Peppermint for IBS & Digestive Health
Enteric-coated peppermint oil for irritable bowel syndrome has produced some of the strongest randomized-trial evidence of any botanical preparation in any indication. The Khanna 2014 systematic review (9 trials, 726 patients) and the Alammar 2019 meta-analysis (12 trials, 835 patients) both reported a number needed to treat of approximately 3 for clinically meaningful improvement in global IBS symptoms — a treatment effect that exceeds many pharmaceutical IBS therapies. The American College of Gastroenterology, the British Society of Gastroenterology, and the European Society of Neurogastroenterology and Motility all endorse peppermint oil as a recommended first-line option for global IBS symptoms. The mechanism is precise and well-mapped: L-menthol blocks voltage-gated L-type calcium channels in intestinal smooth muscle, producing antispasmodic relaxation that reduces the visceral hypersensitivity and motility disturbances at the core of IBS pathophysiology. This page walks through the mechanism, the pivotal trials, the formulation differences (regular enteric coating vs IBgard sustained-release microspheres), dosing protocols, the functional dyspepsia and SIBO crossover applications, and the critical GERD caution.
Table of Contents
- Why Peppermint Oil's IBS Evidence Is So Strong
- Mechanism: L-Menthol Calcium Channel Blockade
- Pittler & Ernst 1998 — The First Meta-Analysis
- Khanna 2014 — Modern Systematic Review
- Alammar 2019 — Pooled Meta-Analysis
- IBgard Sustained-Release Microspheres
- Dosing Protocol and Practical Use
- Functional Dyspepsia and Iberogast
- SIBO and Herbal Antimicrobial Regimens
- Pre-Endoscopy Antispasmodic Use
- GERD — The Critical Caution
- Key Research Papers
- Connections
- Featured Videos
Why Peppermint Oil's IBS Evidence Is So Strong
It is genuinely unusual for a botanical preparation to accumulate the strength of evidence that enteric-coated peppermint oil has accumulated for irritable bowel syndrome. Most herbal interventions have, at best, a handful of small single-center trials with mixed results and minimal blinding. Peppermint oil for IBS has, by contrast:
- More than a dozen well-conducted double-blind, placebo-controlled randomized trials spanning four decades and multiple continents
- Multiple independent meta-analyses (Pittler 1998, Ford 2008, Khanna 2014, Alammar 2019) consistently reporting clinically meaningful effect sizes
- A number needed to treat of approximately 3 for symptom improvement — comparable to or better than tricyclic antidepressants, selective serotonin reuptake inhibitors, and antispasmodics
- Endorsement from three major gastroenterology professional societies (ACG, BSG, ESNM) as a recommended first-line therapy
- A coherent and well-documented mechanism (L-type calcium channel blockade in intestinal smooth muscle) that maps directly onto the symptoms it improves (pain, cramping, bloating)
- An excellent safety profile when delivered via enteric coating — the dominant adverse effect is a small increase in heartburn risk, which is a known and predictable consequence of the LES-relaxant effect
For comparison, the herbal interventions with similar evidence depth in other indications — St. John's Wort for mild-to-moderate depression, saw palmetto for benign prostatic hyperplasia, and Ginkgo biloba for vascular cognitive symptoms — all have produced more recent large-trial findings that complicated or contradicted the earlier positive findings. Peppermint oil's IBS evidence base has actually strengthened over time as more trials have been completed.
Mechanism: L-Menthol Calcium Channel Blockade
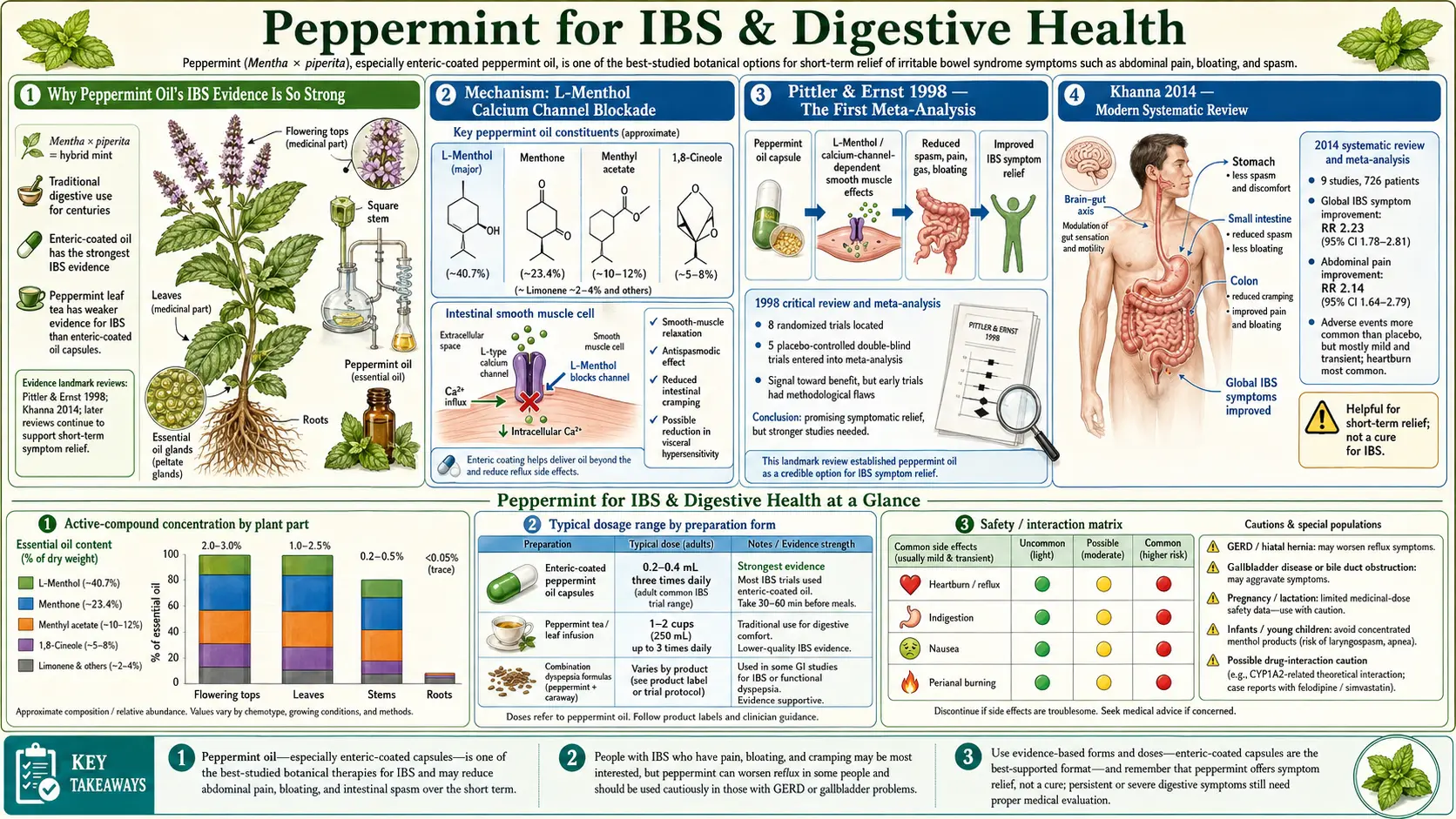
The mechanism of peppermint oil in IBS is essentially the same as the mechanism of the pharmaceutical antispasmodic drug class (mebeverine, hyoscine, otilonium, pinaverium, dicyclomine), but produced by a natural product rather than a synthesized drug. L-menthol — the dominant constituent of peppermint essential oil at 35-55% by weight — blocks voltage-gated L-type calcium channels in intestinal smooth muscle. The result is reduced calcium influx during depolarization, reduced calcium-calmodulin activation of myosin light chain kinase, and reduced smooth muscle contraction.
This is the same fundamental mechanism as the dihydropyridine calcium-channel-blocker drug class (nifedipine, amlodipine, felodipine) used systemically for hypertension. The clinical difference is delivery: peppermint oil delivered via enteric-coated capsule releases its menthol in the small intestine and colon, where the absorption is local and the systemic concentrations remain low. The effect is therefore concentrated where it is wanted (gut smooth muscle) rather than affecting cardiac and vascular smooth muscle as systemic calcium channel blockers do.
Three additional mechanisms contribute:
- 5-HT3 receptor antagonism — menthol partially blocks 5-HT3 serotonin receptors on enteric sensory neurons, the same receptor target as the IBS-D drug alosetron. This reduces visceral hypersensitivity (the abnormal pain response to normal gut distension that is a hallmark of IBS).
- TRPM8 cold-receptor activation — menthol activates TRPM8 receptors on enteric afferents, which can produce a counter-irritant effect that crowds out competing visceral pain signaling.
- Anti-inflammatory effects — peppermint oil reduces production of pro-inflammatory cytokines (TNF-alpha, IL-1beta) in intestinal tissue, addressing the low-grade mucosal inflammation that contributes to a subset of IBS cases.
The composite effect is reduced cramping pain, reduced bloating from improved transit, reduced urgency, and reduced visceral hypersensitivity — addressing the four symptom domains that dominate the IBS clinical picture.
Pittler & Ernst 1998 — The First Meta-Analysis
The first systematic review and meta-analysis of peppermint oil for IBS was published in 1998 by Max Pittler and Edzard Ernst at the University of Exeter Complementary Medicine unit. The authors pooled five double-blind, placebo-controlled randomized trials (197 total patients) of enteric-coated peppermint oil capsules and reported a statistically significant benefit on global IBS symptoms with an odds ratio of approximately 2.7 favoring peppermint over placebo.
The Pittler-Ernst paper was important not because the effect size was unusually large — it was modest by absolute standards — but because it established that peppermint oil deserved serious consideration as a real intervention rather than dismissal as folk medicine. The authors specifically noted that the trials with enteric-coated formulations performed better than the trials with uncoated peppermint oil, establishing the principle (later confirmed) that the enteric coating is essential for both efficacy and tolerability.
The paper's caveat was that the included trials were small and somewhat methodologically heterogeneous, and the authors called for larger and more rigorous trials. Those trials were subsequently completed over the following 15 years, and the later meta-analyses (Khanna 2014, Alammar 2019) confirmed and strengthened the original finding.
Khanna 2014 — Modern Systematic Review
Reshma Khanna and colleagues at the University of Western Ontario published an updated systematic review and meta-analysis in 2014, pooling nine randomized placebo-controlled trials with a total of 726 IBS patients. The headline findings:
- Global IBS symptom improvement: relative risk of improvement 2.23 (95% CI 1.78-2.81) favoring peppermint over placebo
- Abdominal pain reduction: relative risk 2.14 (95% CI 1.64-2.79) favoring peppermint
- Number needed to treat for symptom improvement: approximately 3
- Number needed to harm for adverse events: approximately 114 (heartburn was the most common adverse effect)
- Adverse events were transient and mild in all trials — no serious treatment-related adverse events were reported across the pooled cohort
The Khanna 2014 paper is the most-cited reference for peppermint oil's efficacy in IBS and is the basis for the American College of Gastroenterology's endorsement of peppermint oil as a recommended therapy for global IBS symptoms in their 2021 clinical guideline.
For context, the number needed to treat of approximately 3 compares favorably with most pharmaceutical IBS therapies. Tricyclic antidepressants for IBS have an NNT of approximately 4. Selective serotonin reuptake inhibitors have an NNT of approximately 4. The IBS-C drug linaclotide has an NNT of approximately 7. The IBS-D drug rifaximin has an NNT of approximately 9. Peppermint oil's effect size is therefore in the upper tier of available IBS interventions on average, and substantially exceeds placebo response by clinically meaningful margins.
Alammar 2019 — Pooled Meta-Analysis
The 2019 meta-analysis by Nour Alammar and colleagues at the University of Maryland School of Medicine pooled 12 randomized placebo-controlled trials with 835 total IBS patients — the largest meta-analysis to date. Key findings:
- Improvement in global IBS symptoms: relative risk 2.39 (95% CI 1.93-2.97) favoring peppermint
- Reduction in abdominal pain: relative risk 1.78 (95% CI 1.43-2.20) favoring peppermint
- Both effects were statistically significant with low heterogeneity (I² less than 30%), meaning the trials produced consistent results despite methodological variation
- Subgroup analyses found benefit across IBS subtypes (IBS-D, IBS-C, IBS-M)
- Trials of longer duration (8-12 weeks) and trials using IBgard sustained-release microspheres showed numerically larger effect sizes than shorter trials with regular enteric coating
The Alammar paper is the strongest single piece of evidence supporting clinical use of peppermint oil in IBS. The combination of effect size, consistency across trials, breadth of IBS subtypes benefiting, and acceptable safety profile justifies the major gastroenterology guideline endorsements.
For more on the IBS condition and the full menu of evidence-based treatment options, see our Irritable Bowel Syndrome page.
IBgard Sustained-Release Microspheres
The proprietary IBgard formulation (manufactured by IM HealthScience) uses a sustained-release microsphere technology that distributes the peppermint oil throughout the small intestine more uniformly than traditional enteric-coated capsules. Each IBgard capsule contains 180 mg of peppermint oil distributed across approximately 200 individual microspheres, each independently enteric-coated.
The clinical rationale is that traditional enteric-coated capsules release their full payload at a single point when the enteric coating dissolves at small-bowel pH, producing a high local concentration at one location and limited exposure elsewhere along the gut. The microsphere approach spreads the dose across the full length of the small intestine and into the proximal colon, producing more uniform smooth-muscle exposure.
The IBSREST randomized controlled trial (Cash et al. 2016) of IBgard in 72 IBS patients reported a 40% reduction in the IBS Symptom Severity Score over 4 weeks, compared to a 24% reduction with placebo, with effects detectable as early as 24 hours after starting therapy. The trial used the IBgard product specifically rather than generic enteric-coated peppermint oil.
For practical use, the choice between IBgard and a generic enteric-coated peppermint oil capsule (such as Heather's Tummy Care or Now Foods Peppermint Gels) is mostly a cost-vs-evidence-quality question. IBgard is more expensive but has the strongest single-product trial data. Generic enteric-coated peppermint oil capsules are substantially cheaper and have the bulk of the meta-analyzed evidence base behind them, though no single generic product has been specifically tested.
Dosing Protocol and Practical Use
Standard dosing protocols across the trial literature:
- Generic enteric-coated peppermint oil: 0.2 mL (approximately 180 mg) per capsule, taken 1 capsule three times daily, 30-60 minutes before meals
- IBgard sustained-release: 1-2 capsules three times daily before meals
- Trial duration: Typical trials run 4-12 weeks. The clinical benefit is generally apparent within 1-2 weeks if it is going to occur. Continuing therapy beyond 12 weeks is reasonable in responders.
- Timing relative to meals: Pre-meal dosing (30-60 minutes before) is the standard. Some practitioners suggest morning dosing for IBS-C and evening dosing for IBS-D, but the trial evidence supports the three-times-daily before-meals approach
- Reassessment point: Re-evaluate symptoms at 8-12 weeks. If there has been no meaningful improvement by 8 weeks, peppermint is unlikely to provide benefit and a different approach is warranted.
The capsules should be swallowed whole — not chewed, crushed, or opened — because the enteric coating is what prevents upper-GI release that would produce heartburn and burping of peppermint flavor. Patients who chew the capsules or who use uncoated peppermint oil preparations typically experience uncomfortable upper-GI symptoms within minutes and discontinue.
Functional Dyspepsia and Iberogast
Functional dyspepsia — chronic upper-GI discomfort, bloating, postprandial fullness, and early satiety without identifiable structural disease — shares many mechanistic features with IBS, and peppermint has been studied as a treatment with positive results.
The most-studied combination product is Iberogast (STW 5), a German herbal preparation containing nine botanicals including peppermint, caraway, chamomile, licorice root, milk thistle, lemon balm, angelica root, celandine, and bitter candytuft. Iberogast has more than two decades of clinical trial evidence in functional dyspepsia, with multiple RCTs showing meaningful symptom reduction. The product is widely used in Germany and is available in the US as a dietary supplement.
For peppermint specifically (separate from the broader Iberogast preparation), the most-cited combination is peppermint oil + caraway oil. Multiple trials of this combination in functional dyspepsia have shown improvement in dyspeptic symptoms (epigastric pain, fullness, bloating) compared to placebo, with effect sizes in the moderate range. The combination is available as Carmenthin in Germany and is approximately equivalent to standard pharmaceutical dyspepsia therapy in head-to-head trials.
The mechanism overlaps with IBS: peppermint relaxes gastric smooth muscle and reduces postprandial spasm, while caraway adds carminative effects (reduces gas formation and bloating) and additional antispasmodic action.
For a comprehensive review of fennel, another carminative herb often used in similar functional GI applications, see our Fennel page.
SIBO and Herbal Antimicrobial Regimens
Small intestinal bacterial overgrowth (SIBO) treatment protocols commonly include peppermint oil as one component of broader herbal antimicrobial regimens. Peppermint oil has documented antimicrobial activity against many of the bacterial species implicated in SIBO — E. coli, Klebsiella, Enterococcus, methanogenic archaea — in laboratory studies.
The Chedid et al. 2014 SIBO trial at Johns Hopkins compared an herbal antimicrobial regimen (containing oregano oil and berberine, with a related arm including peppermint oil) to the pharmaceutical antibiotic rifaximin in 104 SIBO patients. The herbal regimen produced similar SIBO eradication rates (46% vs 34% for rifaximin) at similar cost, supporting the legitimacy of botanical approaches in this indication.
In standard integrative SIBO protocols, peppermint oil is typically used alongside oregano oil, berberine, allicin (garlic-derived), and neem — a combination intended to address the broader spectrum of SIBO bacteria including the methane-producing archaea that often resist single-agent therapy. The dual benefit of peppermint in this context is the antimicrobial action plus the antispasmodic relief of the cramping and bloating symptoms that SIBO produces.
For detailed SIBO management including the herbal-antimicrobial protocols, see our SIBO page and the deep-dive sub-article on herbal antimicrobials.
Pre-Endoscopy Antispasmodic Use
A less-publicized application of peppermint oil is as a pre-procedure antispasmodic during colonoscopy and upper endoscopy. Topical peppermint oil sprayed onto the colonic mucosa during colonoscopy reduces colonic spasm, improves visualization, and reduces procedural discomfort — effects documented in multiple RCTs from Japan, Italy, and the UK.
The Mizuno 2006 trial in Japan and the Asao 2003 trial both demonstrated that peppermint oil spray during colonoscopy reduced colonic muscle contractions and improved polyp detection compared to placebo or saline spray. The Inoue 2014 trial extended these findings to esophagogastroduodenoscopy (EGD), with peppermint oil reducing gastric muscle activity and improving visualization of the gastric mucosa.
While not a take-home prescription, this validates the antispasmodic mechanism in a setting (real-time endoscopic observation) where the effect can be directly visualized rather than inferred from symptom reports. Peppermint oil's smooth-muscle-relaxing effect is genuine, reproducible, and reliable.
GERD — The Critical Caution
The most important practical caution for peppermint oil in IBS is its effect on the lower esophageal sphincter (LES). The same smooth-muscle calcium-channel blockade that produces antispasmodic relief in the gut also reduces resting LES tone — the muscular ring that prevents stomach acid from refluxing into the esophagus. In patients with gastroesophageal reflux disease, hiatal hernia, or symptomatic acid reflux, peppermint can worsen symptoms substantially.
This is the most common scenario in which peppermint goes from helpful to harmful. Many IBS patients also have overlapping GERD — both involve visceral hypersensitivity and autonomic dysregulation, and the conditions co-occur much more often than chance. A patient who starts peppermint oil capsules for IBS symptoms and develops worsening heartburn within 1-2 weeks is experiencing a predictable mechanism-based adverse effect, not an idiosyncratic reaction.
Practical guidance:
- Avoid peppermint in known GERD, hiatal hernia, or active reflux symptoms. The benefit-risk balance does not favor it in this population, even for severe IBS.
- Enteric coating reduces but does not eliminate the LES effect. Absorbed menthol still circulates systemically.
- If heartburn appears after starting peppermint, discontinue. The effect typically appears within the first 1-2 weeks. Continuing risks esophagitis over time.
- Substitute non-LES-relaxant antispasmodics in GERD-IBS overlap. Ginger, fennel, soluble fiber (psyllium husk), low-FODMAP dietary management, and pharmaceutical antispasmodics that do not cross the BBB or affect smooth muscle outside the gut wall are reasonable alternatives.
The other significant cautions are: gallstones (peppermint increases bile flow and can precipitate biliary colic), infants and very young children under 2-5 years (menthol exposure is associated with rare cases of laryngospasm), and pregnancy (moderate dietary peppermint is fine; high-dose essential oil supplementation should be avoided).
Key Research Papers
- Pittler MH, Ernst E (1998). Peppermint oil for irritable bowel syndrome: a critical review and meta-analysis. American Journal of Gastroenterology. — PubMed
- Ford AC et al. (2008). Effect of fibre, antispasmodics, and peppermint oil in the treatment of irritable bowel syndrome: systematic review and meta-analysis. BMJ. — PubMed
- Khanna R, MacDonald JK, Levesque BG (2014). Peppermint oil for the treatment of irritable bowel syndrome: a systematic review and meta-analysis. Journal of Clinical Gastroenterology. — PubMed
- Cash BD et al. (2016). A novel delivery system of peppermint oil is an effective therapy for irritable bowel syndrome symptoms (IBSREST trial). Digestive Diseases and Sciences. — PubMed
- Alammar N et al. (2019). The impact of peppermint oil on the irritable bowel syndrome: a meta-analysis of the pooled clinical data. BMC Complementary and Alternative Medicine. — PubMed
- Hawthorn M et al. (1988). The actions of peppermint oil and menthol on calcium channel-dependent processes in intestinal, neuronal and cardiac preparations. Alimentary Pharmacology & Therapeutics. — PubMed
- Chedid V et al. (2014). Herbal therapy is equivalent to rifaximin for the treatment of small intestinal bacterial overgrowth. Global Advances in Health and Medicine. — PubMed
- Lacy BE et al. (2021). ACG Clinical Guideline: Management of Irritable Bowel Syndrome. American Journal of Gastroenterology. — PubMed
- Madisch A et al. (2004). Treatment of functional dyspepsia with a herbal preparation (STW 5, Iberogast). Alimentary Pharmacology & Therapeutics. — PubMed
- Holtmann G et al. (2003). Efficacy of artichoke leaf extract in the treatment of patients with functional dyspepsia. Alimentary Pharmacology & Therapeutics (with peppermint-caraway combination comparison). — PubMed
- Inoue K et al. (2014). L-menthol improves adenoma detection rate during colonoscopy. Endoscopy. — PubMed
- Asao T et al. (2003). Peppermint oil spray as an aid to colonoscopy. Gastrointestinal Endoscopy. — PubMed
PubMed Topic Searches
- PubMed: Peppermint IBS meta-analyses
- PubMed: Menthol calcium channel mechanism
- PubMed: IBgard formulation trials
- PubMed: Peppermint dyspepsia caraway
- PubMed: Peppermint endoscopy antispasmodic
- PubMed: Peppermint SIBO herbal
Connections
- Peppermint Overview
- Peppermint Benefits Hub
- Peppermint for Headache
- Peppermint for Respiratory
- Peppermint for Cognitive
- Irritable Bowel Syndrome
- SIBO
- Herbal Antimicrobials (SIBO)
- Low-FODMAP Diet
- Bloating
- Abdominal Pain
- Reflux and Heartburn
- Ginger
- Fennel
- Chamomile
- Gut Healing
- All Herbs