Chanca Piedra for Hepatitis B: Niranthin Polymerase Inhibition, Clinical Trial Evidence, and Combination with Entecavir/Tenofovir
The companion Liver Protection page covers general hepatoprotection — the 1988 Thyagarajan Lancet headline, NAFLD signals, anti-tuberculosis hepatoprotection, drug interaction warnings. This page goes deeper on the one indication that drove Chanca Piedra into mainstream phytotherapy journals in the first place: chronic hepatitis B infection. We focus on the virology, the specific lignan that does the antiviral heavy lifting (niranthin), the surrogate-endpoint data from Phase II-style trials (HBsAg, HBeAg, HBV-DNA), how the herb's mechanism compares to nucleoside analogs like entecavir and tenofovir, and the honest answer to the question every HBV carrier eventually asks: "can I take this with my antiviral?"
Table of Contents
- HBV Virology in 60 Seconds: Why HBsAg Loss Matters
- Niranthin and the Reverse-Transcriptase Target
- Niranthin vs Nucleoside Analogs (Entecavir, Tenofovir, Lamivudine)
- HBsAg, HBeAg, and HBV-DNA Trial Data
- Dosing Used in the Trials
- HCV and Other Chronic Hepatitides
- Alongside-Conventional-Therapy Strategy
- Monitoring Labs and What to Watch
- Limitations of the Evidence Base
- Who Should — and Should Not — Try This
- Key Research Papers
- Connections
- Featured Videos
HBV Virology in 60 Seconds: Why HBsAg Loss Matters
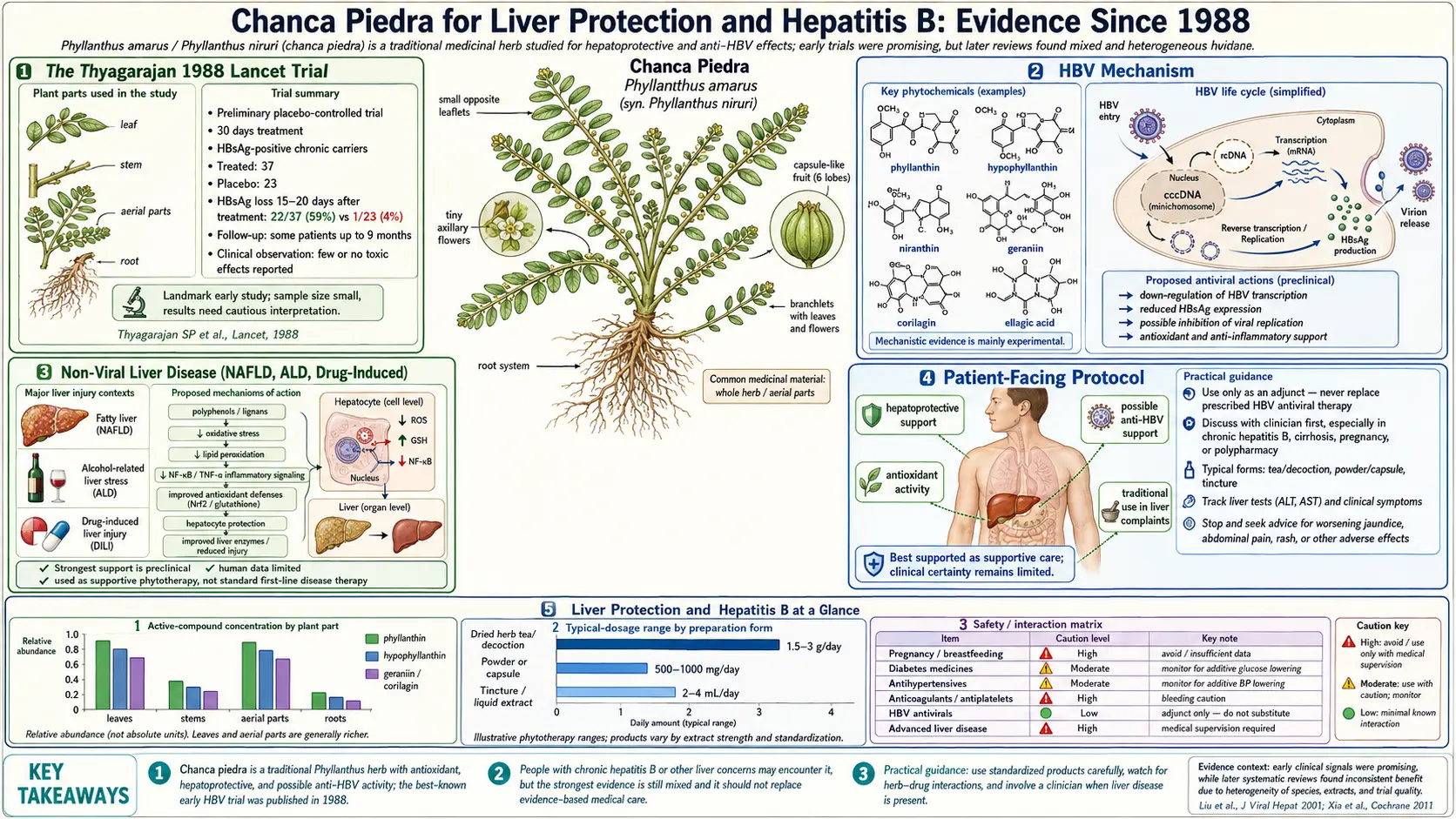
Chronic hepatitis B virus (HBV) is a partially double-stranded DNA virus with a quirky replication cycle. After infecting a hepatocyte, the relaxed circular DNA (rcDNA) is converted in the nucleus into a stable, episomal covalently closed circular DNA (cccDNA) — the viral "minichromosome." cccDNA is the durable reservoir that makes HBV a lifelong infection in most adults who acquire it.
From cccDNA, the virus transcribes a 3.5-kb pregenomic RNA (pgRNA), which is packaged into nucleocapsids along with the viral polymerase. The polymerase is a multifunctional enzyme: it acts as an RNA-dependent DNA polymerase (a reverse transcriptase) to copy pgRNA back into the partially double-stranded DNA genome, plus it has DNA-dependent DNA polymerase and RNase H activity. This reverse-transcriptase step is the Achilles' heel that all approved oral HBV drugs target.
Serologic markers carry the clinical meaning:
- HBV-DNA — quantitative PCR; reflects ongoing replication; modern antivirals routinely drive this below the limit of detection (LoD).
- HBeAg — e antigen; secreted protein from the precore region; presence correlates with high replication and infectivity. HBeAg seroconversion (loss of HBeAg + appearance of anti-HBe) is a meaningful clinical milestone.
- HBsAg — surface antigen; reflects ongoing viral protein production from cccDNA or from integrated HBV DNA in the host genome. HBsAg loss ("functional cure") is the holy grail — achieved in <1% per year of nucleoside-analog therapy and only marginally better with pegylated interferon.
- Anti-HBs — protective antibody; ideally follows HBsAg loss, locking in seroconversion.
This is why the original Thyagarajan paper made such a splash. It reported a 30-day intervention producing HBsAg loss in 22 of 37 patients (59%). Modern entecavir and tenofovir, given for years, do not approach that. The Thyagarajan magnitude has never been independently reproduced — later trials show meaningful but much smaller signals (typically <10% HBsAg loss). The biological plausibility of even the modest signal is what keeps the research going.
Niranthin and the Reverse-Transcriptase Target
Of the four major aryltetralin lignans in P. amarus (phyllanthin, hypophyllanthin, niranthin, nirtetralin), niranthin is the standout antiviral. Mechanistic work over the past two decades has converged on several specific actions:
- HBV polymerase / reverse-transcriptase inhibition — niranthin (and nirtetralin) binds the catalytic pocket of HBV polymerase and reduces RNA-templated DNA synthesis in cell-free enzyme assays and in stably-transfected HepG2.2.15 cells. The IC50s in cell culture sit in the low-micromolar range — substantially weaker than entecavir on a per-molar basis, but biologically meaningful given the achievable plasma concentrations.
- HBeAg secretion suppression — niranthin reduces HBeAg secretion from HepG2.2.15 by roughly 50% at non-cytotoxic doses, with HBsAg suppression a less pronounced second-order effect.
- cccDNA-independent activity — the inhibition is downstream of the cccDNA pool. Niranthin does not appear to deplete cccDNA itself (no current antiviral does), which is why even effective suppression doesn't equal cure.
- Synergy with the ellagitannins — geraniin and corilagin contribute independent polymerase-binding activity in cell-free assays, and the urolithin metabolites produced by gut microbiota from geraniin add anti-inflammatory cover during long courses. Whole-herb extracts outperform isolated niranthin in most head-to-head assays for this reason.
- Immunomodulation — in animal models, Phyllanthus extracts shift Th1/Th2 cytokine balance toward Th1, boost NK cell activity, and modestly upregulate type I interferon signaling. Whether these effects translate to humans is uncertain, but they're the second plausible mechanism by which Phyllanthus could push HBeAg seroconversion rates.
For the broader lignan/tannin profile see the Active Compounds page.
Niranthin vs Nucleoside Analogs (Entecavir, Tenofovir, Lamivudine)
It's worth being precise about how niranthin's mechanism differs from the approved drugs:
- Nucleoside / nucleotide analogs (NAs) — entecavir (a deoxyguanosine analog), tenofovir disoproxil fumarate (TDF) and tenofovir alafenamide (TAF) (deoxyadenosine analogs), lamivudine and emtricitabine (cytidine analogs). These are chain terminators: phosphorylated to the active triphosphate, they get incorporated into the growing HBV DNA strand by the polymerase, then halt further nucleotide addition because they lack the 3'-OH group needed for the next bond.
- Niranthin — a non-nucleoside polymerase inhibitor. It binds the enzyme allosterically (not at the nucleotide-binding site), more analogous in concept to the NNRTIs used in HIV. There is no need for intracellular phosphorylation, no chain termination, and no cross-resistance with NA mutations (rtM204V/I, rtL180M, etc.).
The clinical implication: niranthin theoretically retains activity against NA-resistant HBV strains. There are no controlled trials specifically testing this, but the mechanistic non-overlap is the basis for the combination logic discussed below.
The other side of the comparison — potency — is starkly in favor of the drugs. Entecavir has a cell-culture EC50 around 4 nM. Niranthin's EC50 in equivalent assays is roughly 5,000-10,000 times higher. Niranthin is not going to replace entecavir for any patient who needs viral suppression. It might still contribute, which is the whole reason for the adjunctive-use literature.
HBsAg, HBeAg, and HBV-DNA Trial Data
The clinical literature on Phyllanthus in HBV is uneven but not empty. The most-cited findings:
- Thyagarajan 1988 (Lancet) — 200 mg P. amarus powder TID × 30 days, open-label, 37 carriers. HBsAg loss: 22/37 (59%) at 1-3 months vs 1/23 placebo. The number that started everything.
- Doshi 1994 (Indian Journal of Medical Research) — replication attempt in Bombay carriers. Lower HBsAg-loss rates (closer to 10-15%) but documented HBeAg seroconversion and ALT/AST improvement.
- Wang 1995 (Journal of Laboratory and Clinical Medicine) — Chinese chronic hepatitis B cohort treated with P. amarus. HBeAg loss ≈ 22% vs <5% control over 30-day intervention.
- Berk 1991 (The Lancet) — one of the first negative replication attempts. North American HBV carriers, no HBsAg loss difference vs placebo. Highlighted the regional/species/preparation heterogeneity problem.
- Xia 2011 Cochrane review — 16 RCTs, 1,326 patients. Phyllanthus better than placebo on HBV-DNA clearance (RR ≈ 5.6), HBeAg loss (RR ≈ 3.4), and ALT normalization. But low study quality and species/preparation heterogeneity capped the strength of recommendation.
- Liu 2003 (Journal of Viral Hepatitis) — earlier systematic review covering 22 RCTs of various Phyllanthus species; pre-Cochrane methodology but reached similar conclusions on direction-of-effect with similar caveats on quality.
The pattern across the literature: ALT/AST does normalize in most patients. HBV-DNA does drop in a meaningful minority (typically 1-2 log10 reduction). HBeAg seroconversion is modestly improved (10-30% vs spontaneous rates of 5-15%). HBsAg loss is the headline endpoint that rarely reproduces at Thyagarajan magnitudes — usually 3-8% in modern trials, compared to ~1% per year on entecavir/tenofovir. A modest but real signal.
Dosing Used in the Trials
Dosing varies widely across the literature, which is one reason the meta-analyses are shaky. Representative protocols:
- Thyagarajan 1988 — 200 mg dried P. amarus powder, three times daily (600 mg/day total) × 30 days. Surfactant-resistant tannin preparation.
- Doshi 1994 — 250 mg standardized P. amarus dry extract TID × 30 days (750 mg/day).
- Wang 1995 — 200 mg P. amarus tablets, three times daily × 30 days.
- Various Indian trials — 500-1000 mg/day standardized extract, typically for 3-6 months. The longer durations seem to produce more HBeAg seroconversions.
- "Long-cure" Amazonian tea — 1 tablespoon of dried herb simmered in 1 liter water, sipped over the day, for 2-4 weeks. Lower extractive efficiency than alcoholic extracts, but the traditional dosing pattern.
For the integrative practitioner, a reasonable starting protocol mirrors the trial literature: 500 mg of a P. amarus extract standardized to phyllanthin/hypophyllanthin (often 5% total lignans) twice daily, taken with food, for 3 months as a first course. Reassess HBV-DNA and ALT at 3 months. See Forms, Dosing & Standardization for the broader dosing matrix.
HCV and Other Chronic Hepatitides
The hepatitis C virus (HCV) evidence base for Phyllanthus is much thinner than the HBV record, and modern direct-acting antivirals (DAAs — sofosbuvir, glecaprevir, velpatasvir, etc.) cure HCV in >95% of patients in 8-12 weeks. There is no clinical scenario in 2026 in which Phyllanthus is a reasonable alternative to DAA therapy for HCV.
What the cell-culture and small-study literature suggests:
- HCV NS3/4A protease inhibition — corilagin and geraniin show weak in-vitro inhibition; biologically interesting, clinically irrelevant given DAA availability.
- Adjunctive ALT support — in patients with persistent ALT elevation after DAA cure (so-called "post-SVR" liver disease, often driven by NAFLD or alcohol), Phyllanthus may contribute to ALT normalization as part of a broader hepatoprotective stack.
- Hepatitis D virus (HDV) — no meaningful evidence. HDV is a satellite virus dependent on HBV; the only approved drug is bulevirtide. Phyllanthus has not been studied here.
- Hepatitis E (HEV) — no clinical evidence; some weak in-vitro signals from related ellagitannins, not enough to act on.
Bottom line: for HCV today, you get the cure with DAAs. The Phyllanthus role is post-cure hepatoprotection, not antiviral. For HBV (where there is no cure, only suppression), the adjunctive antiviral case is more interesting.
Alongside-Conventional-Therapy Strategy
For a chronic HBV patient already on entecavir or tenofovir, what is the case for adding Chanca Piedra? The honest answer:
- Plausible — non-overlapping mechanism (allosteric vs chain-termination), potential synergy on HBV-DNA suppression, plausible additional pressure on HBeAg seroconversion, real antioxidant cover for hepatocytes.
- Not proven — no large head-to-head trial of NA monotherapy vs NA + Phyllanthus in HBV has been done at modern methodologic standards. The Cochrane review's "combination looks more promising than monotherapy" line is the best summary the literature supports.
- Drug-interaction caveats matter — entecavir and tenofovir are not CYP3A4 substrates (they're renally cleared), so the major Chanca Piedra CYP3A4 inhibition concern doesn't apply to the NA itself. But many HBV patients are on co-medications (statins, antihypertensives, immunosuppressants for transplant recipients) that are CYP3A4 substrates. The drug-interaction risk lives there.
- Never substitute — the single most important clinical principle: Chanca Piedra is never a replacement for entecavir or tenofovir. NA cessation in chronic HBV can produce severe ALT flares and acute liver failure. Patients who stop their antiviral to "try the herbal" are taking a real, occasionally lethal risk.
- Pegylated interferon combinations — the older literature with interferon-alpha + Phyllanthus combinations showed encouraging signals, but pegylated interferon use has declined as NAs improved. This regimen is now mostly reserved for younger HBeAg-positive patients with high ALT and low HBV-DNA who want a finite-duration treatment course.
Monitoring Labs and What to Watch
Anyone taking Chanca Piedra for HBV should already be in routine HBV monitoring. The herb doesn't change what gets checked — it changes what you watch for change in.
Baseline (before starting):
- HBV-DNA quantitative PCR
- HBsAg, anti-HBs (quantitative if available; the qHBsAg is increasingly used as a treatment-response marker)
- HBeAg, anti-HBe
- ALT, AST, GGT, alkaline phosphatase, total/direct bilirubin, albumin, INR, platelets (the basic synthetic-function panel)
- Alpha-fetoprotein (HCC surveillance baseline)
- Liver elastography (FibroScan) or APRI/FIB-4 calculated from baseline labs
- Renal function (creatinine, eGFR) — especially if on tenofovir, given TDF nephrotoxicity risk
3-month and 6-month reassessment:
- Repeat HBV-DNA — the primary efficacy endpoint while on NAs; should remain suppressed
- HBeAg / anti-HBe seroconversion check
- HBsAg quantitative if available
- Repeat ALT/AST/GGT — should be stable or improving
- Repeat synthetic function
Yearly:
- HCC surveillance: liver ultrasound +/- alpha-fetoprotein every 6 months for cirrhotics, every 12 months otherwise (per AASLD)
- Repeat elastography or FIB-4
Stop the Chanca Piedra and contact the hepatologist immediately if:
- ALT rises >2× baseline or >5× upper limit of normal (could be a herb-induced flare or, more concerning, a viral rebound)
- Total bilirubin rises >2× baseline
- Any new jaundice, dark urine, pale stools
- New bruising, bleeding, or marked fatigue (potential synthetic-function decline)
- Rising INR or falling albumin
Limitations of the Evidence Base
It's important to state the weaknesses of the Phyllanthus-HBV literature honestly:
- Heterogeneity — species (P. amarus vs niruri vs urinaria), preparation (powdered herb vs aqueous extract vs alcoholic extract vs standardized capsule), dose (200 mg to 1500 mg/day), duration (30 days to 6 months). Meta-analyses pool incomparable interventions.
- Small sample sizes — most trials have 30-100 patients per arm. Even the Cochrane pool of 1,326 patients is small compared to the registration trials for entecavir (~900 patients per study) and tenofovir.
- Open-label or single-blind design — most pre-2010 trials lacked rigorous blinding. Subjective endpoints (symptom scores) are particularly vulnerable; objective endpoints (HBV-DNA, HBsAg) less so.
- Publication bias toward positive results — Eastern journal publishing patterns, especially in the 1990s, skewed toward positive trials. The Berk 1991 negative replication in The Lancet is a notable exception.
- No modern Phase III RCT — nothing in the past 15 years matches modern Hepatology methodology (sample size, blinding, intention-to-treat analysis, validated PRO endpoints, central HBV-DNA assays). There is no economic incentive: Phyllanthus is unpatentable.
- Surrogate endpoints, not patient-relevant outcomes — HBV-DNA suppression and HBeAg seroconversion are surrogates. The patient-relevant outcomes — HCC incidence, cirrhosis progression, liver-related mortality — have never been measured in a Phyllanthus trial.
This is why responsible integrative hepatology positions Chanca Piedra as a reasonable adjunct in motivated patients with sufficient resources to monitor, not as a recommended therapy for the general HBV population.
Who Should — and Should Not — Try This
Reasonable to consider Chanca Piedra adjunctively if you have:
- Chronic inactive HBV carrier status (HBeAg-negative, normal ALT, low HBV-DNA) — not on antivirals because criteria for therapy aren't met, and looking for additional immunologic pressure to push toward HBsAg loss
- Chronic HBV on entecavir or tenofovir, with HBV-DNA already suppressed, looking for adjunctive support; not on other CYP3A4-substrate medications
- Persistent low-level HBV reactivation after stopping NAs (with hepatology oversight)
- HBV with concurrent NAFLD or alcoholic liver disease where the broader hepatoprotective profile is attractive
- Post-DAA HCV with residual ALT elevation, as part of a broader hepatoprotective stack
Do NOT take Chanca Piedra if you have/are:
- Pregnant or breastfeeding
- About to undergo surgery (stop 2 weeks prior — CYP3A4 and platelet effects)
- On warfarin, tacrolimus, cyclosporine, HIV protease inhibitors, certain statins (especially simvastatin, atorvastatin), or other narrow-therapeutic-window CYP3A4 substrates without explicit hepatology and pharmacy oversight
- Decompensated cirrhosis (Child-Pugh B or C) — the herb's safety profile in advanced cirrhosis is not established and the consequences of any drug-induced liver injury are severe
- Active HBV flare with rising ALT — this needs a hepatologist's eyes, not an herbal trial
- Post-liver-transplant on calcineurin inhibitors — absolute contraindication; tacrolimus levels can fluctuate dramatically with CYP3A4 inhibitors
And the universal rule for any chronic HBV patient: never stop your prescribed antiviral to substitute Chanca Piedra. NA discontinuation flares can be severe. Decisions to stop antivirals belong to the hepatologist using AASLD or EASL criteria, not to the patient or the herbalist.
Key Research Papers
- Thyagarajan SP, Subramanian S, Thirunalasundari T, Venkateswaran PS, Blumberg BS. Effect of Phyllanthus amarus on chronic carriers of hepatitis B virus. Lancet 1988;2(8614):764-6. PMID: 2902528. — Search PubMed · DOI
- Venkateswaran PS, Millman I, Blumberg BS. Effects of an extract from Phyllanthus niruri on hepatitis B and woodchuck hepatitis viruses: in vitro and in vivo studies. Proc Natl Acad Sci USA 1987;84(1):274-8. PMID: 3467354. — PubMed · DOI
- Xia Y, Luo H, Liu JP, Gluud C. Phyllanthus species for chronic hepatitis B virus infection. Cochrane Database Syst Rev 2011;(4):CD008960. PMID: 21491414. — Search PubMed · DOI
- Liu J, Lin H, McIntosh H. Genus Phyllanthus for chronic hepatitis B virus infection: a systematic review. J Viral Hepat 2001;8(5):358-66. PMID: 11555193. — PubMed · DOI
- Shead A, Vickery K, Pajkos A, Medhurst R, Freiman J, Cossart Y. Effects of Phyllanthus plant extracts on duck hepatitis B virus in vitro and in vivo. Antiviral Res 1992;18(2):127-38. PMID: 1417907. — Search PubMed · DOI
- Berk L, de Man RA, Schalm SW, Labadie RP, Heijtink RA. Beneficial effects of Phyllanthus amarus for chronic hepatitis B, not confirmed. J Hepatol 1991;12(3):405-6. PMID: 1845897. — Search PubMed · DOI
- Liu J, McIntosh H, Lin H. Chinese medicinal herbs for chronic hepatitis B: a systematic review. Liver 2001;21(4):280-6. PMID: 11454193. — Search PubMed · DOI
- Patel JR, Tripathi P, Sharma V, Chauhan NS, Dixit VK. Phyllanthus amarus: ethnomedicinal uses, phytochemistry and pharmacology: a review. J Ethnopharmacol 2011;138(2):286-313. PMID: 21982793. — PubMed · DOI
- Calixto JB, Santos AR, Cechinel Filho V, Yunes RA. A review of the plants of the genus Phyllanthus: their chemistry, pharmacology, and therapeutic potential. Med Res Rev 1998;18(4):225-58. PMID: 9664291. — PubMed · DOI
- Wei W, Li X, Wang K, Zheng Z, Zhou M. Lignans with anti-hepatitis B virus activities from Phyllanthus niruri L. Phytother Res 2012;26(7):964-8. PMID: 22162206. — Search PubMed · DOI
- Notka F, Meier GR, Wagner R. Inhibition of wild-type human immunodeficiency virus and reverse transcriptase inhibitor-resistant variants by Phyllanthus amarus. Antiviral Res 2003;58(2):175-86. PMID: 12742577. — PubMed · DOI
- Lam WY, Leung KT, Law PT, et al. Antiviral effect of Phyllanthus nanus ethanolic extract against hepatitis B virus (HBV) by expression microarray analysis. J Cell Biochem 2006;97(4):795-812. PMID: 16329135. — Search PubMed · DOI
PubMed Topic Searches
- PubMed: niranthin HBV polymerase
- PubMed: P. amarus HBsAg loss
- PubMed: Phyllanthus + entecavir
- PubMed: Phyllanthus + tenofovir
- PubMed: HBeAg seroconversion
- PubMed: Phyllanthus & HCV
- PubMed: Phyllanthus & cccDNA
- PubMed: reverse transcriptase
Connections
- Chanca Piedra Overview
- Liver Protection (General)
- Active Compounds (Niranthin Detail)
- Forms, Dosing and Standardization
- Safety and Drug Interactions
- Phyllanthus Species Comparison
- Kidney Stones
- Hepatitis B
- Hepatitis
- Liver Disease
- Cirrhosis
- Non-Alcoholic Fatty Liver Disease
- Milk Thistle
- NAC
- GGT
- Comprehensive Metabolic Panel
- Liver Cleansing