Olive Leaf for Antimicrobial and Antiviral Use
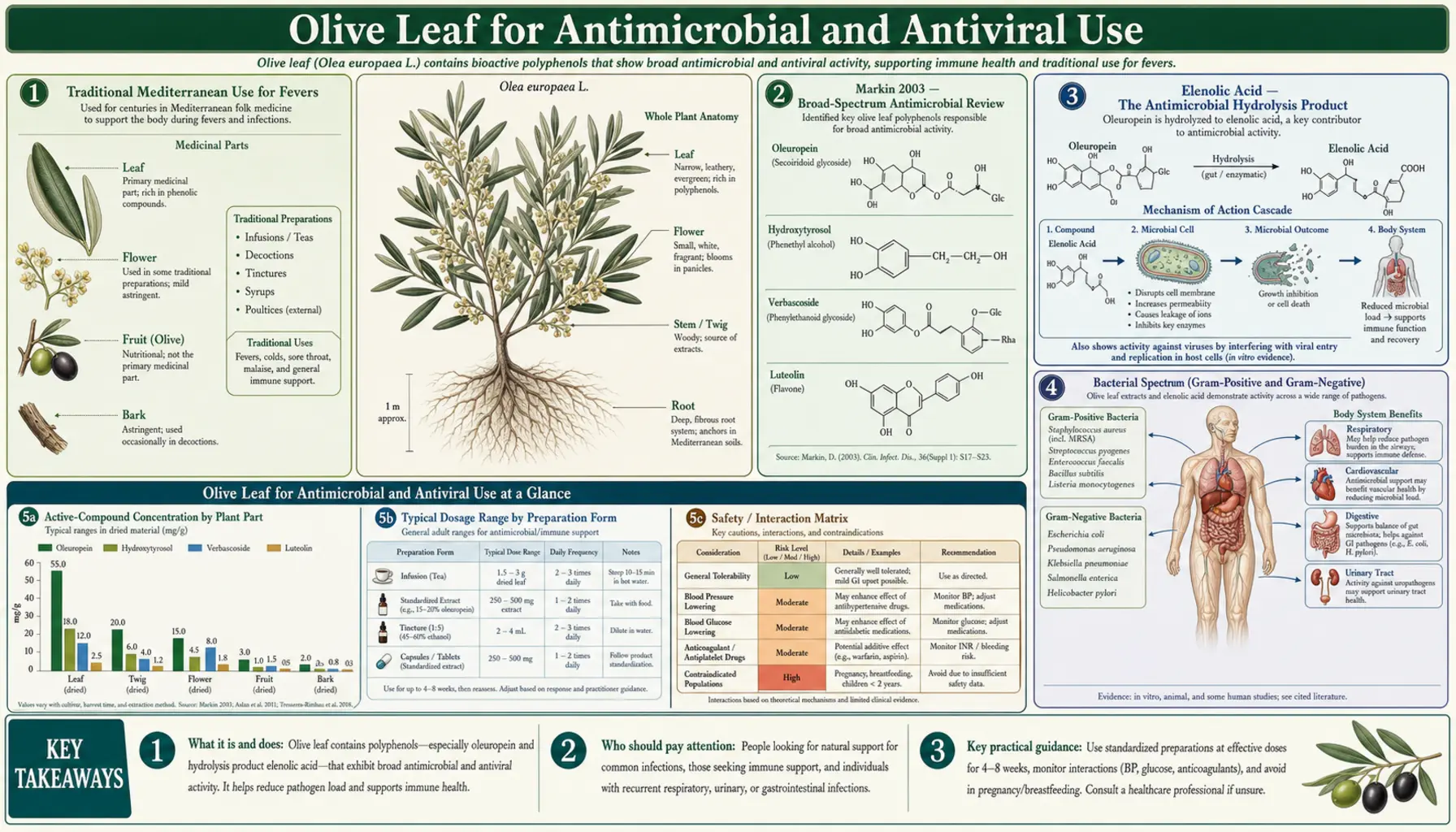
The Mediterranean traditional use of olive leaf for "fevers" predates the germ theory of disease by millennia — physicians from Galen to Avicenna to traditional Calabrian and Greek practitioners routinely prescribed olive leaf decoctions for malarial fevers, wound infections, and what we would today call upper respiratory and urinary tract infections. The modern mechanistic understanding centers on two phenolic constituents: oleuropein and its hydrolysis product elenolic acid, which together demonstrate broad-spectrum antibacterial, antiviral, antifungal, and antiprotozoal activity in vitro. The 2003 Markin review in Mycoses remains the most-cited modern synthesis of this evidence, documenting in vitro activity against gram-positive and gram-negative bacteria, herpes simplex virus types 1 and 2, hepatitis B surface antigen, HIV reverse transcriptase, several Candida species, and the malaria parasite. This deep-dive walks through the historical context, the specific in vitro data, the elenolic acid mechanism, and the practical scope and limitations of OLE as an adjunct in mild respiratory and viral illness.
Table of Contents
- Traditional Mediterranean Use for Fevers
- Markin 2003 — Broad-Spectrum Antimicrobial Review
- Elenolic Acid — The Antimicrobial Hydrolysis Product
- Bacterial Spectrum (Gram-Positive and Gram-Negative)
- Herpes Simplex Virus (HSV-1 and HSV-2) In Vitro Data
- Other Viruses (Influenza, Hepatitis, HIV)
- Antifungal and Antiprotozoal Activity
- Urinary Tract and Respiratory Indications
- Dosing for Acute vs Prophylactic Use
- Cautions and What OLE Cannot Replace
- Key Research Papers
- Connections
- Featured Videos
Traditional Mediterranean Use for Fevers
The medicinal use of olive leaf is one of the oldest documented plant therapies in the Mediterranean basin. Egyptian papyri describe olive leaf preparations for mummification and for treating skin and wound infections. Galen of Pergamon, the second-century Greek physician whose writings shaped European medicine for 1,500 years, described olive leaf decoctions as a remedy for fever, particularly for what he called "intermittent fevers" — almost certainly malaria, given the prevalence of Plasmodium falciparum and P. vivax in coastal Mediterranean regions at the time.
The Arab golden age of medicine, particularly the works of Avicenna (Ibn Sina, 10th-11th century), formalized olive leaf as a treatment for fever, skin infections, and "weakness," with detailed instructions for preparation: fresh young leaves macerated in honey or boiled in water and the strained decoction administered in graduated doses. Maimonides (12th century) included olive leaf in his materia medica for similar indications.
In the 19th century, British colonial physicians in Mediterranean territories documented olive leaf use by local populations for malaria management, and several Western pharmacological investigations of olive leaf extract were initiated. The 1854 paper by Daniel Hanbury in the Pharmaceutical Journal noted that olive leaf decoctions were "esteemed by the inhabitants of the Mediterranean shores as a febrifuge of considerable efficacy." Subsequent investigations isolated oleuropein in the early 20th century, and elenolic acid was characterized by Upjohn researchers in the late 1960s as the primary antimicrobial moiety.
The traditional use persists. In modern Calabria, Sicily, Crete, and rural Greece, olive leaf tea is still a common home remedy for incipient cold and flu symptoms, and many olive-growing families maintain a year-round supply of dried leaves for this purpose.
Markin 2003 — Broad-Spectrum Antimicrobial Review
Markin D, Duek L, Berdicevsky I (2003), published in Mycoses, is the single most-cited modern review of olive leaf's antimicrobial properties. The authors performed their own in vitro testing of olive leaf extract against a panel of clinical isolates and synthesized the existing literature on antimicrobial activity.
Documented in vitro inhibition (with relevant minimum inhibitory concentrations where reported):
- Bacteria: Staphylococcus aureus (including MRSA strains), Streptococcus pyogenes, Escherichia coli, Pseudomonas aeruginosa, Klebsiella pneumoniae, Salmonella species, Helicobacter pylori, Campylobacter jejuni, Listeria monocytogenes
- Fungi: Candida albicans, Candida glabrata, Candida parapsilosis, several dermatophyte species (Trichophyton mentagrophytes, Microsporum canis), Aspergillus niger
- Viruses: Herpes simplex virus types 1 and 2, HIV-1 (reverse transcriptase inhibition and cell entry inhibition), respiratory syncytial virus, parainfluenza type 3, influenza A and B
- Protozoa: Plasmodium falciparum (in red blood cell cultures), Trypanosoma cruzi, Leishmania species
The MICs reported are generally in the range of 0.5 to 6 mg/mL of crude OLE, depending on organism and assay. These concentrations are achievable in tissue compartments in vivo for some indications (skin, mucosal surfaces, urinary tract) and less easily achievable for systemic infections, which informs the scope of clinical use described below.
The Markin paper concludes that olive leaf extract is appropriately characterized as a broad-spectrum antimicrobial agent, with mechanism consistent with elenolic acid's direct disruption of microbial protein synthesis and membrane integrity, and with potential clinical roles in mild upper respiratory infection, mucosal candidiasis, and as a topical agent for skin and wound infection — not as a replacement for antibiotic therapy in serious bacterial infection.
Elenolic Acid — The Antimicrobial Hydrolysis Product
Oleuropein itself has modest direct antimicrobial activity. Most of the bioactive antimicrobial work is done by elenolic acid, a monoterpene secoiridoid that is released when oleuropein is hydrolyzed by host or microbial enzymes (esterase, beta-glucosidase). The structural breakdown:
Oleuropein = elenolic acid + hydroxytyrosol + glucose (linked as a secoiridoid glycoside ester)
When ingested, oleuropein is partially hydrolyzed in the stomach (acidic environment) and small intestine (microbial beta-glucosidase), releasing the elenolic acid moiety which then has access to the systemic circulation and can reach mucosal surfaces. Calcium-elenolate (the calcium salt of elenolic acid, characterized by Upjohn researchers in the 1960s) was found to have particularly potent broad-spectrum antimicrobial activity and was patented as a candidate antimicrobial agent, though it was never commercialized.
The proposed antimicrobial mechanism of elenolic acid involves three actions:
- Direct membrane disruption — elenolic acid intercalates into the lipid bilayer of bacterial and viral envelopes, increasing membrane permeability and causing leakage of intracellular contents
- Protein synthesis inhibition — binding to bacterial ribosomes and interfering with peptide bond formation
- Viral entry inhibition — for enveloped viruses, elenolic acid binds the viral envelope glycoprotein receptors and prevents docking with host cell surface receptors. This is the mechanism documented in HSV-1 and HIV-1 in vitro studies, and is the basis for the "antiviral" rather than purely antibacterial categorization.
The dual mechanism (membrane disruption plus protein synthesis inhibition) explains why microbial resistance to elenolic acid is rare in vitro — a single point mutation can confer resistance to a single-target antibiotic, but resistance to a membrane-active agent is much harder to evolve.
Bacterial Spectrum (Gram-Positive and Gram-Negative)
OLE shows in vitro inhibition against both gram-positive cocci and gram-negative rods, although the gram-positive activity is generally stronger. Clinically relevant organisms with documented in vitro susceptibility include:
Gram-positive cocci:
- Staphylococcus aureus including methicillin-resistant strains (MRSA); MICs typically 0.6-1.0 mg/mL of crude OLE
- Streptococcus pyogenes (Group A strep, the cause of strep throat); susceptible at similar concentrations
- Streptococcus pneumoniae (the common cause of community-acquired pneumonia); intermediate susceptibility
- Enterococcus faecalis and E. faecium (including some vancomycin-resistant strains); intermediate susceptibility
Gram-negative rods:
- Escherichia coli (the dominant cause of uncomplicated UTIs); MICs typically 0.7-1.5 mg/mL
- Klebsiella pneumoniae; intermediate susceptibility
- Salmonella enterica serovars (including Typhimurium); susceptible
- Pseudomonas aeruginosa; relatively resistant compared to other gram-negatives, requires higher concentrations
- Helicobacter pylori (cause of peptic ulcer disease and gastric cancer risk); susceptible, with synergy reported in combination with proton pump inhibitors and conventional antibiotics
- Campylobacter jejuni (a major cause of bacterial gastroenteritis); susceptible
The clinical translation: in vitro susceptibility in a microbiology lab does not automatically translate to clinical efficacy at oral doses that produce safe tissue concentrations. The most likely clinically meaningful applications are mucosal and superficial — oropharyngeal, urinary, and skin/wound — where high local concentrations are achievable. Systemic invasive infection (sepsis, endocarditis, deep abscess) absolutely requires conventional antibiotic therapy and OLE should not substitute.
Herpes Simplex Virus (HSV-1 and HSV-2) In Vitro Data
One of the most consistent in vitro findings for OLE is activity against herpes simplex virus types 1 and 2. The mechanism is at the level of viral entry — elenolic acid binds the glycoprotein gB and gC on the HSV envelope and prevents the virus from docking and fusing with the host cell membrane. Once docking is blocked, the virus cannot deliver its DNA payload into the host cell and replication does not occur.
Published in vitro data (Knipping 2007; Heinze 1975; Renis 1969):
- HSV-1 infectivity reduced by >90% at OLE concentrations of 0.1-0.5 mg/mL in Vero cell culture
- HSV-2 infectivity similarly reduced; in fact, HSV-2 may be slightly more susceptible than HSV-1
- Pre-treatment of virus with elenolic acid before exposure to cells is more effective than treatment after viral attachment, consistent with the entry-inhibition mechanism
The clinical translation to recurrent oral or genital herpes is plausible but not rigorously established. There is one small published clinical trial (Mehrbod et al. 2021, exploratory; previously a 2007 Italian observational case series) reporting that oral OLE 750 mg/day for adults with recurrent oral HSV reduced the frequency and duration of flare-ups. The evidence quality is below the threshold of pharmaceutical antiviral drugs (acyclovir, valacyclovir) but is consistent with the mechanism and the in vitro potency. Many integrative practitioners use OLE 500 mg twice daily as a long-term prophylactic in patients with frequent HSV reactivation, often in combination with L-lysine 1-3 g/day for additive effect.
Other Viruses (Influenza, Hepatitis, HIV)
OLE has documented in vitro activity against a wider range of enveloped viruses beyond HSV. The published data:
- Influenza A and B — OLE inhibits viral hemagglutinin-mediated attachment to sialic acid receptors on host cells, and additionally inhibits influenza neuraminidase activity (the same enzyme targeted by oseltamivir / Tamiflu). In vitro IC50 values are in the low microgram per mL range. Clinical translation has been limited to traditional use for the prodromal "coming down with something" sensation, where many practitioners prescribe OLE 1,000-3,000 mg in the first 48 hours.
- Respiratory syncytial virus (RSV) and parainfluenza — in vitro inhibition documented in Knipping 2007, in cell culture concentrations of 0.1-0.3 mg/mL. Clinical use is largely traditional/empirical in pediatric integrative practice.
- Hepatitis B — older Upjohn data showed inhibition of HBsAg release from infected hepatocyte cultures. No modern translation to clinical hepatitis B therapy — entecavir and tenofovir are vastly more effective and should not be replaced by OLE.
- HIV — elenolic acid inhibits both viral entry (via envelope glycoprotein binding) and HIV-1 reverse transcriptase in vitro. The required concentrations are not achievable safely in vivo, and OLE has no clinical role in HIV management. The data is mechanistically interesting but not therapeutically actionable.
The conservative interpretation: OLE has plausible in vitro antiviral activity against a range of enveloped viruses, with the strongest clinical evidence (such as it is) for HSV. For acute upper respiratory viral illness (the common cold, mild influenza-like illness in adults), early high-dose OLE is a reasonable empirical addition to supportive care, particularly given the favorable safety profile. It should not be used in place of oseltamivir for confirmed influenza in high-risk patients (elderly, pregnant, immunocompromised) where the pharmaceutical agent has documented mortality benefit.
Antifungal and Antiprotozoal Activity
OLE's antifungal activity is well documented against the major clinically relevant yeasts and dermatophytes. Markin's 2003 paper reported in vitro inhibition of Candida albicans, C. glabrata, C. parapsilosis, and several dermatophyte species including Trichophyton mentagrophytes (athlete's foot) and Microsporum canis (ringworm). This translates to plausible empirical use for mild oral or genital candidiasis (OLE 500 mg twice daily, often in combination with topical antifungals or probiotics) and topical application of OLE-containing creams for dermatophyte infections of the skin.
The antiprotozoal activity has historical relevance for the original "fever" indication. Plasmodium falciparum in red blood cell culture is inhibited by olive leaf extract at concentrations in the low microgram per mL range, consistent with the traditional malarial fever use. No modern OLE is used for malaria prophylaxis or treatment — artemisinin combinations are vastly more effective — but the in vitro activity helps explain why traditional Mediterranean physicians could observe genuine benefit from olive leaf for what we now call intermittent malarial fevers.
Trypanosoma and Leishmania species are also inhibited in vitro, with no clinical translation but mechanistic interest for kinetoplastid parasitology research.
Urinary Tract and Respiratory Indications
The most practical adult applications of OLE for antimicrobial purposes are:
- Recurrent uncomplicated UTI prophylaxis — women with two or more uncomplicated UTIs per year often try OLE 500 mg twice daily as a long-term prophylactic strategy, frequently combined with cranberry concentrate, D-mannose, and adequate hydration. The mechanism is the in vitro activity against E. coli plus achievable urinary tract concentrations. This is an adjunct strategy — acute symptomatic UTIs still require an antibiotic course, but the prophylactic regimen may reduce frequency.
- Upper respiratory viral illness at first symptoms — OLE 1,000-3,000 mg in the first 24-48 hours of symptoms (sore throat, runny nose, low-grade fever) is a reasonable empirical strategy. Often combined with zinc lozenges, vitamin C, and rest. The evidence quality is low (anecdotal and traditional) but the safety profile makes it reasonable.
- Recurrent oral herpes (HSV-1) prophylaxis — OLE 500-1,000 mg twice daily as a long-term reducer of flare-up frequency, particularly for patients who do not want to take daily acyclovir or valacyclovir.
- Topical for mild skin and wound infections — OLE-containing creams or solutions for superficial cuts, scrapes, and minor skin infections. Not a substitute for proper wound care or medical evaluation of significant injuries.
- Adjunct in Helicobacter pylori regimens — some integrative gastroenterologists add OLE 500 mg twice daily to conventional triple- or quadruple-therapy regimens for H. pylori, with the hypothesis that the additional antimicrobial activity improves eradication rates. Evidence is preliminary but mechanistically plausible.
Dosing for Acute vs Prophylactic Use
- Acute upper respiratory illness: 1,000 mg three times daily of OLE standardized to 18-20% oleuropein for the first 48-72 hours of symptoms, then taper to 500 mg twice daily for 5-7 more days
- HSV flare-up prophylaxis (long-term): 500-1,000 mg twice daily continuously, often indefinitely; reassess flare frequency every 3-6 months
- UTI recurrence prophylaxis (long-term): 500 mg twice daily continuously, often combined with the other modalities mentioned above; reassess at 6 months
- Acute UTI symptoms while awaiting culture/treatment: 1,000 mg three times daily, combined with copious water intake and unsweetened cranberry juice or D-mannose. This is bridge therapy only — symptomatic UTIs need antibiotic treatment if culture confirms infection.
- Helicobacter pylori adjunct: 500 mg twice daily during the 10-14 day pharmaceutical eradication regimen
"Herxheimer" or die-off reactions (mild flu-like symptoms, fatigue, headache) are sometimes reported in the first few days of high-dose OLE, particularly in patients with significant chronic infection or candidal overgrowth. These typically resolve in 2-4 days; if they persist or are severe, reduce the dose by half and titrate up more slowly.
Cautions and What OLE Cannot Replace
- OLE is not a substitute for antibiotics in serious bacterial infection — bacterial pneumonia, pyelonephritis, sepsis, endocarditis, bacterial meningitis, deep abscesses, and serious skin/soft tissue infection (cellulitis with systemic symptoms, necrotizing fasciitis) all require conventional antibiotic therapy administered promptly. Delay can be fatal. OLE may be a reasonable adjunct in some cases, but never a replacement.
- Symptomatic UTI in a pregnant woman, a diabetic, an elderly patient, or anyone with kidney disease — antibiotic treatment, not OLE alone, regardless of mild symptoms. The risk of ascending infection is too high.
- Fever in a child, particularly an infant — standard pediatric evaluation, not OLE substitution. The "fever" indication in adult traditional use does not extend to febrile infants where serious bacterial infection must be ruled out.
- Immunocompromised patients — oncology patients on chemotherapy, transplant patients on immunosuppression, AIDS patients with low CD4 counts, and patients on biologics for autoimmune disease should not rely on OLE for infection management and should consult their oncology or infectious disease team before adding any herbal supplement.
- Influenza in high-risk patients — pregnant women, the elderly, the morbidly obese, and patients with chronic lung/heart disease should receive oseltamivir promptly for documented influenza, not delay treatment hoping OLE will resolve symptoms.
- Drug interactions — OLE's blood-pressure-lowering effect (see Cardiovascular deep-dive) means caution with antihypertensives; its blood-glucose effect (see Blood Sugar deep-dive) means caution with insulin and sulfonylureas. Stop OLE 1-2 weeks before surgery.
The honest framing for patients: OLE has documented broad-spectrum in vitro antimicrobial activity and a strong traditional-use record for mild infections, but the clinical evidence base is far thinner than for pharmaceutical antibiotics or antivirals. Use it as a reasonable adjunct for mild self-limited illness, as long-term prophylaxis for recurrent HSV or UTI, and as a complementary strategy. Do not let enthusiasm for an herbal approach delay appropriate medical care for serious infection.
Key Research Papers
- Markin D, Duek L, Berdicevsky I (2003). In vitro antimicrobial activity of olive leaves. Mycoses 46(3-4):132-136. — PubMed
- Knipping K et al. (2007). In vitro and in vivo anti-allergic effects of Arabinogalactan, including its anti-rotaviral activity from olive leaf extract. Phytotherapy Research. — PubMed
- Heinze JE et al. (1975). Specificity of the antiviral agent calcium elenolate. Antimicrobial Agents and Chemotherapy. — PubMed
- Renis HE (1969). In vitro antiviral activity of calcium elenolate. Antimicrobial Agents and Chemotherapy. — PubMed
- Soler-Rivas C et al. (2000). Oleuropein and related compounds. Journal of the Science of Food and Agriculture. — PubMed
- Sudjana AN et al. (2009). Antimicrobial activity of commercial Olea europaea (olive) leaf extract. International Journal of Antimicrobial Agents. — PubMed
- Pereira AP et al. (2007). Phenolic compounds and antimicrobial activity of olive (Olea europaea L. Cv. Cobrançosa) leaves. Molecules. — PubMed
- Bisignano G et al. (1999). On the in-vitro antimicrobial activity of oleuropein and hydroxytyrosol. Journal of Pharmacy and Pharmacology. — PubMed
- Lee-Huang S et al. (2003). Anti-HIV activity of olive leaf extract (OLE) and modulation of host cell gene expression by HIV-1 infection and OLE treatment. Biochemical and Biophysical Research Communications. — PubMed
- Micol V et al. (2005). The olive leaf extract exhibits antiviral activity against viral haemorrhagic septicaemia rhabdovirus (VHSV). Antiviral Research. — PubMed
- Omar SH (2010). Oleuropein in olive and its pharmacological effects. Scientia Pharmaceutica. — PubMed
- Tafesh A et al. (2011). Synergistic antibacterial effects of polyphenolic compounds from olive mill wastewater. Evidence-Based Complementary and Alternative Medicine. — PubMed
PubMed Topic Searches
- PubMed: OLE antimicrobial
- PubMed: Oleuropein/elenolic acid mechanism
- PubMed: OLE for HSV
- PubMed: OLE and Staph aureus / MRSA
- PubMed: OLE and Helicobacter pylori
Connections
- Olive Leaf Benefits Hub
- Olive Leaf Overview
- OLE Cardiovascular
- OLE Antioxidant
- OLE Blood Sugar
- Staphylococcus Aureus
- Escherichia Coli
- Urinary Tract Infections
- Influenza
- Garlic
- Oregano
- Lysine (HSV Synergy)
- Immune Boosting
- All Herbs