Peppermint — Benefits Deep Dive
Peppermint (Mentha × piperita) is a sterile natural hybrid of watermint (Mentha aquatica) and spearmint (Mentha spicata) that originated in late 17th-century England. The plant's pharmacology is dominated by a single molecule — L-menthol — that activates the TRPM8 cold-sensing receptor on sensory neurons (the source of the characteristic "cooling" sensation) while simultaneously blocking voltage-gated calcium channels in smooth muscle. The result is a remarkably broad clinical footprint for a single herb: enteric-coated peppermint oil has produced some of the strongest randomized-trial evidence of any botanical preparation in any indication (irritable bowel syndrome), topical peppermint oil has been validated in head-to-head trials against acetaminophen for tension headache, menthol vapor is the active component of every drugstore decongestant rub, and peppermint aroma reliably increases alertness on cognitive performance tasks. Four deep-dive pages below explore each application in detail.
Deep-Dive Articles
IBS & Digestive
The strongest evidence base for any peppermint preparation. Khanna 2014 and Alammar 2019 meta-analyses of enteric-coated peppermint oil (180-225 mg three times daily) for irritable bowel syndrome — number needed to treat of approximately 3 for clinically meaningful symptom improvement, among the strongest herbal RCT results in any indication. Pittler 1998 trial, L-menthol's voltage-gated calcium channel blockade in intestinal smooth muscle, the IBgard sustained-release microsphere formulation, functional dyspepsia (with caraway), and the GERD caution (peppermint relaxes the lower esophageal sphincter and worsens reflux).
Headache Relief
Göbel 1996 controlled trial of 10% peppermint oil in ethanol applied to the temples for tension-type headache — produced reduction in pain comparable to 1,000 mg acetaminophen by 15 minutes post-application. TRPM8 cold-receptor activation as a counter-irritant mechanism, nasal-inhalation use for migraine attacks, dilution requirements to prevent skin irritation, and the comparison to other topical agents (tiger balm, methyl salicylate).
Respiratory & Cough
Menthol's TRPM8 cold-receptor decongestant effect — the dissociation between subjective relief and objective airflow that Ahmed 2007 documented (patients report clearer breathing despite no change in spirometry). The Vicks VapoRub / menthol-rub mechanism, traditional steam inhalation, antitussive activity for cough reflex suppression, and the critical caution against menthol use in infants and very young children (laryngospasm risk).
Cognitive & Alertness
The Moss 2008 peppermint-aroma cognitive trial — the "minty smell makes you more alert" research that produced measurable improvements in working memory, sustained attention, and processing speed. The crucial mechanistic distinction between trigeminal arousal (menthol's irritant activation of the trigeminal nerve in the nasal cavity) and pure olfactory processing — peppermint works mostly through the trigeminal route, not classical smell. Implications for driving alertness, exam preparation, and afternoon-slump management.
Table of Contents
- Deep-Dive Articles
- Why Peppermint Produces Effects Across So Many Systems
- Research Papers: IBS & Digestive
- Research Papers: Headache
- Research Papers: Respiratory & Cough
- Research Papers: Cognitive & Alertness
- Caution: GERD and Lower Esophageal Sphincter
- External Authoritative Resources
- Connections
- Featured Videos
Why Peppermint Produces Effects Across So Many Systems
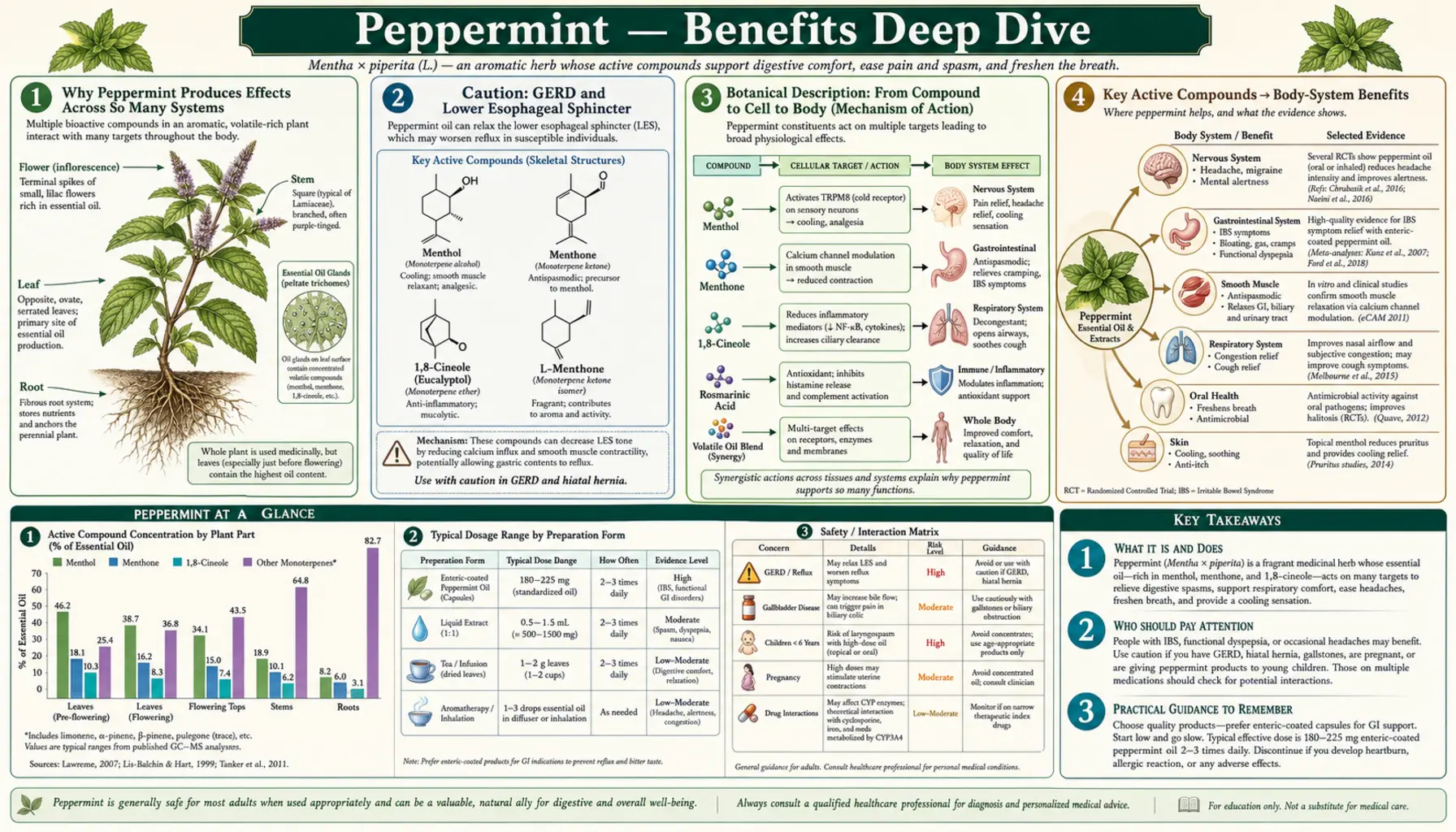
Most medicinal herbs have a single dominant clinical effect, with everything else being secondary or speculative. Peppermint is unusual because a single molecule — L-menthol — produces four distinct and well-documented clinical effects through three different pharmacological mechanisms. Each mechanism maps to a separate category of clinical use, and understanding the mechanism explains why the indication works (and why some indications fail).
- Voltage-gated calcium channel blockade in smooth muscle — L-menthol inhibits L-type calcium channels in intestinal smooth muscle, reducing calcium influx required for contraction. This is the same fundamental mechanism as the dihydropyridine calcium-channel-blocker drug class (nifedipine, amlodipine) used for hypertension, but localized to the gut when peppermint oil is delivered via enteric-coated capsule. The result is direct antispasmodic action on intestinal smooth muscle — the mechanism behind the strong irritable bowel syndrome and functional dyspepsia evidence base.
- TRPM8 cold-receptor activation — menthol is the prototypical TRPM8 agonist; TRPM8 is the same ion channel activated by physical cold (temperatures below approximately 26°C). Activation produces three downstream effects: (a) a subjective sensation of cooling in the area exposed (the source of mint's "refreshing" quality), (b) a counter-irritant effect that crowds out competing pain signals when applied topically (the mechanism behind peppermint oil for tension headache), and (c) a subjective sensation of airflow when activated on nasal mucosa even without objective increase in airflow (the mechanism behind the menthol decongestant effect).
- Trigeminal nerve arousal via nasal irritant activation — when inhaled, menthol activates the trigeminal nerve (cranial nerve V) at its branches in the nasal cavity, producing a mild irritant signal that increases central nervous system arousal independently of classical olfaction. This is the mechanism behind peppermint's alertness-enhancing effect on working-memory and sustained-attention tasks — the "wake me up" quality that distinguishes mint from purely-olfactory pleasant scents like vanilla or lavender.
A unifying feature is that all three mechanisms are reversible, peripheral, and non-receptor-saturating. There is no tolerance build-up to peppermint with daily use the way there is with central-acting sedatives or stimulants. There is no withdrawal syndrome on discontinuation. And the safety profile is excellent across normal dose ranges — the principal cautions are the GERD/reflux exacerbation from lower-esophageal-sphincter relaxation (a fourth, more subtle mechanism), infant laryngospasm risk from menthol exposure, and the biliary-colic risk in patients with gallstones.
Research Papers: IBS & Digestive
- Khanna R, MacDonald JK, Levesque BG (2014). Peppermint oil for the treatment of irritable bowel syndrome: a systematic review and meta-analysis — PubMed: Khanna 2014 IBS meta-analysis
- Alammar N et al. (2019). The impact of peppermint oil on the irritable bowel syndrome: a meta-analysis of the pooled clinical data — PubMed: Alammar 2019 IBS meta-analysis
- Pittler MH, Ernst E (1998). Peppermint oil for irritable bowel syndrome: a critical review and meta-analysis — PubMed: Pittler 1998
- L-menthol voltage-gated calcium channel blockade in smooth muscle — PubMed: Menthol calcium channel
- IBgard sustained-release microsphere peppermint formulation trial — PubMed: IBgard formulation
- ACG Clinical Guideline endorsement of peppermint oil for IBS — PubMed: ACG IBS guideline
- Peppermint and caraway combination for functional dyspepsia — PubMed: Peppermint and caraway dyspepsia
- Iberogast STW 5 herbal combination for functional GI disorders — PubMed: Iberogast trials
- Peppermint oil pre-endoscopy antispasmodic use — PubMed: Peppermint for endoscopy
- SIBO and herbal antimicrobial regimens including peppermint — PubMed: SIBO herbal antimicrobials
Research Papers: Headache
- Göbel H, Schmidt G, Soyka D (1994). Effect of peppermint and eucalyptus oil preparations on neurophysiological and experimental algesimetric headache parameters — PubMed: Göbel 1994 mechanism
- Göbel H et al. (1996). Effectiveness of Oleum menthae piperitae and paracetamol in therapy of headache of the tension type — PubMed: Göbel 1996 acetaminophen trial
- TRPM8 cold receptor activation by menthol and counter-irritant mechanism — PubMed: TRPM8 counter-irritant
- Borhani Haghighi A et al. (2010). Cutaneous application of menthol for migraine prophylaxis — PubMed: Menthol for migraine
- Peppermint oil topical dilution and skin tolerance studies — PubMed: Topical peppermint dilution
Research Papers: Respiratory & Cough
- Ahmed A et al. (2007). Menthol and inhaled nasal sensation of airflow — PubMed: Menthol airflow sensation
- Eccles R (2003). Menthol and related cooling compounds — PubMed: Eccles menthol cooling
- Menthol antitussive activity and cough reflex suppression — PubMed: Menthol antitussive
- Vicks VapoRub menthol-camphor-eucalyptus cough rub clinical trials — PubMed: Vapor rub trials
- Menthol-related laryngospasm and infant safety warnings — PubMed: Infant menthol safety
Research Papers: Cognitive & Alertness
- Moss M et al. (2008). Modulation of cognitive performance and mood by aromas of peppermint and ylang-ylang — PubMed: Moss 2008 cognitive
- Peppermint aroma and sustained attention / driving alertness — PubMed: Peppermint and driving
- Trigeminal nerve activation by menthol vs olfactory processing — PubMed: Trigeminal vs olfactory
- Peppermint chewing gum and cognitive function studies — PubMed: Peppermint gum cognition
- Aromatherapy and athletic / physical performance with peppermint — PubMed: Peppermint and exercise
Caution: GERD and Lower Esophageal Sphincter
The most consequential caution for peppermint use is its relaxant effect on the lower esophageal sphincter (LES). The same smooth-muscle calcium-channel blockade that produces antispasmodic relief in the gut also reduces the resting tone of the LES — the muscular ring that prevents stomach acid from refluxing into the esophagus. In patients with gastroesophageal reflux disease (GERD), hiatal hernia, or symptomatic acid reflux, peppermint can worsen symptoms by allowing more gastric content to enter the lower esophagus.
This is the single most common scenario in which peppermint goes from helpful to harmful. A patient with overlapping IBS and GERD (a common combination — both involve visceral hypersensitivity and autonomic dysregulation) may try peppermint tea or peppermint oil capsules for IBS symptoms and find that reflux worsens substantially. The IBS evidence base does not necessarily translate to this subpopulation. Practical guidance:
- Avoid in known GERD or hiatal hernia. The reflux exacerbation is reliable and dose-dependent.
- Enteric coating partially helps but does not eliminate the risk. The coating delays release until the small intestine, but absorbed menthol can still circulate systemically and reduce LES tone.
- Discontinue if heartburn appears after starting peppermint. The effect is typically apparent within the first 1-2 weeks of use.
- Substitute alternatives for IBS in GERD patients. Ginger, fennel, soluble fiber (psyllium), and the Low-FODMAP diet are reasonable substitutes that do not relax the LES.
The other significant cautions — gallstones (biliary colic risk from increased bile flow), infants and very young children (menthol laryngospasm risk), and pregnancy (high-dose essential oil use only) — are covered in detail on the main Peppermint page.
External Authoritative Resources
- NCCIH — Peppermint Oil — National Center for Complementary and Integrative Health summary
- MedlinePlus — Peppermint (Natural)
- StatPearls — Menthol (Bookshelf NCBI overview of menthol pharmacology and clinical use)
- European Medicines Agency — Peppermint Oil (Menthae piperitae aetheroleum) monograph
- PubMed — All research on Mentha × piperita
Connections
- Peppermint (Main Page)
- Peppermint for IBS & Digestive
- Peppermint for Headache Relief
- Peppermint for Respiratory & Cough
- Peppermint for Cognitive & Alertness
- All Herbs
- Ginger
- Fennel
- Chamomile
- Lemon Balm
- Eucalyptus
- Irritable Bowel Syndrome
- SIBO
- Migraine
- Headache
- Sinusitis
- Gut Healing