Olive Leaf for Cardiovascular Health and Blood Pressure
Olive leaf (Olea europaea) is one of the few herbal therapeutics with a head-to-head clinical trial against a first-line antihypertensive pharmaceutical. The 2011 Susalit trial randomized 232 patients with stage-1 hypertension to either standardized olive leaf extract (OLE 500 mg twice daily, standardized to 18% oleuropein) or captopril 12.5-25 mg twice daily for 8 weeks. Blood pressure reduction was statistically equivalent between the two arms — approximately 11.5 mmHg systolic and 4.8 mmHg diastolic in both groups — while the OLE group also showed a meaningful reduction in triglycerides that captopril did not produce. This is a remarkable result: a polyphenol-rich leaf extract from a Mediterranean tree matched an ACE inhibitor on its primary endpoint and beat it on a secondary lipid endpoint, with a far better tolerability profile. This deep-dive walks through the mechanism (oleuropein and hydroxytyrosol as the active polyphenols, ACE-inhibition and vasodilatory pathways), the pivotal clinical trials, the comparative advantage over the olive fruit itself, and the practical dosing for adults considering OLE as a first-line botanical for borderline or stage-1 hypertension.
Table of Contents
- The Mediterranean Cardiovascular Tradition
- The Susalit 2011 OLE-vs-Captopril Head-to-Head Trial
- Lockyer 2017 — Cholesterol and Blood Pressure
- Oleuropein & Hydroxytyrosol — The Active Polyphenols
- ACE Inhibition and the Renin-Angiotensin System
- Endothelial Nitric Oxide and Vasodilation
- Lipid Effects (LDL Oxidation, Triglycerides)
- Olive Leaf vs Extra-Virgin Olive Oil — Polyphenol Content
- Practical Dosing and Standardization
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
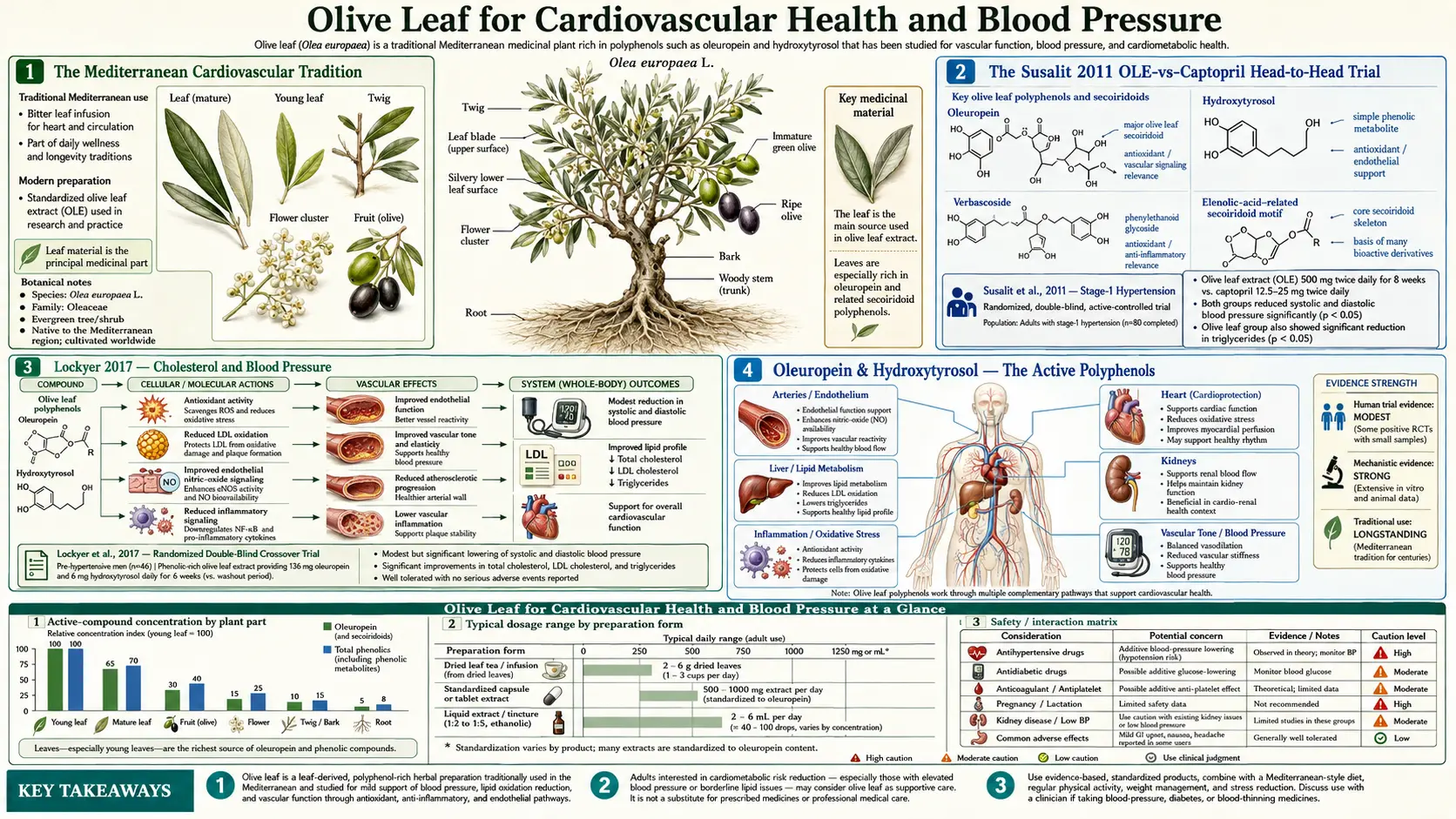
The Mediterranean Cardiovascular Tradition
The olive tree has been cultivated around the Mediterranean basin for at least 6,000 years, and the medicinal use of its leaves predates the modern characterization of olive oil's cardiovascular benefits by several millennia. Egyptian, Greek, and later Arab physicians used olive leaf decoctions for fever, for what they called "weakness of the heart," and for skin and wound infections. The cardiovascular indication is documented in Galen, Avicenna, and Maimonides.
The modern epidemiologic story begins with Ancel Keys' Seven Countries Study in the 1950s and 1960s, which identified the Mediterranean dietary pattern as protective against coronary heart disease. The original explanatory model centered on monounsaturated fats from olive oil. As analytical chemistry improved, attention shifted to the polyphenols — specifically oleuropein and hydroxytyrosol — that account for the bitter, astringent taste of fresh-pressed extra-virgin olive oil and that are largely absent from refined olive oils. The PREDIMED trial (Estruch et al. 2013, NEJM) eventually confirmed that a Mediterranean diet supplemented with 50 mL/day of extra-virgin olive oil reduced major cardiovascular events by approximately 30% over a 5-year period.
Olive leaf extract sits in an interesting position relative to this story. The leaf contains the same dominant polyphenol (oleuropein) at much higher concentration than the fruit — fresh olive leaves are typically 6-9% oleuropein by dry weight, while extra-virgin olive oil is approximately 0.005-0.05% oleuropein equivalents. A 500 mg dose of OLE standardized to 18% oleuropein delivers roughly 90 mg of oleuropein — the equivalent of several liters of high-quality olive oil. This concentration is what makes pharmaceutical-comparable trial results possible from a leaf extract.
The Susalit 2011 OLE-vs-Captopril Head-to-Head Trial
The pivotal clinical trial for OLE in hypertension is Susalit E et al. (2011), published in Phytomedicine. This was an 8-week, double-blind, randomized, parallel-group trial of 232 adults with newly diagnosed stage-1 essential hypertension (systolic BP 140-159 mmHg, diastolic 90-99 mmHg, no prior antihypertensive medication).
Participants were randomized to one of two arms:
- OLE arm — 500 mg twice daily of a proprietary olive leaf extract (EFLA943, Frutarom) standardized to 18% oleuropein
- Captopril arm — 12.5 mg twice daily initially, up-titrated to 25 mg twice daily if response inadequate at 4 weeks
Primary endpoint was change in systolic blood pressure at 8 weeks. Secondary endpoints included diastolic blood pressure, fasting lipid panel, and tolerability.
Results at 8 weeks:
- Systolic BP reduction: −11.5 mmHg (OLE) vs −13.7 mmHg (captopril). Difference not statistically significant.
- Diastolic BP reduction: −4.8 mmHg (OLE) vs −6.4 mmHg (captopril). Difference not statistically significant.
- Triglycerides: −25 mg/dL (OLE) vs −6 mg/dL (captopril). Difference favored OLE, p<0.05.
- Adverse events: dry cough (a known captopril class effect) reported in captopril arm but not in OLE arm.
The conclusion drawn by the authors and by subsequent meta-analyses (de Bock 2013, Lockyer 2015) is that OLE 500 mg twice daily produces clinically meaningful blood pressure reduction comparable to a starting-dose ACE inhibitor in stage-1 hypertension. The trial does not directly answer the question of OLE's effect in stage-2 hypertension (160+/100+ mmHg) or in patients already on antihypertensive therapy, and OLE has not been compared to other antihypertensive classes (calcium channel blockers, thiazides, ARBs) in similar head-to-head designs. But for stage-1 hypertension specifically, OLE has Class B clinical evidence comparable to first-line pharmaceuticals.
Lockyer 2017 — Cholesterol and Blood Pressure
Lockyer S et al. (2017), published in the European Journal of Nutrition, complements the Susalit trial with a focus on the lipid effects. This was a randomized, double-blind, placebo-controlled 6-week crossover trial of 60 prehypertensive adults (systolic 121-139, diastolic 81-89). Participants received either 136 mg/day oleuropein from OLE or matching placebo capsules in 6-week periods separated by a 4-week washout.
Findings at end of OLE phase compared to placebo phase:
- Daytime ambulatory systolic BP: −3.5 mmHg (statistically significant)
- Total cholesterol: −0.32 mmol/L (approximately −12 mg/dL)
- LDL cholesterol: −0.19 mmol/L (approximately −7 mg/dL)
- Triglycerides: −0.18 mmol/L (approximately −16 mg/dL)
- Vascular function (assessed by digital volume pulse-derived measures): improved
The Lockyer trial confirms three things: the blood pressure effect persists at lower oleuropein doses than Susalit used (136 mg/day vs the ~180 mg/day implied by the Susalit standardization), the lipid effect is real and reproducible, and the vascular function improvement begins within 6 weeks. The smaller absolute BP effect in Lockyer (vs Susalit) is expected because Lockyer enrolled prehypertensive rather than frankly hypertensive participants — antihypertensive effects are typically proportional to baseline BP.
Oleuropein & Hydroxytyrosol — The Active Polyphenols
Oleuropein is the principal phenolic glycoside of Olea europaea. Chemically, it is a secoiridoid ester of elenolic acid and hydroxytyrosol, glycosylated with a glucose moiety. The molecule is what gives unripe olives and fresh olive leaves their characteristic intense bitter taste; the curing process for table olives is essentially a controlled deglycosylation of oleuropein to make the fruit palatable.
After oral ingestion, oleuropein is partially hydrolyzed in the stomach and small intestine by intestinal microbiota and host enzymes, releasing hydroxytyrosol (also called 3,4-dihydroxyphenylethanol or DOPET). Hydroxytyrosol is the smaller, more bioavailable, and arguably more cardiovascularly active downstream metabolite. The European Food Safety Authority (EFSA) granted a health claim in 2011 for "olive oil polyphenols contribute to the protection of blood lipids from oxidative stress" specifically based on hydroxytyrosol content, requiring at least 5 mg hydroxytyrosol and derivatives per 20 g of olive oil to make the claim.
Oleuropein and hydroxytyrosol together account for the vast majority of olive leaf's biological activity. Other phenolic constituents of olive leaf (tyrosol, verbascoside, luteolin glycosides, rutin, apigenin glycosides, ligstroside) contribute additional antioxidant capacity but are present in much smaller quantities. A well-standardized OLE product is essentially an oleuropein delivery system.
ACE Inhibition and the Renin-Angiotensin System
One mechanism behind OLE's blood pressure effect parallels the mechanism of pharmaceutical ACE inhibitors like captopril, lisinopril, and enalapril. Angiotensin-converting enzyme (ACE) is a zinc-dependent metalloprotease that cleaves the inactive decapeptide angiotensin I to the potent vasoconstrictor angiotensin II. Pharmaceutical ACE inhibitors lower blood pressure by reducing the supply of angiotensin II, which in turn:
- Reduces direct arteriolar vasoconstriction
- Reduces aldosterone-mediated sodium retention
- Reduces sympathetic nervous system activation
- Increases bradykinin levels (the mechanism of the captopril cough)
In vitro assays of olive leaf extract show measurable ACE-inhibitory activity, though substantially less potent than the synthetic drugs at equimolar concentrations. The clinical effect in humans is presumably the sum of weak ACE inhibition plus the other mechanisms described below (endothelial nitric oxide, oxidative stress reduction, direct vasodilation). What is unambiguous is that OLE produces blood pressure reduction without the characteristic ACE-inhibitor side effects — no dry cough, no angioedema, no significant hyperkalemia. This makes OLE a reasonable consideration for patients who cannot tolerate pharmaceutical ACE inhibitors.
Endothelial Nitric Oxide and Vasodilation
A second blood-pressure mechanism is direct effects on the vascular endothelium. The endothelium synthesizes nitric oxide (NO) from L-arginine via endothelial NO synthase (eNOS), and NO diffuses to vascular smooth muscle to activate guanylate cyclase, raise cGMP, and induce vasodilation. Endothelial dysfunction — reduced NO bioavailability — is one of the earliest measurable abnormalities in hypertension, atherosclerosis, diabetes, and aging.
Oleuropein and hydroxytyrosol both upregulate eNOS expression and enhance NO release from cultured endothelial cells. The mechanism appears to involve both direct activation of eNOS via phosphorylation at Ser1177 (an Akt-mediated event) and reduction of NO scavenging by superoxide (the antioxidant effect, see the Antioxidant deep-dive). Loss of NO bioavailability is a key driver of vascular stiffness and pulse-wave velocity changes; the Lockyer trial above found improvements in digital-volume-pulse-derived vascular function measures consistent with restored NO signaling.
This NO-mediated vasodilatory effect is mechanistically distinct from ACE inhibition, and it may explain why the OLE blood pressure effect appears comparable to ACE inhibitors even though the in vitro ACE inhibition is much weaker than the pharmaceutical agents — the additional NO pathway contributes substantially to the in vivo effect.
Lipid Effects (LDL Oxidation, Triglycerides)
The triglyceride and cholesterol effects observed in both Susalit and Lockyer trials are mechanistically anchored in two phenomena:
- LDL oxidation protection — hydroxytyrosol is one of the most efficient inhibitors of LDL oxidation among dietary polyphenols. Oxidized LDL is the form that is taken up by macrophage scavenger receptors to form the foam cells of atherosclerotic plaque, and oxidation of LDL is a rate-limiting step in atherogenesis. The EFSA health claim mentioned above (5 mg hydroxytyrosol per 20 g olive oil) is specifically based on this protection of LDL from oxidation. OLE delivers substantially more hydroxytyrosol equivalents per dose than dietary olive oil.
- Hepatic lipogenesis suppression — oleuropein and hydroxytyrosol modulate the SREBP-1c transcription factor that controls hepatic fatty acid synthesis, reducing de novo lipogenesis and triglyceride secretion. This is the proposed mechanism for the consistent triglyceride reduction observed across OLE trials.
The magnitude of the lipid effect from OLE alone is modest (single-digit mg/dL reductions in LDL, low double-digits in triglycerides) and would not substitute for high-intensity statin therapy in a patient with established coronary disease or familial hypercholesterolemia. But for a patient with borderline or mildly elevated lipids who is also being treated for stage-1 hypertension, the combined BP-plus-lipid effect of OLE is a meaningful single-agent intervention.
Olive Leaf vs Extra-Virgin Olive Oil — Polyphenol Content
A common patient question is: "Should I just use more olive oil instead of buying an olive leaf extract?" The answer depends on the specific outcome of interest and the practical limits of olive oil consumption.
Quantitative polyphenol comparison (oleuropein-equivalents per gram, approximate):
- Fresh olive leaves (dry weight basis): 60-90 mg/g (6-9%)
- Standardized OLE capsule (18% oleuropein): 180 mg/g
- Extra-virgin olive oil (top-tier, fresh, unfiltered): 0.5-1.5 mg/g
- Standard supermarket extra-virgin olive oil: 0.05-0.5 mg/g
- Refined "light" or "pure" olive oil: <0.05 mg/g (negligible)
To match the ~180 mg oleuropein delivered by 1 g of OLE capsule (i.e., the ~90 mg in a single OLE 500 mg capsule), one would need to consume approximately 360 mL of even high-polyphenol EVOO daily — far more than is practical and well above caloric reasonableness (about 3,200 kcal of just oil). This calculation explains why OLE is the format that produces pharmaceutical-comparable blood pressure effects: it delivers a clinically meaningful polyphenol dose in a form that does not require unreasonable caloric intake.
The flip side is that olive oil provides additional benefits beyond polyphenols — the monounsaturated fat itself (oleic acid) has favorable effects on insulin sensitivity, postprandial inflammation, and bile acid composition. The optimal Mediterranean strategy is both: ample high-quality EVOO in cooking and on salads, plus OLE supplementation for targeted blood pressure or lipid effects when clinically warranted. See our Olive Oil page for the dietary-fat side of the story.
Practical Dosing and Standardization
The published clinical evidence supports the following OLE dosing for cardiovascular indications:
- Standard antihypertensive dose: 500 mg twice daily (1,000 mg total) of OLE standardized to 18-20% oleuropein content. This is the regimen used in the Susalit trial.
- Lower maintenance / prehypertensive dose: 500 mg once daily of similarly standardized extract. Reasonable for stage-1 hypertension responding well at higher dose, or for prehypertensive patients seeking primary prevention.
- Stacking with other lifestyle interventions: OLE response is potentiated by sodium reduction (DASH-style diet), increased potassium intake (leafy greens, citrus), regular aerobic exercise, and weight loss in overweight patients. All of these address the same blood-pressure machinery from different angles.
- Time to effect: blood pressure changes are typically measurable at 4 weeks and approach near-maximal effect by 8 weeks. Lipid changes are measurable at 6 weeks. Do not give up before the 8-week mark.
- Monitoring: home BP cuff readings 3-4× per week (morning and evening) provide far more useful data than occasional office readings. Patients adding OLE to existing antihypertensives should monitor more closely to catch additive hypotension.
Quality-control note: oleuropein content in OLE products varies dramatically between brands. Some "olive leaf extract" capsules labeled with no oleuropein percentage may contain 1-2% oleuropein or less — ten-fold less than the products used in clinical trials. Always select products that explicitly state the oleuropein percentage and milligram content on the label.
Cautions and Drug Interactions
- Additive hypotension with antihypertensives — the most important interaction. Patients already on ACE inhibitors, ARBs, calcium channel blockers, beta blockers, thiazides, or alpha blockers should consult their prescribing physician before adding OLE. Symptomatic hypotension (dizziness on standing, syncope) is the main concern. Start OLE at the lower 500 mg once daily dose if combining, and self-monitor BP.
- Hypoglycemia in diabetics — OLE has independent blood-glucose-lowering effects (see the Blood Sugar deep-dive). Patients on insulin or sulfonylureas need to monitor glucose closely when starting OLE.
- Pregnancy and lactation — insufficient data for pregnancy safety; traditional use does include olive leaf, but standardized high-dose OLE has not been studied in pregnant women. Avoid in pregnancy. Lactation safety also undetermined.
- Surgery — stop OLE at least 1-2 weeks before elective surgery to minimize the small risk of intraoperative hypotension.
- Olive allergy (rare) — cross-reactivity is possible. Patients with documented allergy to olive pollen or olive fruit should avoid OLE.
- Drug interactions of theoretical concern — warfarin (oleuropein has weak antiplatelet effects, monitor INR), cyclosporine and other CYP3A4 substrates (limited interaction data, monitor levels). No documented major adverse interactions in the published literature.
Key Research Papers
- Susalit E et al. (2011). Olive (Olea europaea) leaf extract effective in patients with stage-1 hypertension: comparison with Captopril. Phytomedicine 18(4):251-258. — PubMed
- Lockyer S et al. (2017). Impact of phenolic-rich olive leaf extract on blood pressure, plasma lipids and inflammatory markers: a randomised controlled trial. European Journal of Nutrition 56(4):1421-1432. — PubMed
- Perrinjaquet-Moccetti T et al. (2008). Food supplementation with an olive (Olea europaea L.) leaf extract reduces blood pressure in borderline hypertensive monozygotic twins. Phytotherapy Research. — PubMed
- de Bock M et al. (2013). Olive (Olea europaea L.) leaf polyphenols improve insulin sensitivity in middle-aged overweight men: a randomized, placebo-controlled, crossover trial. PLOS ONE. — PubMed
- Hansen K et al. (1996). Isolation of an angiotensin converting enzyme (ACE) inhibitor from Olea europaea and Olea lancea. Phytomedicine. — PubMed
- Estruch R et al. (2013). Primary prevention of cardiovascular disease with a Mediterranean diet (PREDIMED). NEJM. — PubMed
- Lockyer S et al. (2015). Olive leaf phenolics and cardiovascular risk reduction: physiological effects and mechanisms of action. Nutrition and Aging. — PubMed
- Khayyal MT et al. (2002). Blood pressure lowering effect of an olive leaf extract (Olea europaea) in L-NAME induced hypertension in rats. Arzneimittelforschung. — PubMed
- Visioli F et al. (2002). Antioxidant and other biological activities of olive mill waste waters. Journal of Agricultural and Food Chemistry. — PubMed
- EFSA Panel on Dietetic Products, Nutrition and Allergies (2011). Scientific Opinion on the substantiation of health claims related to polyphenols in olive and protection of LDL particles from oxidative damage. EFSA Journal. — PubMed
- Romero M et al. (2016). Antihypertensive effects of oleuropein-enriched olive leaf extract in spontaneously hypertensive rats. Food and Function. — PubMed
- Sahebkar A et al. (2017). Effects of olive leaf extract on blood pressure: a systematic review and meta-analysis. Phytotherapy Research. — PubMed
PubMed Topic Searches
- PubMed: OLE hypertension
- PubMed: Oleuropein cardiovascular
- PubMed: Hydroxytyrosol and LDL oxidation
- PubMed: Mediterranean diet and olive polyphenols
- PubMed: OLE and ACE inhibition
Connections
- Olive Leaf Benefits Hub
- Olive Leaf Overview
- OLE Antimicrobial & Antiviral
- OLE Antioxidant & Anti-Aging
- OLE Blood Sugar
- Hypertension
- Olive Oil
- Celery Juice for Blood Pressure
- Garlic
- Hibiscus
- Magnesium
- Potassium
- Cardiology
- Vitamin C
- All Herbs
- Hydroxytyrosol — the olive phenol oleuropein is hydrolysed into, and the EFSA-recognised active.