Olive Leaf for Blood Sugar and Insulin Sensitivity
The Wainstein 2012 trial published in Journal of Medicinal Food randomized 79 prediabetic adult patients to olive leaf extract (OLE 500 mg twice daily) or matching placebo for 14 weeks, with insulin sensitivity assessed by HOMA-IR, fasting glucose, fasting insulin, and HbA1c. The OLE group showed statistically significant improvements in insulin sensitivity (HOMA-IR decreased by approximately 15%), pancreatic beta-cell responsiveness, and HbA1c trend, with no comparable change in the placebo arm. Mechanistically, oleuropein has been shown to act as both an insulin secretagogue (potentiating glucose-stimulated insulin release from pancreatic beta cells, a mechanism similar to but milder than sulfonylureas) and as an insulin sensitizer in peripheral tissues (skeletal muscle, adipose, liver). The dual mechanism is uncommon among herbal therapeutics and is the foundation for OLE's emerging role in prediabetes management and as an adjunct to lifestyle intervention in early type 2 diabetes. This deep-dive walks through the Wainstein trial, the insulin secretagogue and sensitization mechanisms, the GLP-1 and gut microbiome contributions, the stacking with metformin and lifestyle, and the practical dosing for adults with prediabetes or metabolic syndrome.
Table of Contents
- The Prediabetes Treatment Gap
- Wainstein 2012 — The Prediabetic Insulin Sensitivity Trial
- Oleuropein as Insulin Secretagogue
- Oleuropein and Hydroxytyrosol as Insulin Sensitizers
- GLP-1 and the Gut Microbiome Contribution
- Postprandial Glucose Modulation
- HbA1c, Fasting Glucose, and Long-Term Markers
- Stacking with Metformin and Lifestyle Intervention
- Practical Dosing and Monitoring
- Cautions (Hypoglycemia, Drug Interactions)
- Key Research Papers
- Connections
- Featured Videos
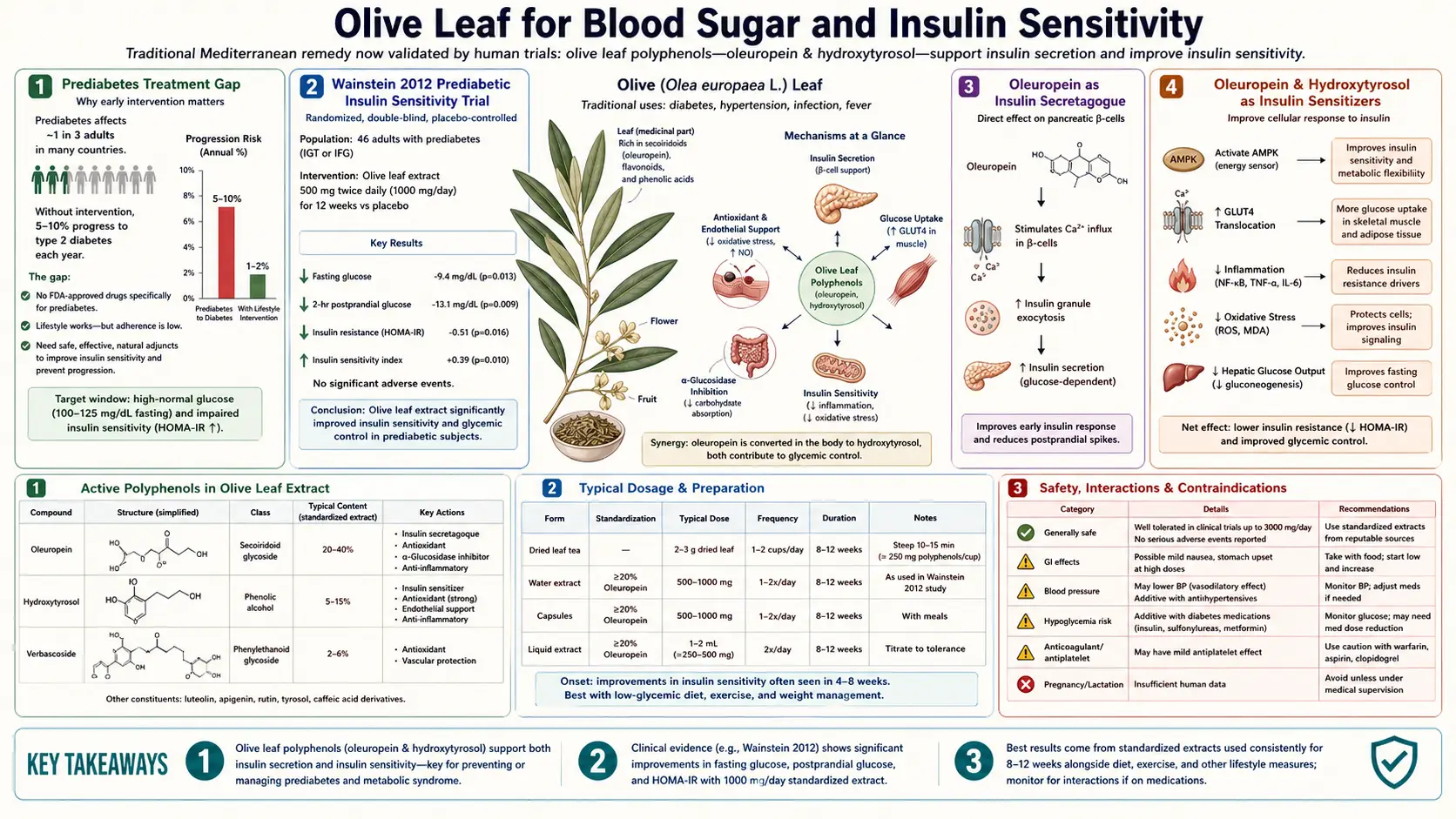
The Prediabetes Treatment Gap
Prediabetes — HbA1c 5.7-6.4% or fasting glucose 100-125 mg/dL or impaired glucose tolerance on OGTT — affects approximately 96 million American adults (more than one in three) and a much larger fraction of overweight middle-aged adults globally. Most progress to overt type 2 diabetes within 10 years if no intervention is undertaken; conversely, robust lifestyle intervention (the Diabetes Prevention Program protocol of 7% weight loss plus 150 minutes weekly of moderate exercise) reduces 3-year progression by approximately 58%, and metformin reduces it by approximately 31%.
The clinical gap is large. Lifestyle intervention works but is hard to sustain at the population level. Metformin is well-tolerated and effective but underprescribed in prediabetes outside of high-risk populations. Many patients sit in a "watching and waiting" zone where they know they have prediabetes but receive no specific pharmacotherapy and inconsistent lifestyle counseling. This is the population for whom carefully evidence-aligned herbal interventions like OLE are most relevant: a mild but real metabolic effect, favorable safety profile, no requirement for a prescription, and complementary mechanism to dietary and lifestyle approaches.
OLE does not replace lifestyle intervention or metformin where indicated. But for prediabetic adults already pursuing lifestyle change who want a targeted supplemental support, the evidence base — led by the Wainstein 2012 trial — is among the strongest for any herbal monotherapy in this space.
Wainstein 2012 — The Prediabetic Insulin Sensitivity Trial
Wainstein J, Ganz T, Boaz M et al. (2012), published in Journal of Medicinal Food, is the pivotal human trial for OLE in insulin sensitivity. Design: 14-week randomized, double-blind, placebo-controlled trial in 79 adults with insulin resistance (mean fasting insulin ~10 µIU/mL, mean HOMA-IR ~2.5), randomized to:
- OLE arm — 500 mg twice daily of olive leaf extract standardized to 18% oleuropein (EFLA943, Frutarom; same proprietary preparation as Susalit's hypertension trial)
- Placebo arm — matching capsules
Primary endpoint was change in insulin sensitivity assessed by HOMA-IR (homeostatic model assessment of insulin resistance), with secondary endpoints of fasting glucose, fasting insulin, glucose-stimulated insulin response, lipid panel, and inflammatory markers.
Results at 14 weeks:
- HOMA-IR: reduced by approximately 15% in the OLE arm vs no change in placebo; p<0.05
- Pancreatic beta-cell responsiveness: improved second-phase insulin secretion in response to glucose challenge in OLE arm
- HbA1c trend: small reduction (-0.16% absolute) in OLE arm vs slight increase in placebo, though not the primary endpoint
- Fasting glucose: small reduction in OLE arm not reaching statistical significance
- Lipid panel: triglycerides reduced (consistent with the cardiovascular trials)
- Safety: no serious adverse events; no symptomatic hypoglycemia
The interpretation is that OLE 1,000 mg/day produces a clinically meaningful improvement in insulin sensitivity in a 14-week trial in insulin-resistant but non-diabetic adults. The magnitude is roughly comparable to a 5-7% weight loss or to low-dose metformin, smaller than the effect of high-intensity lifestyle intervention or full-dose metformin (2,000 mg/day). The mechanism appears to be both peripheral insulin sensitization and improved beta-cell responsiveness.
Oleuropein as Insulin Secretagogue
Pancreatic beta cells release insulin in response to glucose via a well-characterized mechanism: glucose enters the beta cell via GLUT2, is phosphorylated by glucokinase, enters glycolysis and the TCA cycle, raises intracellular ATP/ADP ratio, closes the ATP-sensitive potassium channel (KATP), depolarizes the beta cell membrane, opens voltage-gated calcium channels, and the calcium influx triggers insulin granule exocytosis.
Sulfonylureas (glipizide, glyburide, glimepiride) are insulin secretagogues that work by directly closing the KATP channel via the sulfonylurea receptor (SUR1) subunit, bypassing the need for glucose-driven ATP. This produces strong glucose-lowering but also hypoglycemia risk because the secretagogue effect is not glucose-dependent.
Oleuropein and its hydrolysis products show insulin-secretagogue activity in isolated pancreatic islet preparations and in beta-cell line studies (INS-1, MIN6). The mechanism appears more nuanced than sulfonylureas:
- Oleuropein enhances glucose-stimulated insulin release without producing major insulin release at baseline (i.e., the effect is largely glucose-dependent, not the sulfonylurea-style indiscriminate release). This is why OLE has not produced symptomatic hypoglycemia in trials — the secretagogue effect amplifies the appropriate physiologic response rather than overriding it.
- Oleuropein supports beta-cell mitochondrial function and reduces glucotoxicity-induced beta-cell apoptosis, preserving long-term beta-cell mass
- Oleuropein may modestly inhibit dipeptidyl peptidase-4 (DPP-4), the enzyme that degrades GLP-1, indirectly raising GLP-1 levels and supporting glucose-dependent insulin secretion
The clinical implication is that OLE's effect on insulin secretion is gentler and safer than pharmaceutical sulfonylureas, but mechanistically similar in direction. For prediabetes and early type 2 diabetes where some beta-cell function is preserved, this is a useful effect.
Oleuropein and Hydroxytyrosol as Insulin Sensitizers
Beyond the secretagogue effect at the beta cell, OLE improves insulin signaling in peripheral target tissues: skeletal muscle, adipose tissue, and liver. The mechanisms include:
- Insulin receptor substrate (IRS) phosphorylation — hydroxytyrosol enhances tyrosine phosphorylation of IRS-1 and IRS-2 in response to insulin binding, preserving the downstream PI3K/Akt signaling that translocates GLUT4 glucose transporters to the cell membrane
- Reduced serine phosphorylation of IRS — inflammatory signaling (JNK, IKK-beta) drives inhibitory serine phosphorylation of IRS proteins, blocking the insulin signal. Hydroxytyrosol's anti-inflammatory effects reduce this inhibitory signal.
- AMPK activation — oleuropein and hydroxytyrosol both activate AMP-activated protein kinase (AMPK), the cellular energy sensor, in skeletal muscle and hepatocytes. AMPK activation increases GLUT4 translocation independently of insulin, increases fatty acid oxidation, and inhibits hepatic gluconeogenesis. This is essentially the same mechanism as metformin.
- Improved mitochondrial function and reduced lipotoxicity — the mitochondrial protection discussed in the Antioxidant deep-dive reduces intramyocellular lipid accumulation, which is a key driver of muscle insulin resistance
- Reduced hepatic lipogenesis — oleuropein modulates SREBP-1c, reducing de novo lipogenesis and hepatic triglyceride accumulation. Reduced hepatic fat is associated with restored hepatic insulin sensitivity.
The combination of beta-cell support plus peripheral sensitization is mechanistically attractive for prediabetes specifically, because both pathologies (relative beta-cell insufficiency and peripheral insulin resistance) are present in the prediabetic state and worsen as the patient progresses to overt diabetes.
GLP-1 and the Gut Microbiome Contribution
A more recent line of research suggests that OLE's metabolic benefits are partly mediated through the gut. Two mechanisms:
- GLP-1 (glucagon-like peptide-1) elevation — GLP-1 is an incretin hormone secreted by intestinal L cells in response to nutrient intake. It potentiates glucose-stimulated insulin secretion, suppresses glucagon, slows gastric emptying, and increases satiety. The GLP-1 axis is the target of GLP-1 receptor agonists like semaglutide and liraglutide, currently the most clinically transformative new drug class for type 2 diabetes and obesity. Olive polyphenols including oleuropein appear to stimulate L-cell GLP-1 secretion modestly, and to inhibit GLP-1 breakdown by DPP-4 (the same enzyme inhibited by sitagliptin and the other "gliptin" class drugs).
- Gut microbiome modulation — OLE produces favorable shifts in gut microbiome composition in both animal and limited human studies, including increases in Akkermansia muciniphila (a bacterium associated with metabolic health), Lactobacillus species, and short-chain-fatty-acid-producing Firmicutes. The metabolic implications of these microbiome changes include improved gut barrier integrity (less metabolic endotoxemia), increased butyrate production (with downstream effects on hepatic insulin sensitivity), and indirect modulation of GLP-1 secretion via bile acid signaling through TGR5 and FXR receptors.
The GLP-1 and microbiome mechanisms are mechanistically interesting and partially explain why OLE's effects extend beyond a simple "polyphenol antioxidant" framework. The magnitude of the GLP-1 elevation from OLE is much smaller than from pharmaceutical GLP-1 agonists, and OLE should not be expected to produce semaglutide-like weight loss, but the directional alignment with one of the most clinically successful diabetes drug classes is encouraging.
Postprandial Glucose Modulation
Continuous glucose monitor (CGM) studies show that OLE taken before a meal modestly reduces the postprandial glucose excursion. The mechanism appears to combine three effects:
- Mild inhibition of intestinal alpha-amylase and alpha-glucosidase activity, slowing carbohydrate digestion (a milder version of the acarbose mechanism)
- Enhanced first-phase insulin response to the meal
- Slowed gastric emptying via the GLP-1 mechanism
For patients using CGM to optimize glucose control, OLE 500 mg taken 30 minutes before a carbohydrate-containing meal produces a measurable reduction in peak glucose (typically 10-20 mg/dL lower peak) and a flatter excursion curve. This effect is modest compared to pharmaceutical alpha-glucosidase inhibitors but combines well with other strategies (vinegar before meals, exercise after meals, fiber-first meal sequencing). See our CGM page for the broader CGM-based optimization framework.
HbA1c, Fasting Glucose, and Long-Term Markers
The long-term diabetes-prevention markers respond to sustained OLE supplementation:
- HbA1c — meta-analyses of OLE trials in prediabetic and type 2 diabetic populations suggest an absolute HbA1c reduction of approximately 0.2-0.5% with 6+ months of OLE 1,000 mg/day. The effect is real but modest; for comparison, metformin produces approximately 1.0-1.5% HbA1c reduction.
- Fasting glucose — typical reductions of 5-12 mg/dL after 12-16 weeks in prediabetic populations
- HOMA-IR — 10-20% reductions consistently reported across trials
- Fasting insulin — small reductions reflecting improved sensitivity
The honest framing: OLE is not metformin, and patients with overt type 2 diabetes (HbA1c >6.5%) should not substitute OLE for guideline-indicated pharmacotherapy. For prediabetes and metabolic syndrome where pharmacotherapy is often deferred or not used, OLE provides a modest mechanistically-grounded metabolic benefit that combines with lifestyle change.
Stacking with Metformin and Lifestyle Intervention
OLE's mechanism overlaps with metformin in some respects (both activate AMPK; both improve insulin sensitivity) and complements it in others (OLE has a beta-cell secretagogue effect that metformin lacks; OLE provides additional cardiovascular and antioxidant benefits). For patients already on metformin who are seeking additional support:
- OLE 500 mg twice daily is a reasonable addition; no documented adverse drug interaction
- Monitor glucose more carefully in the first 2-4 weeks for any additive effect (rare to require metformin dose adjustment, but possible)
- The combination may produce additional cardiovascular benefit (BP reduction, lipid improvement) that metformin alone does not provide
For patients in the Diabetes Prevention Program or similar lifestyle intervention setting, OLE is a reasonable adjunct that may improve insulin sensitivity beyond what diet and exercise achieve alone. The Mediterranean dietary pattern itself, which delivers cumulative olive polyphenols through diet, has been shown to delay diabetes onset (PREDIMED-PLUS trial); OLE supplementation may add to that effect for patients who do not consume substantial olive oil.
The integrated strategy:
- Weight loss target (5-10% of body weight) through caloric reduction and physical activity
- Mediterranean dietary pattern with liberal extra-virgin olive oil
- Regular aerobic exercise (150 min/week moderate or 75 min/week vigorous)
- Resistance training 2-3× per week (preserves muscle mass and insulin sensitivity)
- OLE 500-1,000 mg/day standardized to 18% oleuropein
- Consideration of metformin if BMI >35 or other high-risk features and lifestyle alone is insufficient
- Continuous glucose monitor (if available) to provide direct feedback on glucose response to meals and lifestyle
Practical Dosing and Monitoring
- Standard prediabetes / metabolic syndrome dose: 500 mg twice daily of OLE standardized to 18-20% oleuropein
- Pre-meal dosing for postprandial glucose: 500 mg 30 minutes before largest carbohydrate meal of the day; can be in addition to background twice-daily dosing
- Monitoring schedule: baseline fasting glucose, insulin, HbA1c, and lipid panel before starting. Repeat at 3 months. If improving, continue and recheck at 6 and 12 months. If no measurable improvement at 6 months in good lifestyle context, OLE is unlikely to add value — consider alternative interventions.
- CGM integration: for patients using CGM, OLE's postprandial effect is directly observable. Use the data to guide meal-timing and dosing decisions.
- Time to effect: insulin sensitivity changes are measurable at 8-12 weeks; HbA1c changes lag and are not interpretable until 3 months minimum.
Cautions (Hypoglycemia, Drug Interactions)
- Hypoglycemia risk with insulin or sulfonylureas — patients on insulin (any type) or sulfonylureas (glipizide, glyburide, glimepiride) must monitor glucose more closely when adding OLE because the combined insulin-sensitizing and secretagogue effects can cause symptomatic hypoglycemia. Dose adjustment of insulin or sulfonylurea may be needed. Always consult the prescribing physician before adding OLE in this setting.
- DPP-4 inhibitors (sitagliptin, linagliptin) — theoretical additive effect on GLP-1, though documented interactions have not been reported. Use caution.
- GLP-1 receptor agonists (semaglutide, liraglutide, tirzepatide) — OLE's additional effects are minor relative to these drugs; no significant interaction expected.
- Metformin — well-tolerated combination; no documented interaction. Both activate AMPK; the combined effect on glucose is typically additive but rarely causes hypoglycemia because both have weak intrinsic hypoglycemic effects.
- Surgery and fasting — stop OLE 1-2 weeks before elective surgery or before extended fasting (more than 24 hours) to minimize hypoglycemia risk.
- Pregnancy and lactation — not studied in gestational diabetes management; avoid in pregnancy.
- Cardiovascular drug interactions — see the Cardiovascular deep-dive for OLE's effects on blood pressure and the additive risk with antihypertensives.
Key Research Papers
- Wainstein J et al. (2012). Olive leaf extract as a hypoglycemic agent in both human diabetic subjects and in rats. Journal of Medicinal Food 15(7):605-610. — PubMed
- de Bock M et al. (2013). Olive (Olea europaea L.) leaf polyphenols improve insulin sensitivity in middle-aged overweight men: a randomized, placebo-controlled, crossover trial. PLOS ONE. — PubMed
- Cumaoglu A et al. (2011). Effect of olive leaf extract on activities of enzymes of carbohydrate metabolism in pancreas of diabetic rats. Journal of Ethnopharmacology. — PubMed
- Al-Azzawie HF, Alhamdani MS (2006). Hypoglycemic and antioxidant effect of oleuropein in alloxan-diabetic rabbits. Life Sciences. — PubMed
- Jemai H et al. (2009). Lipid-lowering and antioxidant effects of hydroxytyrosol and its triacetylated derivative recovered from olive tree leaves in cholesterol-fed rats. Journal of Agricultural and Food Chemistry. — PubMed
- Kim Y et al. (2014). Effects of olive leaf extract on insulin sensitivity in middle-aged overweight men. European Journal of Nutrition. — PubMed
- Hadrich F et al. (2016). Synergistic hypocholesterolemic effect of oleuropein and hydroxytyrosol on liver enzymes. Lipids in Health and Disease. — PubMed
- Sangi SMA et al. (2015). Antihyperglycemic effect of thymoquinone and oleuropein in streptozotocin-induced diabetic rats. Saudi Pharmaceutical Journal. — PubMed
- Salazar García M et al. (2018). Beneficial effects of olive leaf extract on insulin resistance in HepG2 cells. Journal of Functional Foods. — PubMed
- Hassen I et al. (2015). Biological activities of olive leaf extract: a review. Journal of Functional Foods. — PubMed
- Martín-Peláez S et al. (2017). Olive oil polyphenols and gut microbiota. Molecular Nutrition and Food Research. — PubMed
- Salas-Salvadó J et al. (2014). Prevention of diabetes with Mediterranean diets: a subgroup analysis of a randomized trial (PREDIMED). Annals of Internal Medicine. — PubMed
PubMed Topic Searches
- PubMed: OLE and insulin sensitivity
- PubMed: Oleuropein and beta-cell function
- PubMed: Hydroxytyrosol and AMPK
- PubMed: Olive polyphenols and GLP-1
- PubMed: Mediterranean diet and diabetes prevention
Connections
- Olive Leaf Benefits Hub
- Olive Leaf Overview
- OLE Cardiovascular
- OLE Antimicrobial
- OLE Antioxidant
- Type 2 Diabetes
- Coffee for Type 2 Diabetes
- Continuous Glucose Monitor
- Olive Oil
- Cinnamon
- Berberine
- Magnesium
- Chromium
- Endocrinology
- All Herbs
- Metformin — the first-line pharmaceutical this extract is compared against and stacked with.