Manuka Honey (Leptospermum scoparium)
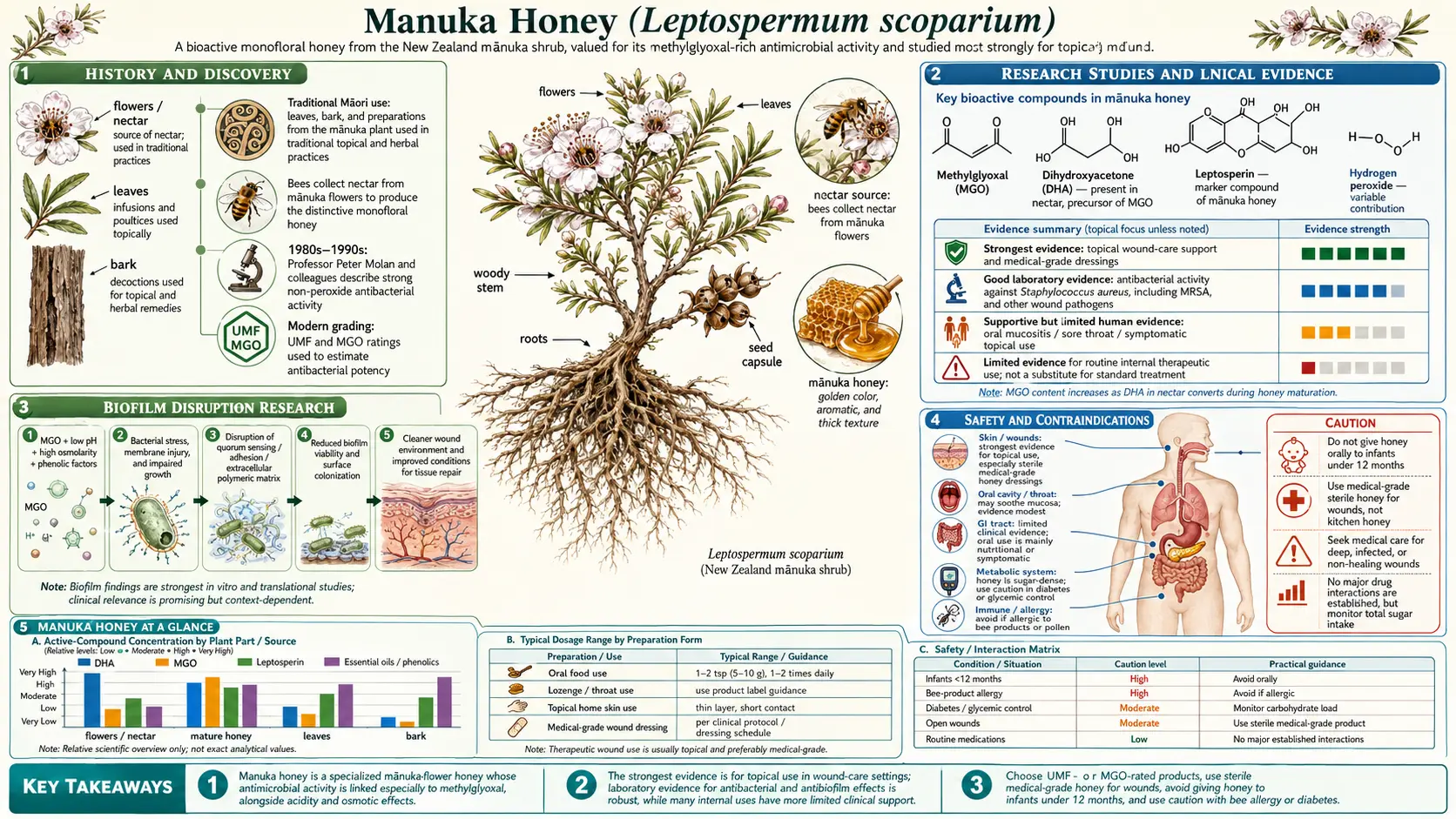

Table of Contents
- History and Discovery
- What Makes Manuka Unique
- Key Antibacterial Compounds
- UMF and MGO Grading Systems
- Mechanism of Antibacterial Action
- Bacteria Targeted
- Research Studies and Clinical Evidence
- MRSA and Hospital Wound Care
- Wound Healing Applications
- Gastrointestinal Uses
- Oral Health
- Biofilm Disruption Research
- Synergistic Effects
- Other Health Benefits
- How to Choose Quality Manuka Honey
- Forms and Applications
- Recommended Usage
- Safety and Contraindications
- Key Research Papers and References
- Featured Videos
History and Discovery
Manuka honey is made by introduced honeybees (Apis mellifera) from the nectar of the manuka bush (Leptospermum scoparium), a New Zealand shrub whose leaves, bark, and gum were used in traditional Māori medicine (rongoā) long before the honey itself drew any scientific attention. The honey's modern reputation dates to 1981, when University of Waikato biochemist Peter Molan found it carried a stable, non-peroxide antibacterial activity that ordinary honeys lacked — a property explained in 2008 when a German team identified methylglyoxal (MGO) as the active compound. — the fuller story is told in the dedicated History & Traditional Use article.
What Makes Manuka Unique
All raw honeys possess some degree of antibacterial activity, primarily derived from the enzymatic production of hydrogen peroxide by the bee-added enzyme glucose oxidase. However, this hydrogen peroxide activity is easily destroyed by heat, light exposure, and the catalase enzyme present in blood and wound tissues, severely limiting its clinical usefulness. Manuka honey distinguishes itself from all other honeys through its potent non-peroxide antibacterial activity, a property that remains stable and effective under conditions that would neutralize the antimicrobial action of conventional honeys.
The Unique Manuka Factor, or UMF, is the trademark term established to describe and quantify this distinctive non-peroxide antibacterial activity. The UMF grading system was originally developed by Professor Peter Molan and later adopted by the UMF Honey Association of New Zealand as an industry standard. The UMF rating compares the antibacterial potency of a given batch of manuka honey against a standard antiseptic solution of phenol. A UMF rating of 10, for example, indicates that the honey has equivalent antibacterial activity to a 10 percent phenol solution. This standardized comparison allows consumers and clinicians to select honey with verified therapeutic potency.
The key compound responsible for the non-peroxide activity is methylglyoxal, commonly abbreviated as MGO. Methylglyoxal is a naturally occurring alpha-dicarbonyl compound that forms in manuka honey through the non-enzymatic conversion of dihydroxyacetone (DHA), a substance found in high concentrations in the nectar of Leptospermum scoparium flowers. While DHA is present in the fresh nectar, it slowly converts to MGO over time during the honey's maturation, a process that continues for several months after the honey is harvested. This explains why freshly extracted manuka honey may initially test at lower MGO levels than the same batch measured months later.
The MGO concentrations found in manuka honey are extraordinary compared to other honeys. While conventional honeys typically contain MGO levels of 1 to 10 milligrams per kilogram, manuka honey can contain concentrations ranging from 83 to over 1,000 milligrams per kilogram. These concentrations are sufficient to inhibit the growth of a wide range of pathogenic bacteria, including antibiotic-resistant strains. No other commercially available honey in the world contains MGO at comparable concentrations, making manuka honey truly singular in its antibacterial potency.
Beyond MGO, manuka honey contains a complex matrix of bioactive compounds that contribute to its overall therapeutic profile. These include leptosperin, a naturally occurring glycoside unique to Leptospermum nectar that serves as an authenticity marker, as well as various phenolic acids, flavonoids, and other phytochemicals derived from the manuka plant. The synergistic interaction of these compounds creates an antibacterial effect greater than what MGO alone would produce, suggesting that the whole honey matrix is more therapeutically effective than any single isolated component.
Key Antibacterial Compounds
The antibacterial potency of manuka honey arises from a complex interplay of multiple bioactive compounds, each contributing distinct mechanisms of microbial inhibition. Understanding these individual components and their interactions is essential for appreciating why manuka honey is such an effective antimicrobial agent.
Methylglyoxal (MGO) is the dominant antibacterial compound in manuka honey and the primary driver of its non-peroxide activity. MGO is a reactive dicarbonyl compound with the molecular formula C3H4O2. It exerts its antibacterial effects by modifying bacterial proteins and DNA through glycation reactions, forming advanced glycation end-products (AGEs) that disrupt essential cellular functions. MGO cross-links with amino acid residues in bacterial proteins, particularly arginine and lysine, causing structural deformation and loss of enzymatic function. This mechanism is fundamentally different from conventional antibiotics, which target specific metabolic pathways, making it extremely difficult for bacteria to develop resistance. MGO concentrations in high-grade manuka honey can exceed 800 milligrams per kilogram, providing potent bactericidal activity.
Hydrogen peroxide is produced enzymatically in all raw honeys through the action of glucose oxidase, an enzyme added by the bees during honey production. When honey is diluted, glucose oxidase catalyzes the oxidation of glucose to gluconic acid, generating hydrogen peroxide as a byproduct. In manuka honey, this hydrogen peroxide activity operates alongside and in addition to the MGO-mediated non-peroxide activity, creating a dual antimicrobial system. The hydrogen peroxide generated is produced at low, sustained concentrations that are effective against bacteria but gentle enough not to cause tissue damage, unlike the concentrated hydrogen peroxide solutions used in conventional antiseptics.
Bee defensin-1 is an antimicrobial peptide produced in the hypopharyngeal glands of honeybees and secreted into the honey during production. This cationic peptide belongs to the defensin family of innate immune molecules and exhibits broad-spectrum activity against Gram-positive bacteria by disrupting bacterial cell membranes. Research published by Kwakman and colleagues in 2010 in the FASEB Journal demonstrated that bee defensin-1 contributes meaningfully to the total antibacterial activity of honey, particularly against Staphylococcus aureus and Bacillus subtilis. The peptide works synergistically with MGO and hydrogen peroxide, enhancing the overall antimicrobial effect of manuka honey beyond what any single compound achieves alone.
Leptosperin is a methyl syringate glycoside found exclusively in honey derived from Leptospermum species. While leptosperin itself does not exhibit strong direct antibacterial activity, it serves as a crucial authenticity marker for genuine manuka honey and may contribute to the honey's anti-inflammatory and antioxidant properties. The presence and concentration of leptosperin can be used to verify that honey is genuinely derived from manuka nectar rather than being adulterated or mislabeled. The New Zealand Ministry for Primary Industries has included leptosperin testing as part of its official manuka honey authentication standards.
Dihydroxyacetone (DHA) conversion is the biochemical process that gives rise to the high MGO levels in manuka honey. DHA is a simple three-carbon sugar compound present at exceptionally high concentrations in the nectar of Leptospermum scoparium flowers. After bees collect the nectar and process it into honey, DHA undergoes a slow, non-enzymatic Maillard-type conversion to MGO. This reaction continues over weeks and months, meaning that manuka honey's MGO levels and corresponding antibacterial potency increase with age during the first year or so after harvest. The rate of conversion depends on temperature and storage conditions, with moderate warmth accelerating the process. This natural chemical transformation is unique to manuka honey and is the fundamental reason for its extraordinary MGO concentrations.
Additional bioactive compounds in manuka honey include methyl syringate, which has demonstrated anti-inflammatory effects; various phenolic acids such as gallic acid, caffeic acid, and p-coumaric acid, which contribute antioxidant capacity; and flavonoids including pinobanksin, pinocembrin, and chrysin. The acidic pH of manuka honey, typically between 3.2 and 4.5, also contributes to its antibacterial action by creating an inhospitable environment for many pathogenic bacteria. The combined effect of all these components creates a multi-target antimicrobial system that is remarkably difficult for bacteria to overcome.
UMF and MGO Grading Systems
The therapeutic value of manuka honey varies enormously between batches, making standardized grading systems essential for both clinical use and consumer protection. Two primary grading systems are used internationally: the Unique Manuka Factor (UMF) system and the Methylglyoxal (MGO) system. Understanding these ratings is crucial for selecting manuka honey with verified antibacterial potency.
The UMF grading system was the first standardized measurement developed for manuka honey. Established by the UMF Honey Association (UMFHA) in New Zealand, this system rates the antibacterial strength of manuka honey by comparing it to the antiseptic activity of phenol (carbolic acid). A UMF rating of 15 means the honey has equivalent antibacterial activity to a 15 percent phenol solution when tested against Staphylococcus aureus in laboratory agar well diffusion assays. The modern UMF grading evaluates four key chemical markers: MGO content, leptosperin levels, DHA concentration, and hydroxymethylfurfural (HMF) levels. HMF is measured as a freshness indicator, since elevated HMF levels indicate heat damage or prolonged storage. Only licensed producers who submit to independent third-party laboratory testing by accredited facilities can carry the UMF trademark.
UMF ratings are typically categorized into functional tiers. Honey rated UMF 5+ is considered low-activity and is suitable primarily as a general wellness food. UMF 10+ marks the threshold for therapeutic-grade honey with meaningful antibacterial properties. UMF 15+ is considered high-activity and is recommended for active wound care and medicinal use. UMF 20+ and above represents premium, exceptionally potent honey with the highest antibacterial activity. Some rare batches achieve UMF 25+ or even UMF 28+, commanding premium prices due to their scarcity and extraordinary potency.
The MGO grading system provides a more direct chemical measurement by specifying the exact concentration of methylglyoxal in milligrams per kilogram of honey. This system was developed following Professor Thomas Henle's identification of MGO as the primary non-peroxide antibacterial compound. The MGO rating gives consumers a precise, quantitative measure of the key active ingredient rather than a relative biological activity comparison. Common MGO ratings include MGO 83+ (equivalent to approximately UMF 5+), MGO 263+ (approximately UMF 10+), MGO 514+ (approximately UMF 15+), and MGO 829+ (approximately UMF 20+).
For therapeutic applications, a minimum grade of UMF 10+ or MGO 263+ is generally recommended. Research has consistently shown that honey below these thresholds does not reliably demonstrate clinically significant antibacterial activity. For active wound management, infection control, and treatment of antibiotic-resistant organisms, many clinicians recommend UMF 15+ (MGO 514+) or higher. Professor Molan's research suggested that the minimum inhibitory concentrations needed to suppress common wound pathogens correspond to UMF ratings of 12 to 15 in most clinical scenarios.
The approximate equivalencies between the two systems are as follows: UMF 5+ corresponds to MGO 83+, UMF 10+ to MGO 263+, UMF 12+ to MGO 356+, UMF 15+ to MGO 514+, UMF 18+ to MGO 696+, UMF 20+ to MGO 829+, and UMF 25+ to MGO 1200+. These correlations are approximate because UMF incorporates multiple markers beyond MGO alone, meaning that two honeys with identical MGO levels could differ slightly in their UMF ratings depending on their leptosperin and DHA profiles.
Mechanism of Antibacterial Action
Manuka honey kills and inhibits bacteria through multiple simultaneous mechanisms, creating a multi-pronged assault that makes bacterial resistance development extremely unlikely. This multi-target approach is fundamentally different from conventional antibiotics, which typically act on a single molecular target and are therefore vulnerable to resistance mutations.
Osmotic dehydration is one of the most immediate antibacterial mechanisms of honey. All honeys are supersaturated sugar solutions containing approximately 80 percent sugars by weight, predominantly fructose and glucose. This extremely high sugar concentration creates powerful osmotic pressure that draws water out of bacterial cells through their semi-permeable membranes. The resulting cellular dehydration disrupts metabolic processes, collapses turgor pressure, and ultimately causes bacterial death through plasmolysis. This osmotic effect is particularly relevant when manuka honey is applied undiluted to wound surfaces, where it creates a hostile, water-depleted microenvironment that bacteria cannot survive in.
Low pH contributes significantly to the antibacterial environment created by manuka honey. With a pH typically ranging from 3.2 to 4.5, manuka honey is markedly acidic. Most pathogenic bacteria, including common wound pathogens like Staphylococcus aureus and Pseudomonas aeruginosa, require near-neutral pH conditions (6.5 to 7.5) for optimal growth. The acidic environment of manuka honey disrupts bacterial enzyme function, destabilizes cell membranes, and inhibits essential metabolic pathways. When applied to chronic wounds, which are often alkaline with pH values above 7.0, manuka honey lowers the wound pH toward the mildly acidic range (5.5 to 6.5) that is optimal for tissue healing and hostile to bacterial colonization.
MGO-mediated protein cross-linking represents the most distinctive antibacterial mechanism of manuka honey. Methylglyoxal reacts with amino acid residues in bacterial proteins through a process known as glycation, forming covalent cross-links that alter protein structure and destroy enzymatic function. MGO preferentially targets arginine residues through the formation of hydroimidazolone adducts and lysine residues through the formation of carboxyethyllysine. These modifications affect structural proteins, transport proteins, and metabolic enzymes across the bacterial cell, causing widespread functional disruption. Research has shown that MGO can also react with bacterial DNA, causing strand breaks and base modifications that impair replication and transcription. Because MGO simultaneously attacks multiple protein and nucleic acid targets throughout the bacterial cell, the probability of a bacterium acquiring resistance through random mutation is vanishingly small.
Biofilm disruption is one of the most clinically significant antibacterial mechanisms of manuka honey. Biofilms are structured microbial communities encased in a self-produced extracellular polymeric substance (EPS) matrix that adheres to surfaces such as wound beds, implants, and mucosal tissues. Bacteria within biofilms are notoriously resistant to antibiotics, often requiring 100 to 1,000 times the antibiotic concentration needed to kill their planktonic (free-floating) counterparts. Manuka honey has been shown to penetrate and disrupt established biofilms through several mechanisms. MGO degrades the structural proteins and polysaccharides of the EPS matrix, weakening biofilm architecture. The osmotic activity of the honey draws water from the biofilm, causing structural collapse. Additionally, manuka honey has been shown to inhibit quorum sensing, the cell-to-cell communication system that bacteria use to coordinate biofilm formation and maintenance.
Wound healing cascade activation extends manuka honey's benefits beyond direct bacterial killing. Research has demonstrated that manuka honey stimulates multiple aspects of the wound healing process. It promotes macrophage activation and cytokine release, enhancing the innate immune response at the wound site. It stimulates angiogenesis, the formation of new blood vessels necessary for tissue regeneration. Manuka honey promotes fibroblast proliferation and collagen synthesis, accelerating granulation tissue formation and wound closure. The honey also maintains a moist wound environment conducive to healing while simultaneously preventing the wound bed from becoming waterlogged through its osmotic properties. Furthermore, the anti-inflammatory effects of manuka honey reduce excessive inflammation that can delay healing in chronic wounds, creating an environment that supports orderly tissue repair.
Bacteria Targeted
Manuka honey has demonstrated antibacterial activity against a remarkably broad spectrum of pathogenic organisms in laboratory studies and clinical settings. Its multi-target mechanism of action makes it effective against both Gram-positive and Gram-negative bacteria, including several species that have developed resistance to conventional antibiotics.
Staphylococcus aureus, including methicillin-resistant Staphylococcus aureus (MRSA), is perhaps the most extensively studied target of manuka honey. S. aureus is the most common cause of wound infections worldwide and a leading cause of healthcare-associated infections. MRSA strains carry the mecA gene, which confers resistance to all beta-lactam antibiotics, making infections extremely difficult to treat. Multiple studies have demonstrated that manuka honey inhibits and kills MRSA at concentrations achievable in clinical wound applications. Crucially, research has shown that S. aureus does not develop resistance to manuka honey even after repeated sub-inhibitory exposure over extended periods, in stark contrast to its rapid development of resistance to conventional antibiotics.
Escherichia coli is a Gram-negative bacterium responsible for urinary tract infections, wound infections, and gastrointestinal illness. Manuka honey has shown consistent inhibitory activity against multiple strains of E. coli, including extended-spectrum beta-lactamase (ESBL) producing strains that are resistant to many antibiotics. The minimum inhibitory concentrations of manuka honey against E. coli have been reported in the range of 6 to 25 percent volume-to-volume in laboratory studies.
Pseudomonas aeruginosa is a notorious opportunistic pathogen that causes chronic wound infections, burn wound sepsis, ventilator-associated pneumonia, and catheter-related infections. P. aeruginosa is intrinsically resistant to many antibiotics and is a prolific biofilm former, making it one of the most challenging organisms in clinical medicine. Research has demonstrated that manuka honey is effective against P. aeruginosa, including multidrug-resistant strains, and can disrupt established P. aeruginosa biofilms that are impervious to antibiotic therapy.
Streptococcus pyogenes (Group A Streptococcus) causes strep throat, cellulitis, impetigo, necrotizing fasciitis, and other invasive infections. Studies have shown that manuka honey effectively inhibits S. pyogenes growth, supporting its traditional use for sore throat and its modern application in wound care for streptococcal skin infections.
Helicobacter pylori is the bacterium responsible for most peptic ulcers and chronic gastritis, and it is a recognized carcinogen linked to gastric cancer. Research by Al Somal and colleagues, published in collaboration with Professor Molan, demonstrated that manuka honey inhibits H. pylori growth at concentrations as low as 5 percent volume-to-volume. This finding supports the traditional use of manuka honey for digestive complaints and has sparked interest in its potential role as an adjunct therapy in H. pylori eradication regimens.
Clostridioides difficile (formerly Clostridium difficile) causes severe antibiotic-associated diarrhea and life-threatening pseudomembranous colitis, particularly in hospitalized and elderly patients. Research has shown that manuka honey inhibits both the vegetative cells and the spore germination of C. difficile, making it a potential adjunct to standard C. difficile treatment protocols.
Additional bacteria against which manuka honey has demonstrated activity include Enterococcus faecalis (including vancomycin-resistant enterococci, VRE), Acinetobacter baumannii (a major cause of multidrug-resistant hospital infections), Klebsiella pneumoniae, Proteus mirabilis, Streptococcus mutans (the primary cause of dental caries), Porphyromonas gingivalis (implicated in periodontal disease), and Burkholderia cepacia complex organisms (problematic in cystic fibrosis patients). The breadth of this activity spectrum underscores the non-specific, multi-target nature of manuka honey's antibacterial mechanisms.
Research Studies and Clinical Evidence
The scientific evidence supporting manuka honey's antibacterial properties spans more than three decades of laboratory research, animal studies, and clinical trials. The body of published literature has grown substantially since Professor Molan's pioneering work in the 1990s, with hundreds of peer-reviewed papers now documenting its antimicrobial efficacy and clinical applications.
The Wound Care journal has published numerous studies evaluating manuka honey in clinical wound management. A randomized controlled trial by Jull and colleagues (2008) examined the use of manuka honey dressings on venous leg ulcers in 368 patients across multiple New Zealand hospitals. While the study found that honey-treated ulcers did not heal significantly faster than those receiving standard care, it confirmed that manuka honey was safe, well-tolerated, and effective at reducing wound odor and bacterial burden. A subsequent systematic review by Jull et al. (2015) in the Cochrane Database of Systematic Reviews concluded that honey appeared to be effective for partial-thickness burns and infected post-operative wounds, while acknowledging that more high-quality randomized trials were needed.
PLOS ONE has published several important studies on manuka honey's antimicrobial mechanisms. A study by Jervis-Bardy and colleagues (2011) demonstrated that manuka honey was effective at killing Staphylococcus aureus in established biofilms on sinus mucosa tissue from patients with chronic rhinosinusitis, suggesting applications in ENT medicine. Lu and colleagues (2013) published research in PLOS ONE showing that manuka honey killed bacteria through multiple mechanisms simultaneously, including membrane disruption, metabolic inhibition, and cell lysis, confirming the multi-target hypothesis that explains the absence of resistance development.
Frontiers in Microbiology has featured research exploring the molecular mechanisms of manuka honey's antibacterial action. Carter and colleagues (2016) published a comprehensive study demonstrating that manuka honey inhibited the cell division of S. aureus by disrupting the bacterial cytoskeletal protein FtsZ, leading to incomplete septum formation and cell lysis. This finding revealed a previously unknown mechanism of action distinct from the MGO-mediated protein glycation pathway. Johnston and colleagues (2018) published in the same journal demonstrating that manuka honey downregulated genes involved in S. aureus virulence factor expression, effectively disarming the bacteria's pathogenic toolkit even at sub-lethal concentrations.
Professor Molan's research at the University of Waikato established the foundational knowledge of manuka honey's antibacterial properties. His early publication with colleague Russell (1988) in the Journal of Applied Bacteriology first documented the non-peroxide antibacterial activity of manuka honey. Molan's 1992 review paper, "The Antibacterial Activity of Honey," published in Bee World, became one of the most cited papers in honey research. His 2001 paper in the Journal of Wound Care systematically reviewed the clinical evidence for honey in wound management and was instrumental in shifting medical opinion toward accepting honey as a legitimate wound care agent. Molan's body of work, comprising over 80 published papers, created the scientific framework upon which all subsequent manuka honey research has been built.
Other significant contributions include the work of Mavric and colleagues (2008) at the Technical University of Dresden, who published the identification of MGO as the key antibacterial compound in Molecular Nutrition and Food Research. Cooper and colleagues at the University of Wales Institute Cardiff published extensively through the 2000s and 2010s on manuka honey's activity against wound pathogens, particularly MRSA and other antibiotic-resistant organisms. Their work in the Journal of Clinical Pathology (2002) provided some of the earliest clinical evidence that manuka honey could kill MRSA in actual wound specimens.
MRSA and Hospital Wound Care
The emergence and global spread of methicillin-resistant Staphylococcus aureus (MRSA) represents one of the most serious threats in modern infectious disease medicine. MRSA infections cause an estimated 120,000 deaths globally each year, with particularly devastating impact in hospital and long-term care settings where vulnerable patients are at highest risk. The ability of manuka honey to kill MRSA has been one of the most important and clinically impactful findings in the field of natural antimicrobials.
Medihoney is a medical-grade manuka honey product that received clearance from the United States Food and Drug Administration (FDA) in 2007 for use in wound management. Produced by Derma Sciences (now part of Integra LifeSciences), Medihoney is standardized to contain consistent levels of antibacterial activity and is gamma-irradiated for sterility without compromising its bioactive compounds. The FDA clearance was a watershed moment for manuka honey, transitioning it from an alternative remedy to a recognized medical device with regulatory approval. Medihoney is available in several formulations, including an antibacterial wound gel, calcium alginate dressings, adhesive dressings, and paste, each designed for different wound types and clinical applications.
Clinical studies using manuka honey in hospital wound care have demonstrated impressive results. A study by Blaser and colleagues (2007), published in the journal Wounds, documented the successful treatment of MRSA-infected chronic wounds in ten patients using medical-grade manuka honey after conventional antibiotic treatments had failed. All wounds achieved bacteriological clearance of MRSA, and seven of ten wounds healed completely. Natarajan and colleagues (2001) reported in the Journal of Dermatological Treatment that manuka honey dressings successfully eradicated MRSA from chronic venous ulcers in patients where mupirocin, the standard topical anti-MRSA agent, had failed.
The United Kingdom's National Health Service (NHS) has been at the forefront of adopting manuka honey in clinical practice. Several NHS hospital trusts, including the University Hospital of Wales and Waikato Hospital, have incorporated medical-grade manuka honey products into their wound care formularies. The National Institute for Health and Care Excellence (NICE) has acknowledged honey-based wound products in its evidence summaries. Clinical nurse specialists in tissue viability across the NHS have published numerous case studies documenting successful outcomes with manuka honey in wounds that had failed to respond to months or years of conventional treatment, including MRSA-infected pressure ulcers, surgical wound dehiscences, and chronic leg ulcers.
One of the most compelling aspects of manuka honey's anti-MRSA activity is the consistent finding that MRSA does not develop resistance to it. Blair and colleagues (2009) published research in the International Journal of Antimicrobial Agents demonstrating that S. aureus, including MRSA strains, showed no reduction in sensitivity to manuka honey even after prolonged exposure at sub-inhibitory concentrations over multiple passages. This contrasts sharply with the rapid emergence of resistance seen when bacteria are similarly exposed to sub-inhibitory concentrations of conventional antibiotics, and it underscores the therapeutic advantage of the multi-target antibacterial mechanism of manuka honey.
Wound Healing Applications
The clinical application of manuka honey in wound healing extends across a diverse range of wound types and severities, from minor abrasions to complex chronic wounds that have resisted conventional treatments for months or years. The honey's combination of antibacterial activity, anti-inflammatory effects, and wound healing stimulation makes it uniquely suited to address the multiple factors that contribute to impaired wound healing.
Burns represent one of the most well-established applications for manuka honey in wound care. Honey has been used to treat burns since ancient times, and modern clinical evidence strongly supports its efficacy. A meta-analysis by Wijesinghe and colleagues (2009), published in Burns, analyzed five randomized controlled trials involving 519 patients and found that honey-treated superficial and partial-thickness burns healed significantly faster than those treated with conventional dressings, including silver sulfadiazine, the standard-of-care topical burn treatment. Mean healing times were 4 to 5 days shorter with honey treatment. Manuka honey provides an optimal moist wound environment for burn healing, reduces pain during dressing changes by preventing gauze adherence, controls infection without the cytotoxic effects of silver-based agents, and minimizes hypertrophic scarring.
Surgical wounds, including those complicated by dehiscence or infection, respond favorably to manuka honey treatment. Al-Waili and Saloom (1999) published early clinical evidence of honey's effectiveness in post-operative wound management. Studies on caesarean section wound infections, pilonidal sinus surgery, and Fournier's gangrene debridement have all documented positive outcomes with manuka honey dressings. The honey reduces the risk of surgical site infections when used prophylactically and accelerates healing of infected wounds that have undergone secondary closure.
Diabetic ulcers are among the most challenging chronic wounds in clinical medicine, with impaired healing driven by neuropathy, peripheral vascular disease, hyperglycemia, and chronic inflammation. Manuka honey addresses multiple factors in the diabetic wound healing cascade. It controls bacterial burden in the ischemic, poorly perfused wound bed where systemic antibiotics cannot reach therapeutic concentrations. It modulates the excessive inflammatory response characteristic of diabetic wounds. It promotes angiogenesis and granulation tissue formation in tissue with compromised blood supply. Several case series have documented successful healing of diabetic foot ulcers that had been unresponsive to weeks or months of conventional treatment after the introduction of medical-grade manuka honey dressings.
Pressure sores (pressure ulcers, decubitus ulcers) are chronic wounds caused by sustained pressure on tissues overlying bony prominences, most commonly affecting immobile patients. These wounds are frequently colonized with biofilm-forming organisms and are among the most difficult to heal. Clinical reports have documented the successful use of manuka honey in stage II, III, and IV pressure ulcers, with honey dressings promoting debridement of necrotic tissue, controlling malodorous bacterial overgrowth, and stimulating the formation of healthy granulation tissue in prepared wound beds.
Skin grafts benefit from manuka honey's dual role as an antimicrobial and wound healing promoter. Honey dressings can be applied to both the graft donor site and the recipient site. At the donor site, manuka honey accelerates re-epithelialization and reduces pain and infection risk. At the recipient site, the honey's antibacterial properties help prevent graft infection, one of the leading causes of graft failure, while its promotion of angiogenesis supports the vascularization necessary for graft take.
Gastrointestinal Uses
The internal consumption of manuka honey for gastrointestinal conditions represents a growing area of clinical interest, building on centuries of traditional use of honey for digestive complaints. The antibacterial, anti-inflammatory, and mucosal-protective properties of manuka honey make it a compelling complementary agent for several gastrointestinal disorders.
Helicobacter pylori infection affects approximately half of the world's population and is the primary cause of peptic ulcer disease, chronic gastritis, and a significant risk factor for gastric adenocarcinoma and gastric mucosa-associated lymphoid tissue (MALT) lymphoma. Standard eradication therapy involves triple or quadruple antibiotic regimens that are associated with significant side effects and declining success rates due to increasing antibiotic resistance. Research by Al Somal and colleagues (1994) demonstrated that manuka honey inhibited H. pylori growth at concentrations of 5 percent volume-to-volume, while McGovern and colleagues (1999) showed in vitro susceptibility of H. pylori clinical isolates to manuka honey. While manuka honey is unlikely to eradicate established H. pylori infection as a monotherapy, its use as an adjunct to standard eradication regimens may improve success rates and reduce gastrointestinal side effects.
Gastritis and acid reflux symptoms may be ameliorated by the mucosal-protective properties of manuka honey. The honey coats and soothes inflamed gastric and esophageal mucosa, providing a physical barrier against acid irritation. Its anti-inflammatory compounds reduce mucosal inflammation, while its antibacterial activity helps control bacterial overgrowth that can exacerbate gastric inflammation. Traditional practitioners have long recommended consuming a tablespoon of manuka honey on an empty stomach or before meals to soothe gastric symptoms, and while large-scale clinical trials are lacking, the mechanistic rationale and anecdotal evidence are substantial.
Oral mucositis is a debilitating condition characterized by painful inflammation and ulceration of the oral and gastrointestinal mucosa, most commonly occurring as a side effect of chemotherapy and radiation therapy for cancer. It affects up to 80 percent of head and neck cancer patients receiving radiation therapy and can be severe enough to require opioid pain management, feeding tube placement, and treatment interruptions. Several clinical trials have investigated manuka honey for the prevention and treatment of oral mucositis. Hawley and colleagues (2014) published a pilot study demonstrating that topical application of manuka honey reduced the severity and duration of radiation-induced oral mucositis. A randomized controlled trial by Jayachandran and Balaji (2012) found that honey application significantly reduced oral mucositis severity in patients undergoing radiation therapy for head and neck cancers compared to conventional treatment.
Sore throat is one of the most common traditional uses of honey, and manuka honey's enhanced antibacterial properties make it particularly effective for this application. The honey coats the inflamed pharyngeal mucosa, providing demulcent relief from irritation and pain. Its antibacterial activity targets Streptococcus pyogenes and other common pharyngeal pathogens. The anti-inflammatory compounds reduce mucosal swelling and edema. Clinical surveys consistently report subjective improvement in sore throat symptoms with manuka honey consumption, and its use as a soothing agent is recognized even by conventional medical practitioners.
Oral Health
The application of manuka honey in oral health may seem counterintuitive given that sugar is universally associated with dental disease. However, research has demonstrated that manuka honey's antibacterial properties, particularly its activity against oral pathogens, can actually benefit oral health when used appropriately. The key distinction is that the antibacterial compounds in manuka honey inhibit the acid-producing bacteria that cause dental disease, even though the honey itself contains sugars.
Dental plaque is a biofilm composed primarily of Streptococcus mutans and other acidogenic bacteria that adhere to tooth surfaces. S. mutans metabolizes dietary sugars to produce lactic acid, which demineralizes tooth enamel and initiates the caries process. Research by Badet and Quero (2011) demonstrated that manuka honey significantly inhibited the growth of S. mutans and reduced its ability to produce acid and form biofilms. English and colleagues (2004) at the University of Waikato published research in the Journal of the International Academy of Periodontology showing that manuka honey with a UMF rating of 15+ significantly inhibited plaque bacteria and reduced gingivitis bleeding compared to a control group.
Gingivitis, the inflammation of the gum tissue caused by bacterial plaque accumulation along the gingival margin, is the precursor to more serious periodontal disease. Research has shown that manuka honey inhibits the growth of Porphyromonas gingivalis, one of the keystone pathogens in periodontal disease. Porphyromonas gingivalis produces proteolytic enzymes that destroy gum tissue and alveolar bone, leading to tooth loss if untreated. The ability of manuka honey to inhibit this organism while simultaneously reducing gingival inflammation suggests potential applications in periodontal therapy, either as a topical gel or as a component of oral rinse formulations.
Post-surgical oral healing is an area where manuka honey's combined antibacterial and wound healing properties offer particular advantage. Dental extractions, periodontal surgery, and oral mucosal procedures all create surgical wounds in the bacteria-rich oral environment, and post-operative infection is a significant concern. Research on honey-impregnated dressings and gels for extraction sockets has shown reduced rates of dry socket (alveolar osteitis), decreased post-operative pain and swelling, and accelerated mucosal healing. The honey's ability to control oral bacteria while promoting tissue regeneration in a moist healing environment makes it well-suited for these applications.
Biofilm Disruption Research
Biofilms are implicated in approximately 80 percent of all chronic infections and represent one of the greatest challenges in modern medicine. These structured communities of bacteria encase themselves in a self-produced extracellular polymeric substance (EPS) matrix composed of polysaccharides, proteins, lipids, and extracellular DNA. Within this protective matrix, bacteria are shielded from antibiotics, immune cells, and antiseptics. Biofilm-associated bacteria can tolerate antibiotic concentrations 100 to 1,000 times higher than planktonic bacteria, making biofilm infections extraordinarily difficult to treat. The ability of manuka honey to disrupt biofilms has emerged as one of its most clinically significant properties.
Chronic wound biofilms are present in an estimated 60 to 90 percent of non-healing chronic wounds, including diabetic foot ulcers, venous leg ulcers, and pressure ulcers. These biofilms prevent wound healing by sustaining chronic inflammation, inhibiting epithelial cell migration, and producing tissue-destructive enzymes. Research by Maddocks and colleagues (2012), published in Microbiology, demonstrated that manuka honey prevented S. pyogenes biofilm formation on wound-relevant substrates and disrupted established biofilms by inhibiting bacterial binding to the wound matrix proteins fibronectin and fibrinogen. Alandejani and colleagues (2009) published research in Otolaryngology-Head and Neck Surgery showing that manuka honey was effective against biofilms formed by S. aureus and P. aeruginosa on sinus mucosa, achieving greater biofilm killing than individual antibiotics.
Research by Roberts and colleagues (2015) published in PLOS ONE demonstrated that manuka honey disrupted P. aeruginosa biofilms through multiple mechanisms. The honey reduced the expression of genes involved in quorum sensing, the bacterial communication system that coordinates biofilm formation and virulence factor production. It also disrupted the structural integrity of the EPS matrix, exposing previously protected bacteria to both the honey's antibacterial compounds and the host immune response. These findings suggest that manuka honey could serve as a biofilm-disrupting agent that restores the efficacy of the immune system and conventional antibiotics against biofilm-associated infections.
Implant infections represent another critical application for manuka honey's anti-biofilm properties. Prosthetic joint infections, vascular graft infections, and catheter-related bloodstream infections are all driven by biofilm formation on the implant surface. These infections often require surgical removal of the implant because antibiotics cannot penetrate the biofilm. Research has explored coating medical implants and wound dressings with manuka honey to prevent initial bacterial adhesion and biofilm formation. Campeau and Patel (2014) demonstrated that manuka honey inhibited S. aureus biofilm formation on orthopedic implant materials. This preventive approach could potentially reduce the devastating morbidity and healthcare costs associated with implant infections.
Synergistic Effects
One of the most promising areas of manuka honey research involves its synergistic interactions with conventional antibiotics and other antimicrobial agents. Synergy occurs when two agents used together produce an antibacterial effect greater than the sum of their individual effects, allowing lower doses of each agent to achieve therapeutic efficacy. These synergistic combinations have particular relevance in the era of antibiotic resistance, where restoring the effectiveness of existing antibiotics is as important as developing new ones.
Synergy with conventional antibiotics has been demonstrated in multiple studies. Jenkins and Cooper (2012) published research in the International Journal of Antimicrobial Agents demonstrating that manuka honey restored the sensitivity of MRSA to oxacillin, an antibiotic to which MRSA is by definition resistant. When MRSA was exposed to sub-inhibitory concentrations of manuka honey in combination with oxacillin, the antibiotic regained its bactericidal activity. This remarkable finding suggests that manuka honey can reverse antibiotic resistance mechanisms, potentially restoring the clinical utility of antibiotics that have been rendered obsolete by resistance. Similar synergistic effects have been documented between manuka honey and rifampicin, tetracycline, imipenem, and mupirocin against various resistant organisms.
The mechanism underlying this synergy appears to involve manuka honey's disruption of bacterial cell membrane integrity and efflux pump function. Many antibiotic resistance mechanisms depend on active efflux pumps that expel antibiotics from the bacterial cell before they can reach their intracellular targets. By compromising membrane function and efflux pump activity, manuka honey allows antibiotics to accumulate inside the bacterial cell at concentrations sufficient to exert their bactericidal effects.
Synergy with other wound care agents has also been explored. Combinations of manuka honey with silver dressings, negative pressure wound therapy, and antimicrobial wound irrigants have been reported in clinical case studies with encouraging results. The complementary mechanisms of action, with honey targeting biofilms and modulating inflammation while silver provides broad-spectrum antimicrobial activity, create a more comprehensive approach to complex wound management. However, it should be noted that the acidic pH of manuka honey can affect the release kinetics of silver from silver-containing dressings, and careful consideration of product compatibility is necessary when combining different wound care modalities.
Other Health Benefits
Beyond its well-established antibacterial properties, manuka honey possesses several additional health-promoting activities that contribute to its overall therapeutic value. These ancillary benefits are supported by a growing body of preclinical and clinical research.
Anti-inflammatory activity is a significant component of manuka honey's therapeutic profile. Chronic inflammation is a driving factor in impaired wound healing, and the persistent inflammatory state seen in chronic wounds, autoimmune conditions, and metabolic diseases represents a major clinical challenge. Research has shown that manuka honey modulates the inflammatory response by reducing the production of pro-inflammatory cytokines, including tumor necrosis factor-alpha (TNF-alpha), interleukin-1 beta (IL-1 beta), and interleukin-6 (IL-6), while simultaneously promoting the production of anti-inflammatory mediators. Tomblin and colleagues (2014) published research in Cytokine demonstrating that manuka honey stimulated the release of TNF-alpha from macrophages through Toll-like receptor signaling, an effect that promotes appropriate initial inflammatory responses needed for wound debridement while preventing the transition to pathological chronic inflammation.
Antioxidant capacity is conferred by the phenolic compounds, flavonoids, and other phytochemicals present in manuka honey. These antioxidants scavenge reactive oxygen species (ROS) and free radicals that cause oxidative damage to cellular membranes, proteins, and DNA. Oxidative stress is implicated in aging, cardiovascular disease, neurodegenerative diseases, and cancer. The antioxidant capacity of manuka honey has been measured using ORAC (oxygen radical absorbance capacity) and DPPH (2,2-diphenyl-1-picrylhydrazyl) assays, consistently demonstrating higher antioxidant activity than many conventional honeys. The key antioxidant compounds in manuka honey include methyl syringate, pinobanksin, pinocembrin, chrysin, gallic acid, and caffeic acid.
Prebiotic effects on the gut microbiome represent an emerging area of research. Manuka honey contains oligosaccharides and other non-digestible carbohydrates that can selectively stimulate the growth and activity of beneficial gut bacteria, particularly Bifidobacterium and Lactobacillus species. Rosendale and colleagues (2008) published research demonstrating that manuka honey enhanced the growth of beneficial gut bacteria in a model colon system while its antibacterial activity simultaneously inhibited pathogenic organisms. This selective prebiotic effect suggests that manuka honey consumption could support a healthy gut microbiome composition, potentially benefiting digestive health, immune function, and overall well-being.
Skin care applications have expanded as the cosmetic and dermatological industries have recognized manuka honey's beneficial properties. The honey's humectant properties draw moisture into the skin and help maintain hydration. Its anti-inflammatory activity soothes conditions such as eczema, psoriasis, and acne. Its antibacterial properties make it effective against Cutibacterium acnes (formerly Propionibacterium acnes), the bacterium implicated in acne vulgaris. The promotion of collagen synthesis and tissue repair supports anti-aging effects. Manuka honey is now incorporated into numerous skin care products, including face masks, cleansers, moisturizers, and spot treatments, though the MGO concentrations in cosmetic products are generally much lower than those in medical-grade formulations.
How to Choose Quality Manuka Honey
The global market for manuka honey has experienced extraordinary growth, with premium grades commanding prices of $50 to $150 or more per jar. This commercial value has unfortunately attracted widespread fraud and adulteration, making informed purchasing decisions essential for consumers seeking genuine therapeutic-grade products.
UMF certification from the UMF Honey Association (UMFHA) is widely considered the most reliable indicator of genuine, quality-tested manuka honey. The UMFHA is an independent industry body that licenses producers to use the UMF trademark only after they meet stringent testing and traceability requirements. UMF-certified honey must be tested by accredited third-party laboratories for MGO concentration, leptosperin levels, DHA content, and HMF levels. It must be produced, packed, and labeled in New Zealand, ensuring full traceability from hive to shelf. The UMF license number and rating must appear on every jar. Consumers should verify the license number on the UMFHA website to confirm authenticity.
MGO levels provide a direct, quantitative measure of the primary antibacterial compound and should be checked alongside or instead of UMF ratings. For general wellness and immune support, MGO 83+ (UMF 5+) may be sufficient. For therapeutic applications including wound care, digestive health, and infection management, a minimum of MGO 263+ (UMF 10+) is recommended, with MGO 514+ (UMF 15+) or higher preferred for serious clinical applications. Look for MGO certification on the label from a recognized testing laboratory. The MGO rating should be stated as a guaranteed minimum, meaning the actual MGO content may be equal to or higher than the stated value.
Authenticity testing has become increasingly sophisticated in response to fraud concerns. The New Zealand Ministry for Primary Industries (MPI) implemented an official manuka honey definition in 2018 that requires testing for five chemical markers (leptosperin, DHA, MGO, hydroxymethylfurfural, and 3-phenyllactic acid) and one DNA marker (pollen DNA from Leptospermum scoparium) to be labeled as manuka honey for export. This regulatory framework is among the most rigorous food authentication standards in the world. Consumers should look for products that comply with MPI testing requirements, particularly for honey purchased outside New Zealand where labeling regulations may be less stringent.
Fraud concerns are well-documented in the manuka honey industry. It has been widely reported that the volume of honey sold globally as "manuka" far exceeds the total production capacity of New Zealand's manuka beekeeping industry. Fraudulent practices include diluting genuine manuka honey with cheaper conventional honey, artificially boosting MGO levels through the addition of synthetic methylglyoxal or DHA, mislabeling non-manuka honeys as manuka, and using misleading terminology such as "manuka blend" or "with manuka honey" on products containing minimal amounts of genuine manuka honey. Purchasing from reputable brands with verifiable UMF or MGO certification, checking for New Zealand origin, and buying from authorized retailers are the best protections against fraud.
Forms and Applications
Manuka honey is available in several forms, each designed for specific therapeutic applications. The appropriate form depends on the intended use, the condition being treated, and whether clinical-grade standardization is required.
Raw manuka honey is the most common consumer form, available in glass or plastic jars ranging from 250 grams to 1 kilogram. High-quality raw manuka honey has a distinctive thick, creamy texture, a rich amber to dark brown color, and a complex flavor profile that is less sweet than conventional honey, with herbaceous, slightly bitter, and earthy undertones. Raw manuka honey can be consumed directly, dissolved in warm (not hot) beverages, spread on food, or applied topically to minor skin wounds and irritations. It should not be heated above 40 degrees Celsius, as excessive heat can degrade MGO and other bioactive compounds. Raw manuka honey retains all of its natural enzymes, phenolic compounds, and flavonoids, making it suitable for both internal consumption and external application for non-critical wounds.
Medical-grade Medihoney products represent the clinical standard for wound care applications. These products are manufactured under strict quality control conditions and are gamma-irradiated for sterility, a process that eliminates bacterial spores (including Clostridium botulinum) without affecting the honey's antibacterial activity. Medihoney products are FDA-cleared, CE-marked, and registered with regulatory authorities in multiple countries. They are available in several formulations: antibacterial wound gel for direct application to wound beds, calcium alginate dressings for moderate to heavily exuding wounds, adhesive dressings for superficial wounds and catheter sites, and paste for cavity wounds. Medical-grade products should be used for all significant wounds, particularly those at risk of infection, and they are the only appropriate choice for use in clinical healthcare settings.
Wound dressings impregnated with manuka honey are designed for easy clinical application and represent the most practical format for wound management. These dressings combine the antibacterial and healing properties of manuka honey with the absorptive and protective functions of modern wound dressing materials. Alginate-honey dressings are used for moderate to heavily exuding wounds, where the alginate fibers absorb excess exudate while the honey provides antimicrobial activity. Tulle dressings coated with manuka honey are used for superficial wounds, burns, and skin graft donor sites. Hydrogel-honey dressings provide moisture to dry wound beds while delivering antibacterial honey. These products are designed for daily or alternate-day dressing changes and are available in various sizes to accommodate different wound dimensions.
Lozenges containing manuka honey are designed for oral and throat applications. These products deliver manuka honey directly to the pharyngeal and oral mucosa, providing antibacterial and soothing effects for sore throat, oral mucositis, and general oral health. Quality lozenges should contain a specified MGO level and be free from artificial additives. Some formulations combine manuka honey with propolis, another bee product with antibacterial properties, for enhanced throat care.
Capsules containing freeze-dried or encapsulated manuka honey are available for convenient internal consumption. These products aim to deliver the antibacterial and prebiotic benefits of manuka honey to the gastrointestinal tract in a measured dose format. However, capsule formulations may not retain all the bioactive properties of raw honey, and their clinical efficacy compared to raw honey consumption has not been extensively studied.
Recommended Usage
The appropriate use of manuka honey depends on the intended application, the severity of the condition being treated, and whether the honey is being used for general wellness or specific therapeutic purposes. The following guidelines are based on published research and clinical practice recommendations.
Wound application requires proper technique to maximize therapeutic benefit. For non-critical wounds that can be managed at home, clean the wound with sterile saline or clean water and pat dry. Apply a layer of UMF 15+ (MGO 514+) or higher manuka honey directly to the wound bed, ensuring complete coverage. Cover with a clean, non-adherent dressing and secure with tape or a bandage. Change the dressing daily or when strike-through of wound exudate is visible. For deeper or more complex wounds, apply the honey to the dressing rather than directly to the wound, then place the honey-loaded dressing onto the wound surface. This technique ensures even distribution and reduces discomfort during application. Any wound showing signs of clinical infection (increasing redness, swelling, warmth, purulent drainage, fever) requires professional medical evaluation regardless of honey use.
Internal use for general wellness and digestive health typically involves consuming one to two tablespoons (approximately 15 to 30 milliliters) of raw manuka honey per day. For digestive complaints and potential H. pylori management, take one tablespoon on an empty stomach 30 minutes before meals, three times daily. For sore throat relief, allow a teaspoon of manuka honey to dissolve slowly in the mouth, coating the pharyngeal tissues. For oral health, allow a small amount of honey to dissolve over the teeth and gums after brushing. The honey can be consumed directly from the spoon, dissolved in warm water or herbal tea (below 40 degrees Celsius to preserve bioactive compounds), or added to smoothies and other foods.
Dosage guidelines vary by application. For topical wound use, apply sufficient honey to cover the wound bed to a depth of approximately 3 millimeters, with quantities adjusted based on wound size and exudate levels. Heavily exuding wounds require more honey and more frequent dressing changes, as exudate dilutes the honey and reduces its concentration. For internal use, most studies have used doses of 20 to 40 grams per day (approximately 1 to 2 tablespoons). Higher doses have not been shown to provide additional benefit and add unnecessary sugar intake. Manuka honey should be viewed as a complementary therapeutic agent rather than a replacement for prescribed medications or professional medical care.
Safety and Contraindications
Manuka honey is generally recognized as safe for most adults when used topically or consumed orally in reasonable quantities. However, several important contraindications and precautions must be observed to prevent adverse outcomes.
Bee allergy is an absolute contraindication for manuka honey use. Individuals with known allergies to bee venom, bee products, or pollen should not use manuka honey in any form, whether topical or oral. Honey can contain trace amounts of bee proteins, pollen particles, and propolis residues that may trigger allergic reactions ranging from mild contact dermatitis or oral tingling to severe anaphylaxis in sensitized individuals. Patients with a history of atopic conditions (eczema, asthma, allergic rhinitis) should exercise caution and may wish to perform a small skin patch test before first use. Apply a small amount of honey to the inner forearm, cover with a bandage, and observe for 24 hours for signs of allergic reaction before proceeding with therapeutic use.
Diabetes and blood sugar management require careful consideration when using manuka honey. Like all honeys, manuka honey is a concentrated source of sugars, containing approximately 80 percent carbohydrates by weight, predominantly fructose and glucose. Oral consumption of manuka honey will raise blood glucose levels and must be accounted for in diabetic meal planning and insulin dosing. While some research suggests that honey may have a lower glycemic impact than refined sugars, it remains a significant source of rapidly absorbed carbohydrate. Diabetic patients using manuka honey should monitor blood glucose levels closely and consult with their diabetes care team. Topical application of manuka honey to wounds in diabetic patients does not significantly affect blood glucose levels and is considered safe when performed under clinical supervision.
Infants under one year of age must never be given honey of any kind, including manuka honey, due to the risk of infant botulism. Honey can contain dormant spores of Clostridium botulinum that, while harmless to older children and adults with mature gut microbiomes, can germinate in the immature intestinal tract of infants and produce botulinum toxin, a potentially fatal neurotoxin. This risk applies to all honeys regardless of quality, grade, or processing. Medical-grade gamma-irradiated manuka honey products are sterilized to eliminate botulinum spores and may be used topically on infant wounds under medical supervision, but oral consumption of any honey product remains strictly contraindicated for children under 12 months of age.
Wound depth and severity considerations are essential for safe topical use. While manuka honey is appropriate for superficial wounds, partial-thickness burns, and many chronic wound types, it should not be used as a sole treatment for deep wounds with exposed tendon, bone, or joint capsule, or for wounds with uncontrolled bleeding or suspected necrotizing fasciitis. These conditions require urgent surgical intervention and systemic antibiotic therapy. Manuka honey can be incorporated into the post-surgical wound care plan for such conditions but should never delay or replace necessary medical or surgical treatment. Any wound that deteriorates despite honey treatment, shows signs of spreading infection, or is associated with systemic symptoms of sepsis requires immediate professional medical evaluation.
Other precautions include the potential for a transient stinging sensation when honey is first applied to open wounds, which typically subsides within 15 to 30 minutes. This sensation is attributed to the acidic pH of the honey and is not indicative of an allergic reaction or tissue damage. Rare cases of contact dermatitis to honey have been reported and should prompt discontinuation. Interactions with medications are generally not a concern, though the anti-platelet effects of some honey compounds theoretically warrant caution in patients on anticoagulant therapy or preparing for surgery.
Key Research Papers and References
The following publications represent foundational and significant contributions to the scientific understanding of manuka honey's antibacterial properties and clinical applications.
- Molan PC, Russell KM. "Non-peroxide antibacterial activity in some New Zealand honeys." Journal of Apicultural Research. 1988;27(1):62-67.
- Molan PC. "The antibacterial activity of honey. 1. The nature of the antibacterial activity." Bee World. 1992;73(1):5-28.
- Al Somal N, Coley KE, Molan PC, Hancock BM. "Susceptibility of Helicobacter pylori to the antibacterial activity of manuka honey." Journal of the Royal Society of Medicine. 1994;87(1):9-12.
- Molan PC. "The role of honey in the management of wounds." Journal of Wound Care. 2001;10(1):5-12.
- Cooper RA, Molan PC, Harding KG. "The sensitivity to honey of Gram-positive cocci of clinical significance isolated from wounds." Journal of Applied Microbiology. 2002;93(5):857-863.
- English HK, Pack AR, Molan PC. "The effects of manuka honey on plaque and gingivitis: a pilot study." Journal of the International Academy of Periodontology. 2004;6(2):63-67.
- Blaser G, Santos K, Bode U, Vetter H, Simon A. "Effect of medical honey on wounds colonised or infected with MRSA." Journal of Wound Care. 2007;16(8):325-328.
- Mavric E, Wittmann S, Barth G, Henle T. "Identification and quantification of methylglyoxal as the dominant antibacterial constituent of manuka (Leptospermum scoparium) honeys from New Zealand." Molecular Nutrition and Food Research. 2008;52(4):483-489.
- Jull AB, Walker N, Deshpande S. "Honey as a topical treatment for wounds." Cochrane Database of Systematic Reviews. 2008;(4):CD005083.
- Wijesinghe M, Weatherall M, Perrin K, Beasley R. "Honey in the treatment of burns: a systematic review and meta-analysis of its efficacy." New Zealand Medical Journal. 2009;122(1295):47-60.
- Blair SE, Cokcetin NN, Harry EJ, Carter DA. "The unusual antibacterial activity of medical-grade Leptospermum honey: antibacterial spectrum, resistance and transcriptome analysis." European Journal of Clinical Microbiology and Infectious Diseases. 2009;28(10):1199-1208.
- Alandejani T, Marsan J, Ferris W, Slinger R, Chan F. "Effectiveness of honey on Staphylococcus aureus and Pseudomonas aeruginosa biofilms." Otolaryngology-Head and Neck Surgery. 2009;141(1):114-118.
- Kwakman PH, te Velde AA, de Boer L, Speijer D, Vandenbroucke-Grauls CM, Zaat SA. "How honey kills bacteria." FASEB Journal. 2010;24(7):2576-2582.
- Jervis-Bardy J, Foreman A, Bray S, Tan L, Wormald PJ. "Methylglyoxal-infused honey mimics the anti-Staphylococcus aureus biofilm activity of manuka honey." Laryngoscope. 2011;121(6):1104-1107.
- Jenkins R, Cooper RA. "Improving antibiotic activity against wound pathogens with manuka honey in vitro." PLOS ONE. 2012;7(9):e45600.
- Maddocks SE, Lopez MS, Sherlock O, et al. "Manuka honey inhibits the development of Streptococcus pyogenes biofilms and causes reduced expression of two fibronectin binding proteins." Microbiology. 2012;158(Pt 3):781-790.
- Lu J, Turnbull L, Burke CM, et al. "Manuka-type honeys can eradicate biofilms produced by Staphylococcus aureus strains with different biofilm-forming abilities." PeerJ. 2014;2:e326.
- Carter DA, Blair SE, Cokcetin NN, et al. "Therapeutic manuka honey: no longer so alternative." Frontiers in Microbiology. 2016;7:569.
- Johnston M, McBride M, Dahiya D, Owusu-Apenten R, Nigam PS. "Antibacterial activity of manuka honey and its components: an overview." AIMS Microbiology. 2018;4(4):655-664.
Research Papers
The following PubMed topic searches aggregate the peer-reviewed literature underpinning the claims above. Each link opens a live PubMed query so the result set stays current as new research is published.
- PubMed — methylglyoxal antibacterial activity
- PubMed — wound healing randomized trial
- PubMed — MRSA Staphylococcus aureus
- PubMed — biofilm antimicrobial
- PubMed — diabetic ulcer
- PubMed — burn treatment
- PubMed — sore throat and cough
- PubMed — Helicobacter pylori
- PubMed — oral and periodontal health
- PubMed — UMF and MGO standards
- PubMed — systematic review and meta-analysis
Connections
- Manuka Honey Benefits Deep Dive
- Staphylococcus Aureus
- Garlic
- Thyme
- Oregano
- Silver Nanoparticles
- Myrrh
- Honey
- Tea Tree
- Cancer
- Sepsis
- Urinary Tract Infections
- Eczema
- Acne
- Diabetes
- Pseudomonas Aeruginosa
- Collagen
- Cellulitis
- Cold Flu Treatments