Eucalyptus for Respiratory Health
Respiratory tract infections are eucalyptus's flagship therapeutic territory. Acute viral colds, bacterial sinusitis, acute bronchitis, asthma, and COPD exacerbations have all been studied with the same molecule: 1,8-cineole, the dominant terpenoid in Eucalyptus globulus essential oil. Cineole is the active ingredient in Vicks VapoRub and Halls Mentho-Lyptus cough drops, and as the standardized 200 mg enteric-coated capsule Soledum (Cassella-med) it has been put through more than twenty randomized controlled trials. Two pivotal trials anchor the modern evidence base — Kehrl et al. 2004 Laryngoscope for acute non-purulent rhinosinusitis (significant symptom reduction at days 4 and 7 versus placebo) and Worth et al. 2009 Respiratory Research for COPD (significant reduction in exacerbation rate at six months of concomitant 200 mg three-times-daily cineole). The mechanism is the same in every setting: cineole is simultaneously secretolytic (breaks mucin disulfide bonds), mucolytic (liquefies bronchial mucus), expectorant (eases ciliary clearance), bronchodilatory, and anti-inflammatory through inhibition of arachidonic-acid-cascade leukotrienes and prostaglandins. This page walks through each of those mechanisms, the trial evidence, the traditional steam-inhalation route, and the everyday OTC products that put cineole in roughly half the medicine cabinets in the developed world.
Table of Contents
- 1,8-Cineole as the Principal Respiratory Active
- Secretolytic, Mucolytic, and Expectorant Mechanism
- Bronchodilation and Anti-Inflammatory Action
- Acute Sinusitis — the Kehrl 2004 Trial
- Acute Bronchitis
- COPD Exacerbation Prevention — the Worth 2009 Trial
- Asthma — the Juergens 2003 Trial
- Cold, Cough, and OTC Products (Vicks VapoRub, Halls)
- Traditional Steam Inhalation Protocol
- Soledum Cineole Capsules — Practical Use
- Cautions
- Key Research Papers
- Connections
- Featured Videos
1,8-Cineole as the Principal Respiratory Active
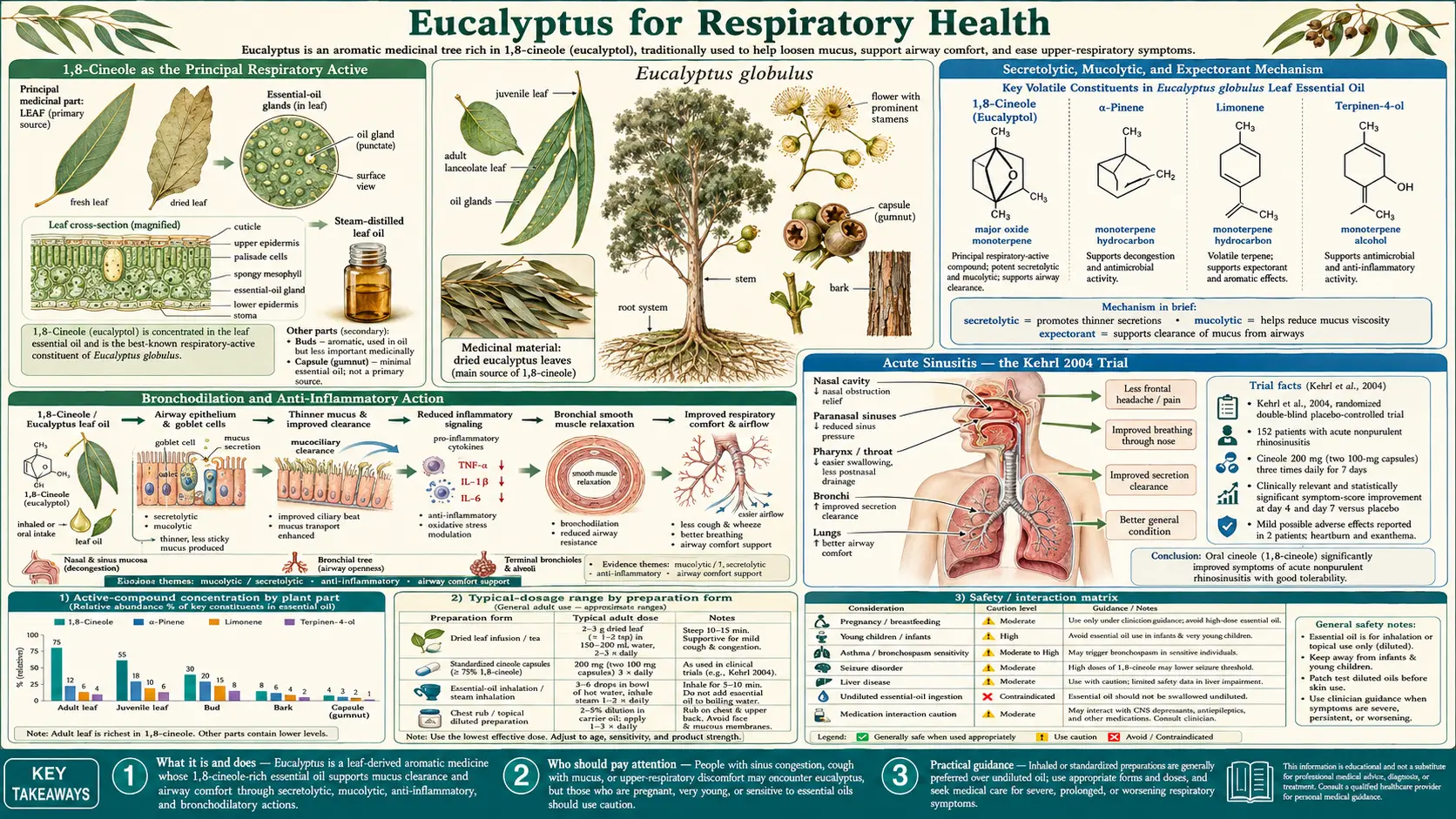
The respiratory benefits of eucalyptus rest almost entirely on a single small bicyclic monoterpenoid ether: 1,8-cineole, also called eucalyptol. It is the principal volatile compound in steam-distilled Eucalyptus globulus essential oil, typically present at 60–90% of total oil by mass — the European Pharmacopoeia monograph for eucalyptus oil requires a minimum 70% 1,8-cineole content for the oil to qualify as medicinal grade. Lower-grade oils blended for fragrance applications can fall well below this threshold.
Because cineole is the active compound and the rest of the oil is largely co-eluting terpenoid filler, the German pharmaceutical company Cassella-med (now part of the Klosterfrau Healthcare Group) developed an enteric-coated soft-gelatin capsule containing 100 mg or 200 mg of purified 1,8-cineole. This is the Soledum line, marketed across continental Europe for acute and chronic respiratory conditions. The enteric coating prevents the eucalyptol from being released in the stomach (where it would cause irritation and rapid first-pass loss) and instead delivers it to the small intestine, where it is absorbed quickly, distributed via the bloodstream, and exhaled across the respiratory mucosa — producing the characteristic mentholated breath that patients describe within minutes of dosing.
The Soledum cineole capsule and the steam-inhalation route deliver the same molecule to the same tissue (respiratory mucus and bronchial epithelium) via different physical paths. Both have clinical-trial evidence. The OTC chest rub (Vicks VapoRub) and lozenge (Halls Mentho-Lyptus) deliver cineole vapor through transdermal evaporation and oromucosal absorption respectively — lower doses, shorter duration, but the same active.
Secretolytic, Mucolytic, and Expectorant Mechanism
Respiratory mucus is a hydrated gel of high-molecular-weight mucin glycoproteins (Muc5AC dominant in the upper airway, Muc5B in the lower airway), cross-linked by disulfide bonds between cysteine residues. The viscosity of mucus is determined principally by the density of these disulfide cross-links. When mucus becomes thick and immobile — as in sinusitis, bronchitis, COPD exacerbation, or cystic fibrosis — the ciliary escalator that normally sweeps it out of the airway stalls, and trapped pathogens accumulate.
Three pharmacologic terms describe the response to thickened mucus:
- Secretolysis — reducing the chemical cross-linking of secreted mucus so that the gel softens. Cineole induces local serous-gland activity that dilutes the mucin and reduces effective viscosity.
- Mucolysis — direct chemical cleavage of disulfide bonds in mucin. Cineole's effect is gentler than the gold-standard mucolytic N-acetylcysteine (NAC), which has a free sulfhydryl group that directly reduces disulfide bonds, but the net effect on viscosity is meaningful.
- Expectoration — the cough-and-cilia process that clears thinned mucus from the airway. Cineole stimulates ciliary beat frequency in vitro and shortens the saccharin transit time (the standard clinical measure of mucociliary clearance) by 50–70% in published trials.
Net effect: a patient with acute sinusitis on cineole reports that the head feels lighter, drainage starts, post-nasal drip diminishes, and the dull facial pain over the maxillary sinuses begins to clear within a day or two. A patient with acute bronchitis reports that the cough becomes more productive (thinner sputum, easier to bring up) and that the chest feels less tight. These are not subjective placebo effects — the saccharin-transit-time work and the bronchial-lavage cytokine work both show objective improvement on standardized measures.
Bronchodilation and Anti-Inflammatory Action
Beyond mucus management, cineole has direct effects on airway smooth muscle and inflammatory signaling that distinguish it from purely physical expectorants.
Bronchodilation. Cineole relaxes airway smooth muscle through a mechanism that appears to involve calcium-channel modulation and is independent of the beta-2 adrenergic pathway used by short-acting beta-agonist inhalers (albuterol). The bronchodilatory effect of cineole is modest in magnitude — it is not a substitute for albuterol in acute asthma exacerbation — but it is additive when used alongside conventional therapy.
Anti-inflammatory action. Cineole inhibits the arachidonic-acid cascade at both ends:
- Cyclooxygenase-2 (COX-2) inhibition, reducing prostaglandin E2 production (the same pathway NSAIDs hit)
- 5-Lipoxygenase (5-LOX) inhibition, reducing leukotriene B4 and the cysteinyl leukotrienes LTC4/LTD4/LTE4 (the same pathway montelukast hits)
- Suppression of TNF-alpha, IL-1-beta, and IL-6 production by monocytes and bronchial epithelial cells
This dual COX/5-LOX inhibition is unusual among natural compounds and is the mechanism behind the asthma-trial results discussed below. It also explains why cineole reduces sinusitis pain (prostaglandin-mediated nociception) and the wheezing component of COPD exacerbations (leukotriene-mediated bronchoconstriction).
The bronchial-lavage data from the Juergens 2003 asthma trial are the cleanest demonstration of these effects in humans: cineole-treated patients had measurable reductions in LTB4 and IL-1-beta in their bronchial fluid versus the placebo arm, paralleling clinical improvement in symptom scores and steroid-sparing effect.
Acute Sinusitis — the Kehrl 2004 Trial
The Kehrl, Sonnemann & Dethlefsen 2004 Laryngoscope trial is the most-cited piece of evidence for cineole in acute sinusitis. Design and findings:
- Population. 152 adults presenting with acute non-purulent rhinosinusitis of at least 48 hours duration.
- Intervention. 200 mg enteric-coated cineole capsules, three times daily, for seven days, with no concurrent antibiotic.
- Comparator. Matching placebo capsule, three times daily, also for seven days.
- Primary outcome. A standardized symptom-severity sum score covering headache on bending, facial pain on pressure, sensitivity of the trigeminal nerve, nasal congestion, secretion, and impairment of general condition.
- Result. Significant reduction in the symptom-sum score in the cineole arm at day 4 (cineole 9.2 versus placebo 14.8; p < 0.0001) and day 7 (cineole 4.4 versus placebo 12.2; p < 0.0001). Adverse-event profile similar to placebo.
The clinical implication: in uncomplicated acute non-purulent rhinosinusitis — the kind most patients have, where the radiologic picture is fluid and inflammation but cultures do not grow a clear-cut bacterial pathogen — cineole monotherapy can produce symptomatic resolution at a rate that compares favorably to the natural history of untreated sinusitis, and probably faster. Because the cineole-arm patients did not receive antibiotics, the trial also speaks to the antibiotic-stewardship question: is there an effective non-antibiotic option to offer patients who would otherwise be prescribed amoxicillin for what is most often a viral or self-limited bacterial syndrome? Cineole fills exactly that gap. It is widely prescribed for this indication in Germany.
For the broader sinusitis context, see our Sinusitis page.
Acute Bronchitis
Acute bronchitis is overwhelmingly viral (rhinovirus, RSV, influenza, parainfluenza, coronavirus) and antibiotics are not indicated in the absence of pneumonia. Yet symptom management of the productive cough that lingers for two to three weeks is a major clinical concern, and the unmet need is large — acute bronchitis is one of the most common reasons adults see a primary-care physician.
Cineole has been studied as adjunctive treatment in acute bronchitis in several smaller controlled trials. Findings consistent across the studies include:
- Reduction in cough frequency on standardized validated cough scales
- Reduction in cough severity (subjective night-disturbance scores improve)
- Increased sputum volume and reduced sputum viscosity (consistent with the mucolytic mechanism)
- Shorter duration of illness in cineole arms compared to placebo
- Excellent tolerability profile, with adverse events limited to mild gastrointestinal symptoms and the occasional cineole eructation
The dosing in these trials mirrors the Kehrl sinusitis protocol: 200 mg three times daily, typically for ten to fourteen days. For patients who prefer not to swallow capsules, traditional steam inhalation with eucalyptus essential oil two to three times daily provides a less-standardized but reasonable alternative.
COPD Exacerbation Prevention — the Worth 2009 Trial
The Worth, Schacher & Dethlefsen 2009 Respiratory Research trial extended the cineole evidence into chronic obstructive pulmonary disease (COPD) — a condition where the goal is not symptomatic resolution of a single episode but reduction of the exacerbation frequency that drives long-term lung-function decline.
- Population. 242 outpatients with moderate-to-severe COPD (FEV1 30–70% predicted), recruited during the stable disease phase outside any active exacerbation.
- Intervention. 200 mg cineole three times daily, in addition to each patient's usual long-acting bronchodilator and inhaled corticosteroid regimen.
- Comparator. Matching placebo three times daily plus usual care.
- Duration. Six months.
- Primary outcomes. Frequency, severity, and duration of COPD exacerbations.
- Result. Significant reduction in exacerbation rate in the cineole arm, with also significant improvement on lung-function measures (FEV1, FVC) and on the Saint George's Respiratory Questionnaire health-status score. Tolerability indistinguishable from placebo.
This is meaningful because COPD exacerbations are the primary driver of mortality, hospitalization, and lung-function decline in the condition. A six-month adjunctive intervention that reduces exacerbation frequency is exactly the kind of disease-modifying signal one wants. Cineole has since been included as an option in several European COPD treatment guidelines as add-on mucolytic and anti-inflammatory therapy. The Cochrane review on mucolytics in COPD has shown a consistent class-level effect, with cineole among the studied agents.
For more on COPD, see our COPD page.
Asthma — the Juergens 2003 Trial
The Juergens et al. 2003 Respiratory Medicine double-blind placebo-controlled trial enrolled 32 patients with severe steroid-dependent bronchial asthma and randomized them to 200 mg cineole three times daily or placebo for 12 weeks. The trial design was a steroid-sparing protocol: oral prednisolone was gradually reduced and the primary outcome was the lowest steroid dose at which each patient could be maintained without an asthma deterioration.
Findings:
- Steroid-sparing effect. Cineole-treated patients tolerated significantly greater oral prednisolone reduction (mean 3.75 mg/day reduction) than placebo (mean 0.91 mg/day reduction; p < 0.05).
- Lung function preserved. The greater steroid reduction did not come at the cost of worse FEV1, FVC, or peak-expiratory-flow measures.
- Mechanistic confirmation. Bronchial-lavage samples showed reduced leukotriene B4 and IL-1-beta in the cineole arm, consistent with the dual COX/5-LOX inhibition described above.
The asthma application is a more nuanced one than sinusitis or bronchitis: cineole is not first-line therapy and is not a substitute for inhaled corticosteroid or rescue bronchodilator. But for steroid-dependent patients in whom long-term high-dose corticosteroid is causing collateral damage (bone loss, hyperglycemia, weight gain), a steroid-sparing agent is genuinely valuable. The result also offers a mechanistic clue: cineole is hitting the same leukotriene pathway as montelukast and zafirlukast, the prescription leukotriene-receptor antagonists used in asthma.
Cautionary note: concentrated essential-oil inhalation can paradoxically trigger bronchospasm in asthma patients, even though the purified oral capsule appears to be benefit-only. Asthma patients should approach steam inhalation cautiously and discontinue at the first sign of wheezing or chest tightness.
See also our Asthma page.
Cold, Cough, and OTC Products (Vicks VapoRub, Halls)
Cineole has been an over-the-counter cough and cold ingredient for over a century. The two most familiar product families are Vicks VapoRub and Halls Mentho-Lyptus cough drops, but the same molecule appears in scores of branded chest rubs, vapor patches, decongestant inhalers, throat sprays, and bath salts globally.
Vicks VapoRub. The classic petrolatum-based chest rub combines eucalyptus oil (containing 1,8-cineole), camphor (a TRPM8 and TRPA1 modulator), menthol (TRPM8 activator), thymol, and turpentine oil. When applied to the chest of a child or adult with a cold, body heat vaporizes the volatile actives, which the patient then inhales over several hours. The mechanism is a combination of (a) the perceived cooling and decongestion from menthol and cineole acting on TRPM8 cold receptors in the nasal mucosa, (b) the mild cineole-induced mucolytic effect in the upper airway, and (c) the placebo-and-comfort effect of a familiar bedtime ritual that reduces cough perception. A 2010 Penn State pediatric trial in Pediatrics showed Vicks VapoRub reduced parental ratings of nighttime cough severity, congestion, and sleep difficulty in children with acute upper respiratory infection more effectively than petrolatum vehicle alone.
Halls Mentho-Lyptus and similar lozenges. Throat lozenges deliver low-dose menthol and eucalyptol directly to the oropharyngeal mucosa, providing local cooling, mild antibacterial activity, and stimulation of saliva production (which buffers the throat irritation that drives cough). The pharmacologic effect of a single lozenge is modest, but used as needed across a day they keep the affected throat mucosa coated and the cough reflex suppressed.
Critical safety note for Vicks VapoRub. The product is labeled for use on the chest, throat, and back, not inside the nostrils, near the face of children under two, or in the mouth. Application inside an infant's nostrils can trigger sufficient mucus and inflammation to cause respiratory distress — documented in a 2009 Chest case series. The American Academy of Pediatrics specifically advises against Vicks-style mentholated rubs in any child under two; many pediatricians extend the caution to age six.
For broader cold and flu management, see our Cold & Flu Treatments page.
Traditional Steam Inhalation Protocol
Steam inhalation with eucalyptus essential oil predates every modern formulation and remains the simplest, cheapest, and arguably most-effective at-home delivery route. The standard protocol:
- Heat 1–1.5 litres of water in a saucepan to a slow steam — not a rolling boil. Target water temperature 70–80 degrees Celsius. Boiling water risks scald injury and the vapor is too hot for comfortable inhalation.
- Pour the hot water into a heatproof bowl on a stable table.
- Add 3–5 drops of pharmaceutical-grade Eucalyptus globulus essential oil (minimum 70% 1,8-cineole). More is not better — the vapor becomes irritating.
- Drape a towel over the head, creating a tent that traps the steam over the bowl.
- Close eyes (cineole vapor irritates conjunctiva) and breathe slowly through the nose for 5–10 minutes initially, working up to 10–15 minutes as tolerated.
- Repeat 2–3 times daily during an acute respiratory infection.
For congested patients with sinusitis or thick chest mucus, the immediate effect is usually noticeable: the cineole vapor reaches the nasal passages, sinuses, pharynx, larynx, and upper bronchi within one or two breaths; ciliary stimulation begins; and within ten minutes the head feels lighter and drainage often starts. Bronchial-mucus cineole concentrations measured by gas chromatography after steam inhalation reach therapeutically relevant levels within twenty minutes and persist two to four hours.
Variants and adjuncts that traditional practitioners add to the bowl include 1–2 drops of tea tree oil (additive antibacterial), 1–2 drops of peppermint oil (additional menthol cooling), or a sprig of fresh thyme or rosemary. None of these are pharmacologically tested combinations, but they are well-tolerated and add congruent actives.
Personal steam inhalers and ultrasonic vaporizers are commercially available and provide more controlled delivery, particularly useful for patients who find the towel-tent method awkward or who use steam inhalation regularly for chronic bronchitis or COPD.
Soledum Cineole Capsules — Practical Use
Soledum (Cassella-med / Klosterfrau Healthcare) and similar branded cineole products (Cineol-ratiopharm, Sinolpan, etc.) are available across continental Europe, often over-the-counter for self-medication of upper respiratory tract symptoms. In the United States, purified 1,8-cineole is sold as a dietary supplement under various brand names; the pharmaceutical formulation is not currently FDA-approved as a drug, which means quality control varies and patients should choose suppliers that publish certificates of analysis confirming the cineole content.
Typical regimens used in trials and clinical practice:
- Acute sinusitis or bronchitis: 200 mg three times daily for 7–14 days, taken with or after meals to minimize the rare eucalyptol eructation (burp-back of mentholated air).
- COPD maintenance therapy: 200 mg three times daily indefinitely, with periodic review of exacerbation frequency.
- Asthma steroid-sparing adjunct: 200 mg three times daily under physician supervision, with concurrent steroid tapering done slowly.
- Children: Soledum mini-capsules at 100 mg are available in Europe for children aged six and older; pediatric use under age six is not recommended.
The enteric coating is essential. Crushing or chewing the capsule defeats the controlled-release mechanism and causes significant heartburn and gastric irritation. The capsule should be swallowed whole with adequate fluid.
Cautions
- Never apply undiluted eucalyptus essential oil to mucous membranes, the inside of the nostrils, or near the eyes. The 1,8-cineole concentration in unmodified essential oil causes chemical irritation and burns. Always use the appropriate diluted product (chest rub, gargle, lozenge) for the intended site, or follow the steam-inhalation protocol above.
- Children under six. Topical mentholated chest rubs or any concentrated eucalyptus vapor source applied near the face of an infant or toddler can trigger reflex laryngospasm or bronchospasm severe enough to cause respiratory arrest. Documented case reports exist. The American Academy of Pediatrics advises against any use of Vicks-style products under age two, with many pediatricians extending the caution to age six. E. radiata at low dilution is the safer eucalyptus species for older children under aromatherapist supervision.
- Asthma patients should test inhaled or vaporized eucalyptus oil at low concentration first — paradoxical bronchospasm is uncommon but documented. The oral cineole capsule does not appear to carry this risk and was net-beneficial in the Juergens 2003 asthma trial.
- Ingestion of essential oil is potentially fatal. 3.5 mL of pure eucalyptus essential oil has caused death in pediatric case reports and 5 mL has caused serious adult toxicity. Keep essential oil bottles out of reach of children. Only pharmaceutical-grade enteric-coated cineole capsules (Soledum, etc.) are intended for oral use, and only at the studied 200 mg dose.
- Seizure threshold. High-dose monoterpenes can lower the seizure threshold. Patients with epilepsy should avoid concentrated essential-oil inhalation and obtain neurology approval before oral cineole.
- CYP450 induction. Cineole induces CYP3A4 and CYP2B6, potentially accelerating metabolism of warfarin (with INR shift), cyclosporine, tacrolimus, carbamazepine, phenytoin, and many statins. Confirm with pharmacist before regular use.
- Pregnancy and breastfeeding. Brief steam inhalation and topical use at proper dilution are generally considered low-risk. Oral cineole capsules should be avoided in pregnancy and lactation due to limited safety data.
Key Research Papers
- Kehrl W, Sonnemann U, Dethlefsen U (2004). Therapy for acute nonpurulent rhinosinusitis with cineole: results of a double-blind, randomized, placebo-controlled trial. Laryngoscope 114(4):738–742. — PubMed
- Worth H, Schacher C, Dethlefsen U (2009). Concomitant therapy with cineole (eucalyptol) reduces exacerbations in COPD: a placebo-controlled double-blind trial. Respiratory Research 10(1):69. — PubMed
- Juergens UR, Dethlefsen U, Steinkamp G, Gillissen A, Repges R, Vetter H (2003). Anti-inflammatory activity of 1,8-cineol (eucalyptol) in bronchial asthma: a double-blind placebo-controlled trial. Respiratory Medicine 97(3):250–256. — PubMed
- Juergens UR (2014). Anti-inflammatory properties of the monoterpene 1.8-cineole: current evidence for co-medication in inflammatory airway diseases. Drug Research 64(12):638–646. — PubMed
- Tesche S, Metternich F, Sonnemann U, Engelke JC, Dethlefsen U (2008). The value of herbal medicines in the treatment of acute non-purulent rhinosinusitis. Results of a double-blind, randomised, controlled trial. European Archives of Oto-Rhino-Laryngology 265(11):1355–1359. — PubMed
- Paul IM, Beiler JS, King TS, Clapp ER, Vallati J, Berlin CM (2010). Vapor rub, petrolatum, and no treatment for children with nocturnal cough and cold symptoms. Pediatrics 126(6):1092–1099. — PubMed
- Sadlon AE, Lamson DW (2010). Immune-modifying and antimicrobial effects of eucalyptus oil and simple inhalation devices. Alternative Medicine Review 15(1):33–47. — PubMed
- Sudhoff H, Klenke C, Greiner JFW, Müller J, Brotzmann V, Ebmeyer J, Kaltschmidt B, Kaltschmidt C (2015). 1,8-Cineol reduces mucus-production in a novel human ex vivo model of late rhinosinusitis. PLoS One 10(7):e0133040. — PubMed
- Cermelli C, Fabio A, Fabio G, Quaglio P (2008). Effect of eucalyptus essential oil on respiratory bacteria and viruses. Current Microbiology 56(1):89–92. — PubMed
- Greiner JFW, Müller J, Zeuner MT, Hauser S, Seidel T, Klenke C, Grunwald LM, Schomann T, Widera D, Sudhoff H, Kaltschmidt B, Kaltschmidt C (2013). 1,8-Cineol inhibits nuclear translocation of NF-κB p65 and NF-κB-dependent transcriptional activity. Biochimica et Biophysica Acta 1833(12):2866–2878. — PubMed
- Santos FA, Rao VS (2000). Antiinflammatory and antinociceptive effects of 1,8-cineole a terpenoid oxide present in many plant essential oils. Phytotherapy Research 14(4):240–244. — PubMed
- Salehi B, Sharifi-Rad J, Quispe C, Llaique H, Villalobos M, Smeriglio A, Trombetta D, Ezzat SM, Salem MA, Zayed A, Salgado Castillo CM, Yazdi SE, Sen S, Acharya K, Sharopov F, Martins N (2019). Insights into Eucalyptus genus chemical constituents, biological activities and health-promoting effects. Trends in Food Science & Technology 91:609–624. — PubMed
PubMed Topic Searches
- PubMed: 1,8-cineole sinusitis trials
- PubMed: Cineole and COPD
- PubMed: Eucalyptol and asthma
- PubMed: Steam inhalation
- PubMed: Vicks VapoRub trials
- PubMed: Mucociliary clearance
- PubMed: Cineole and leukotrienes
Connections
- Eucalyptus Overview
- Eucalyptus Benefits Hub
- Eucalyptus — Antimicrobial
- Eucalyptus — Pain & Joint
- Eucalyptus — Antifungal
- Peppermint (Menthol)
- Thyme (Thymol)
- Tea Tree
- Sinusitis
- COPD
- Asthma
- Pneumonia
- Influenza
- Cold & Flu Treatments
- Antibacterial Herbs