations applied twice daily for four weeks:
- Placebo cream (vehicle control)
- 25% tea tree oil in a cream base
- 50% tea tree oil in a cream base
Results at four weeks:
- Clinical response (resolution of erythema, scaling, itching) — 39% placebo, 68% with 25% tea tree, 72% with 50% tea tree (both active arms significantly better than placebo)
- Mycologic cure — 31% placebo, 55% with 25% tea tree, 64% with 50% tea tree (50% arm significantly better than placebo; 25% arm intermediate)
- Adverse effects — transient mild irritation in 4% of 25% arm and 8% of 50% arm. No discontinuations
The companion oral candidiasis trial of 27 advanced HIV/AIDS patients used a 4-week course of 5% tea tree oral solution swish-and-spit four times daily. Clinical improvement in 60% and mycologic improvement in 33% was observed. The trial was small but demonstrated proof-of-concept for tea tree against fluconazole-refractory oral Candida.
The combined Satchell evidence established that tea tree antifungal activity translates clinically across multiple fungal infections at concentrations between 5% (oral mucosa) and 50% (skin) and 100% (nail).
Antifungal Mechanism (Membrane Disruption + Ergosterol)
Tea tree oil's antifungal mechanism extends the same membrane-disruption mechanism described in detail on the antimicrobial deep-dive, with one important addition specific to fungal cell biology.
Fungal cell membranes differ from bacterial membranes in one critical way: instead of cholesterol (the dominant sterol in animal cell membranes) or hopanoids (in many bacteria), fungal membranes contain ergosterol as their primary sterol. Ergosterol biosynthesis is the target of every major class of antifungal drug — the azoles (fluconazole, itraconazole, ketoconazole) inhibit lanosterol 14α-demethylase, the allylamines (terbinafine, naftifine) inhibit squalene epoxidase, and the polyenes (amphotericin B, nystatin) bind ergosterol directly to disrupt the membrane.
Tea tree oil's terpinen-4-ol has a slightly different mechanism. It intercalates into fungal membranes through the same biophysical disruption it uses against bacteria, but the higher ergosterol content of fungal membranes makes them somewhat more susceptible to monoterpene disruption than bacterial membranes are. The Hammer 2003 paper documented MIC values against major dermatophytes (Trichophyton mentagrophytes, T. rubrum, Microsporum canis, Epidermophyton floccosum) and yeasts (Candida albicans, C. glabrata, Cryptococcus neoformans) in the 0.03–0.5% range — even lower than the bacterial MICs.
An additional clinically interesting finding from Mertas 2015: tea tree oil shows synergy with fluconazole against fluconazole-resistant Candida albicans. The proposed mechanism is that membrane disruption by tea tree increases the intracellular concentration of fluconazole, partially restoring susceptibility in strains that had developed efflux-pump-mediated fluconazole resistance. This is potentially useful for the difficult clinical problem of fluconazole-refractory Candida in immunocompromised patients, particularly oral candidiasis in advanced HIV.
Why Onychomycosis Is So Difficult to Treat
Distal subungual onychomycosis — the most common pattern of nail fungus — involves invasion of the keratin nail plate by the dermatophyte Trichophyton rubrum. The fungus lives in and digests the nail plate, producing the characteristic yellow-brown discoloration, thickening, and crumbling that patients recognize. Several biological features make it exceptionally difficult to treat:
- The nail plate is keratin, not living tissue. Topical antifungals must diffuse through the nail plate to reach the fungus underneath, which most agents do very poorly. The nail plate is essentially a barrier
- The growth rate is slow. A toenail takes 12–18 months to grow completely from the matrix to the distal edge. Any therapy must persist long enough for new uninfected nail to replace the infected nail
- The fungus persists in the nail bed even after the nail plate clears. Recurrence after topical-only therapy is common
- The fungus produces a biofilm matrix within the nail that further reduces drug penetration
- Compliance is difficult over the 6–12+ months that any topical regimen requires. Many patients abandon therapy at the 2–3 month mark when no visible improvement is yet apparent
This is why oral therapy with terbinafine or itraconazole — which delivers the antifungal systemically and concentrates in the nail matrix — achieves substantially higher cure rates (60–80%) than any topical agent (15–30%). The trade-off is the cost (around $200–$400 for a 3-month terbinafine course), the requirement for baseline and interval liver function testing, and the small but real risk of hepatotoxicity, drug interactions, and other systemic adverse effects.
For patients who cannot take oral terbinafine (liver disease, drug interactions, pregnancy, breastfeeding, polypharmacy concerns), topical therapy remains the only option. Tea tree oil's modest absolute cure rates need to be evaluated against that comparison, not against terbinafine.
The 100% Tea Tree Topical Application
Onychomycosis is the one tea tree application where undiluted 100% oil is the standard concentration. The reasoning:
- The nail plate is the principal diffusion barrier, and the diffusion gradient is proportional to the source concentration. Higher external concentration produces higher concentration at the fungus
- The nail plate itself is keratinized and not innervated, so it does not experience the high-concentration tea tree as irritating
- Application is to a defined small area (typically one or two affected toenails), so total dose remains modest
- Twice-daily application maintains continuous concentration gradient through the application period
The practical application technique:
- Wash the foot and dry it completely. Pay particular attention to drying between the toes
- If the nail is thickened, file the surface gently with a single-use emery board to reduce thickness and improve drug penetration. Discard the emery board after use to avoid re-inoculating cleared nails
- Apply 1–2 drops of undiluted tea tree oil directly to the affected nail surface and to the proximal nail fold
- Use a cotton swab to push a small amount of oil under the distal edge of the nail if possible
- Allow to air dry; do not cover with a sock or shoe immediately
- Repeat morning and bedtime for 6–12 months continuously
The patient should expect to see no visible improvement for the first 2–3 months. Improvement appears at the proximal margin (the part of the nail closest to the cuticle, which is the newest nail emerging from the matrix). The treated nail does not become clear; it grows out clear. Patience is essential.
How Tea Tree Compares to Oral Terbinafine
Oral terbinafine 250 mg daily for 12 weeks is the current standard of care for moderate-to-severe toenail onychomycosis. Direct head-to-head comparison with tea tree oil has not been performed (and would not pass an ethics committee, given the substantial efficacy difference). Indirect comparison from separate trials:
| Parameter | Oral terbinafine | 100% tea tree oil topical |
|---|---|---|
| Mycologic cure rate | 70–76% | ~18% |
| Complete cure rate | 38–55% | ~10% |
| Duration of therapy | 12 weeks oral | 6–12 months topical |
| Cost (US) | $200–$400 generic | $15–$40 (oil) |
| Liver toxicity risk | 1:50,000–1:120,000 hepatic injury | None at topical use |
| Drug interactions | Several (CYP2D6) | None |
| Pregnancy/lactation use | Contraindicated | Limited data, generally avoided |
The clinical interpretation:
- For a patient who tolerates oral therapy and has no contraindication, oral terbinafine is the more effective choice and is what most dermatologists will recommend
- For a patient with liver disease, who is taking multiple medications, who is pregnant or breastfeeding, or who has had a previous terbinafine reaction, topical tea tree is a credible alternative with the realistic expectation of partial improvement rather than complete cure
- For a patient with mild distal disease (only the distal third of the nail involved), topical tea tree may be sufficient and avoids systemic exposure
- Combination strategies — oral terbinafine plus topical tea tree as adjunct — have not been formally studied but are biologically reasonable for severe disease
Athlete's Foot (Tinea Pedis) and Skin Fungal Infections
Tinea pedis (athlete's foot) is much easier to treat than nail fungus because the infecting dermatophyte lives in the stratum corneum of the skin, not inside the nail plate. Topical antifungals reach effective concentrations easily. Tea tree oil at 25% or 50% concentration is well-supported by the Satchell 2002 trial discussed above — clinical response rates of 68–72% and mycologic cure rates of 55–64% within four weeks of twice-daily application.
The Tong 1992 earlier trial also demonstrated efficacy for tinea pedis, though at slightly different concentrations. The 25% or 50% concentration ranges have become standard for skin fungal applications.
Other skin fungal infections amenable to tea tree topical treatment:
- Jock itch (tinea cruris) — the same dermatophytes that cause athlete's foot, infecting the groin and inner thigh. 25% tea tree cream twice daily for 4 weeks is comparable to OTC clotrimazole
- Ringworm of the body (tinea corporis) — circular scaling patches on the trunk or limbs. 25% tea tree cream similarly effective
- Pityriasis versicolor — Malassezia furfur overgrowth producing hypo- or hyperpigmented patches. Tea tree shows in vitro activity but less clinical data than dermatophyte indications
- Diaper dermatitis with Candida — topical tea tree should not be used in infants due to risk of ingestion if the area is mouthed; conventional nystatin or clotrimazole is preferred
For chronic or recurrent dermatophyte infection, broader management including foot hygiene, footwear rotation, and treatment of household contacts is needed alongside any topical agent. See our Fungal Infections page for the broader management approach.
Oral Candidiasis and Vaginal Candida
The Satchell 2002 oral candidiasis trial established that 5% tea tree oral solution (swish-and-spit, not swallowed) produced clinical and mycologic improvement in oral Candida in advanced HIV patients with fluconazole-refractory disease. Although the trial was small, it established proof-of-concept for tea tree in mucosal candidiasis.
The practical caveats:
- Tea tree oil must NEVER be swallowed. The 5% oral solution is used as a swish-and-spit only, with care to avoid ingestion
- The 5% oral solution can be irritating to the oral mucosa and is generally less well-tolerated than nystatin oral suspension
- For uncomplicated oral candidiasis in immunocompetent adults, nystatin oral suspension or oral fluconazole are the standard therapies and are preferred over tea tree
- For fluconazole-refractory oral candidiasis in immunocompromised patients, tea tree may be a useful adjunct, particularly given the Mertas 2015 evidence of tea tree-fluconazole synergy
Vaginal Candida has been less formally studied. Case series and small trials suggest activity but the data are not strong enough to displace standard fluconazole or topical azole therapy. Tea tree douching is sometimes promoted in alternative-medicine circles; we do not recommend it — the irritation potential is real, the evidence is weak, and standard treatments are highly effective.
Practical 6–12 Month Topical Regimen
For a patient with culture-confirmed mild-to-moderate distal subungual onychomycosis who has elected topical therapy:
- Obtain pharmaceutical-grade tea tree oil in a 10–30 mL amber dropper bottle. Look for ISO 4730 compliance on the label. Avoid bulk-warehouse tea tree oil of uncertain provenance and storage history
- Patch test — apply one drop to the inner forearm. Wait 24 hours. If no significant reaction develops, proceed
- Trim and file the affected nail with a single-use disposable emery board to reduce thickness and improve drug penetration. Replace the emery board weekly to avoid re-inoculation
- Apply twice daily — 1–2 drops of undiluted tea tree oil to the nail surface, the proximal nail fold, and under the distal nail edge if accessible. Allow to air dry before putting on socks or shoes
- Maintain footwear hygiene — rotate shoes daily (allow each pair to dry completely between uses), use antifungal foot powder in shoes, replace old socks and shoes that may harbor fungal spores
- Continue for 6–12 months minimum — longer for severe disease. Stopping at the first sign of improvement guarantees recurrence
- Re-evaluate at 3 and 6 months — assess for progress at the proximal margin (look for new clear nail growing in from the cuticle). If no improvement at 6 months, consider switching to oral terbinafine
- Address contributing factors — tight footwear, chronic foot moisture, immunocompromise (diabetes, HIV), and active tinea pedis elsewhere all promote recurrence. Manage these alongside the topical antifungal
For tinea pedis (skin fungal infection): use 25% or 50% tea tree in a cream base, apply twice daily for 4–6 weeks, continue for 1–2 weeks after visible resolution to prevent recurrence. Combine with rigorous foot hygiene (dry thoroughly between toes after bathing, daily sock change, dust shoes with antifungal powder).
Cautions (Never Ingest, Contact Dermatitis, Pediatric)
- NEVER ingest tea tree oil — oral ingestion produces dose-dependent CNS depression, ataxia, coma, and respiratory failure. The Morris 2003 case report of a 4-year-old boy who ingested tea tree oil required intensive care admission. The Jacobs 1994 case series documented similar adult presentations. Tea tree oil is a topical-only therapy. Keep all tea tree products out of reach of children, particularly if you have small children at home and are using tea tree for nail fungus
- Pre-pubertal boys — gynecomastia concern — Henley 2007 NEJM linked prolonged topical use of combined lavender-and-tea-tree products to reversible prepubertal gynecomastia. Causality has been re-examined and partially disputed (Hammer 2012), but the cautious recommendation is to avoid prolonged topical tea tree use on pre-pubertal boys until the question is resolved
- Allergic contact dermatitis — tea tree oil is one of the most common essential oil sensitizers. The principal sensitizing chemistry is oxidation products that accumulate in old or improperly stored oil, not the parent monoterpenes. Use fresh oil, replace within 12 months of opening, store in amber glass in a cool dark place. Discontinue if persistent redness, itching, or vesiculation develops at the application site
- Periungual irritation — the high-concentration tea tree used for nail fungus can produce transient redness and mild discomfort in the cuticle and surrounding skin. This is usually self-limited and improves with careful application that avoids excess spread beyond the nail surface. If it persists or worsens, reduce concentration to 50% in a carrier oil
- Pediatric use — tea tree oil should not be used in children under 6 years for nail fungus or tinea pedis, given the inability to prevent oral exposure and the higher pediatric sensitivity. Standard topical antifungals (clotrimazole, terbinafine cream) are preferred
- Pregnancy and breastfeeding — limited data. Topical use at standard concentrations is generally considered acceptable but should be discussed with a clinician, particularly for chronic use over 6+ months
- Diabetes and onychomycosis — patients with diabetes are at high risk for secondary bacterial infection of fungal-affected toenails. They should have podiatry care alongside any antifungal therapy. Topical-only therapy may be inadequate for moderate-severe disease in diabetic patients; oral terbinafine is often preferred despite the additional monitoring
- Pet safety — tea tree oil is highly toxic to cats and dogs even at dilute concentrations. Do not use tea tree oil on or around pets
Key Research Papers
- Buck DS, Nidorf DM, Addino JG (1994). Comparison of two topical preparations for the treatment of onychomycosis: Melaleuca alternifolia (tea tree) oil and clotrimazole. Journal of Family Practice. — PubMed
- Tong MM, Altman PM, Barnetson RS (1992). Tea tree oil in the treatment of tinea pedis. Australasian Journal of Dermatology. — PubMed
- Satchell AC, Saurajen A, Bell C, Barnetson RS (2002). Treatment of interdigital tinea pedis with 25% and 50% tea tree oil solution: a randomized, placebo-controlled, blinded study. Australasian Journal of Dermatology. — PubMed
- Satchell AC, Saurajen A, Bell C, Barnetson RS (2002). Treatment of oropharyngeal candidiasis with topical Melaleuca oil (tea tree oil): a randomized, controlled trial. Journal of the American Academy of Dermatology. — PubMed
- Hammer KA, Carson CF, Riley TV (2003). Antifungal activity of the components of Melaleuca alternifolia (tea tree) oil. Journal of Applied Microbiology. — PubMed
- Hammer KA, Carson CF, Riley TV (2002). In vitro activity of Melaleuca alternifolia oil against dermatophytes and other filamentous fungi. Journal of Antimicrobial Chemotherapy. — PubMed
- Mertas A, Garbusińska A, Szlißka E, Jureczko P, Kowalska M, Krol W (2015). The influence of tea tree oil on antifungal activity and pharmacokinetic properties of fluconazole. BioMed Research International. — PubMed
- Nenoff P, Haustein UF, Brandt W (1996). Antifungal activity of the essential oil of Melaleuca alternifolia (tea tree oil) against pathogenic fungi in vitro. Skin Pharmacology. — PubMed
- Concha JM, Moore LS, Holloway WJ (1998). Antifungal activity of Melaleuca alternifolia (tea tree) oil against various pathogenic organisms. Journal of the American Podiatric Medical Association. — PubMed
- Hammer KA, Carson CF, Riley TV (2004). Antifungal effects of Melaleuca alternifolia (tea tree) oil and its components on Candida albicans, C. glabrata and Saccharomyces cerevisiae. Journal of Antimicrobial Chemotherapy. — PubMed
- Morris MC, Donoghue A, Markowitz JA, Osterhoudt KC (2003). Ingestion of tea tree oil (Melaleuca oil) by a 4-year-old boy. Pediatric Emergency Care. — PubMed
- Hammer KA, Carson CF, Riley TV, Nielsen JB (2006). A review of the toxicity of Melaleuca alternifolia (tea tree) oil. Food and Chemical Toxicology. — PubMed
PubMed Topic Searches
- PubMed: Tea tree onychomycosis
- PubMed: Tea tree tinea pedis
- PubMed: Tea tree Candida
- PubMed: Terpinen-4-ol antifungal mechanism
- PubMed: Tea tree + fluconazole synergy
Connections
- Tea Tree Overview
- Tea Tree Benefits Hub
- Tea Tree for MRSA
- Tea Tree for Acne
- Tea Tree for Head Lice
- Fungal Infections
- Antibacterial Herbs
- Oregano
- Thyme
- Garlic
- Olive Leaf
- Eucalyptus
- Eczema
- Psoriasis
- Silver Nanoparticles
- All Herbs