Common Cold
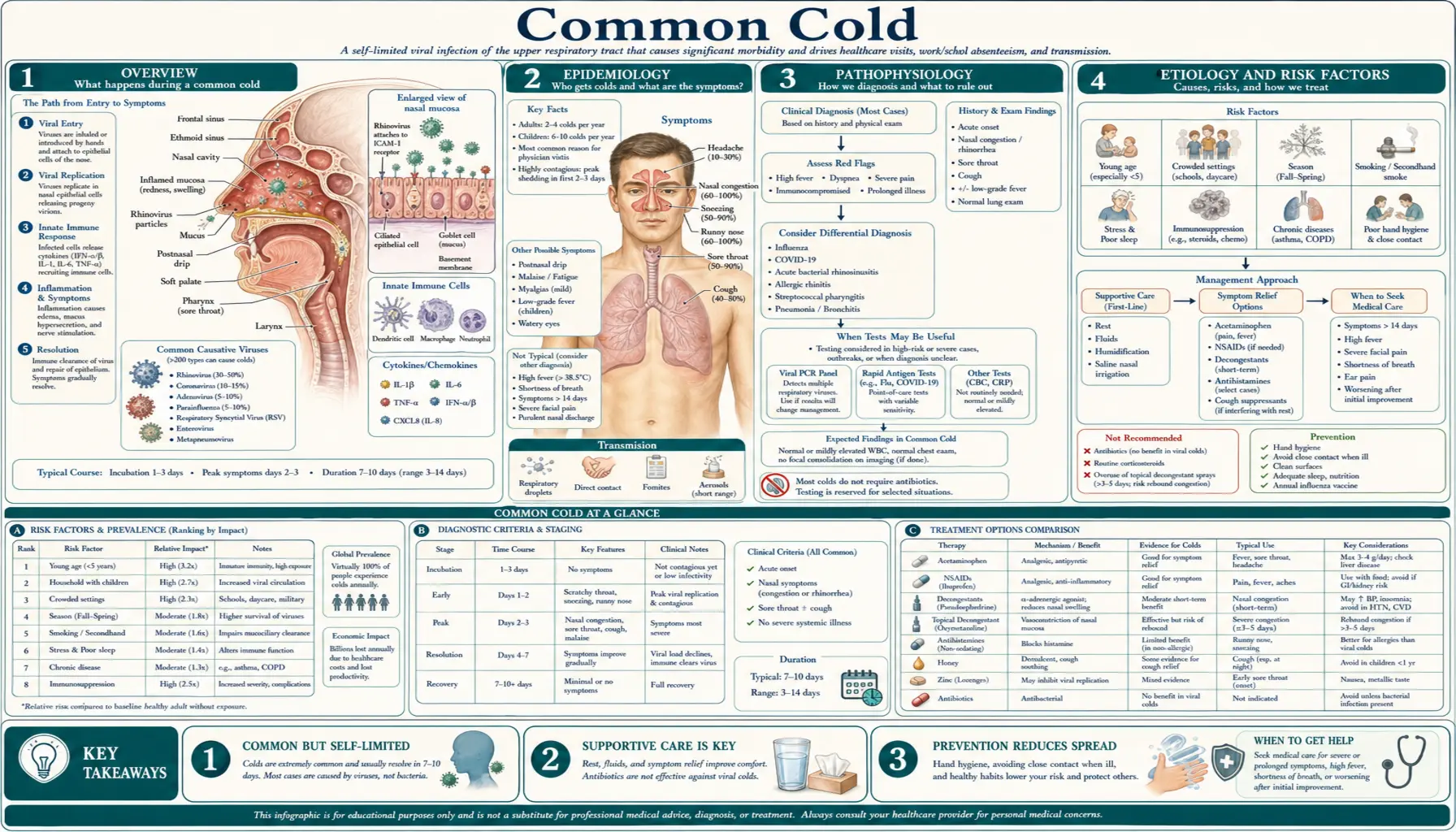
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- Research Papers
- Connections
- Featured Videos
1. Overview
The common cold is a mild, self-limiting viral infection of the upper respiratory tract — mainly the nose, throat, and sinuses. It is, quite simply, the most common human illness on Earth. The average adult catches 2–3 colds a year, and young children — whose immune systems are still meeting these viruses for the first time, and who spend their days in close quarters at daycare and school — average 6–8 colds a year, sometimes more. Over a lifetime, most people will have a cold a few hundred times.
Here is the honest, useful truth that runs through this whole page: a cold is caused by a virus, it will get better on its own in about a week, and there is no cure. That sounds discouraging, but it is actually empowering — because it means the entire game is about feeling less miserable while your own immune system clears the infection, and about not catching one in the first place. Some natural and over-the-counter remedies genuinely help a little; many do nothing; and a few popular products were recently proven useless by the FDA. This page sorts them out with real numbers from real trials, so you can spend your money and effort on what actually works.
The illness is generally harmless, but it is worth knowing the small handful of situations where what looks like “just a cold” is something that needs attention — a sinus infection that has set in, strep throat, the flu, or a chest infection. We cover those red flags too, so you know when to wait it out and when to call someone.
2. Epidemiology
Colds are everywhere, all the time, but they cluster in the colder months. In temperate climates the season runs roughly from early autumn through spring, peaking in winter. In the United States alone, colds cause an estimated tens of millions of missed school and work days each year and drive a large share of doctor visits and over-the-counter spending — Americans spend several billion dollars annually on cold remedies, many of which do little.
Children are the great reservoir and amplifier of colds. A preschooler with 6–8 colds a year reliably brings them home to parents and siblings. Adults living with young children, teachers, daycare workers, and healthcare staff all see more colds than average. The number of colds tends to fall as we age and accumulate immune memory, which is why a healthy older adult often gets fewer colds than a toddler — though for frail elderly people, a “cold” can occasionally be a more serious respiratory virus in disguise.
Why winter? It is not simply “the cold weather.” Two things stack up. First, people crowd indoors in heated, poorly ventilated rooms, so viruses pass from person to person more easily. Second — and this is the more surprising part — the slightly cooler temperature inside your nose in winter actually weakens your nasal lining's first-line antiviral defenses. Researchers led by Ellen Foxman showed that rhinovirus, the leading cold virus, replicates more readily at the cooler 33–35 °C of the nasal passages than at core body temperature, partly because the innate immune (interferon) response is blunted at lower temperatures. So a chilly nose is genuinely a friendlier place for the virus. (To be clear: going outside with wet hair does not give you a cold — you still need to encounter the virus — but cold air may give that virus a small head start once you do.)
3. Pathophysiology
A cold begins when virus particles land on the lining of your nose, throat, or eyes and infect the cells of the respiratory epithelium. Within a day or two the virus is replicating, and — here is the part that surprises most people — most of your symptoms are not caused by the virus directly. They are caused by your own immune response. The infected cells release inflammatory signaling molecules (cytokines and kinins), which dilate blood vessels, leak fluid into the tissues, and stimulate nerve endings.
That immune reaction is what produces the familiar misery: the swollen, congested nasal lining (the “stuffy nose” is inflamed tissue, not just mucus), the runny nose as glands pour out watery secretions, the sneezing and the scratchy, sore throat as nerves are irritated, and the cough as the airway becomes twitchy and inflamed. This is why anti-inflammatory and symptom-targeting measures help even though they do nothing to the virus itself — they turn down the volume on your own reaction.
It also explains the timeline. The virus is typically cleared within several days, but the inflammation it triggered — especially in the lower airway — can linger. That is why the cough is the last symptom to leave, often hanging on for one to two weeks after everything else has settled, as the irritated airway slowly calms down.
This immune-driven model, worked out in detail by researchers such as Ron Eccles, also reframes how we should think about treatment. If the symptoms are your body's inflammatory reaction rather than the virus's direct damage, then the most effective everyday measures are the ones that calm inflammation and ease the mechanical problems it creates — reducing swelling, thinning and clearing mucus, soothing irritated nerve endings — rather than chasing the virus itself with an “antiviral” product. It is also why the same cold can feel very different from one person to the next: the intensity of your symptoms tracks the vigor of your own immune response as much as the particular virus you caught.
4. Etiology and Risk Factors
More than 200 different viruses can cause the common cold, which is the fundamental reason there will probably never be a single vaccine. The biggest player by far is rhinovirus, responsible for roughly half of all colds, with well over a hundred distinct serotypes that your immune system has to learn one by one. Other culprits include parainfluenza viruses, respiratory syncytial virus (RSV), adenoviruses, metapneumovirus, and other respiratory viruses. Because so many different viruses (and so many rhinovirus strains) are circulating, recovering from one cold gives you essentially no protection against the next.
How colds actually spread (and why this matters)
For a long time colds were thought to spread mainly through coughs and sneezes — airborne droplets. We now understand that hands and contaminated surfaces matter at least as much. The chain works like this: an infected person rubs their runny nose or covers a cough, transferring virus to their hands. They touch a doorknob, a phone, a shopping cart, a faucet. You touch the same surface, then — as everyone does, dozens of times an hour without noticing — you touch your eyes or nose. That is called self-inoculation, and it is a major route of infection. Rhinovirus can survive for hours on hard surfaces.
The single most important practical implication of this whole page is here: because so much transmission runs through your hands and your face, frequent handwashing and not touching your eyes and nose beat almost everything else for avoiding a cold. It is unglamorous and free, and it works better than any supplement.
Who catches more colds
- Young children and the people who live and work with them — the dominant risk factor.
- People who sleep poorly. In rhinovirus-challenge studies, getting fewer than 7 hours of sleep was associated with roughly three times the risk of developing a cold compared with 8+ hours (see Prevention).
- People under sustained psychological stress — classic studies by Sheldon Cohen showed chronic stress measurably raises the odds of getting sick after exposure.
- Smokers and those with damaged airways.
- People with low vitamin D, where deficiency is common (the benefit is mainly in correcting a real deficiency, not in megadosing — see below).
5. Clinical Presentation
A cold has a remarkably predictable arc. Knowing it helps you tell a normal cold from something that needs more attention.
The day-by-day timeline
- Day 1–2: It usually starts with a scratchy or sore throat and a vague feeling of being “off.” Sneezing and a clear, runny nose begin.
- Day 2–4: Symptoms peak. Nasal congestion is at its worst, the nose may switch from runny to blocked, and a mild cough often starts. You feel most miserable here.
- Day 4–7: Things slowly improve. Congestion eases, energy returns.
- Week 1–2: Most symptoms are gone, but the cough commonly lingers for another week or two as the airway settles. A lingering cough alone is normal and not a sign of a bacterial infection.
About green or yellow mucus
This is one of the most persistent myths in medicine, so let us be direct: green or yellow snot does NOT mean you have a bacterial infection or need antibiotics. The color comes from an enzyme (myeloperoxidase) inside your own white blood cells that have rushed in to fight the virus. Colored mucus is simply a sign your immune system is working, and it is completely normal during the middle of an ordinary viral cold. Color alone is not a reason for antibiotics.
Cold vs. flu vs. allergies
These three get confused constantly. Here is how to tell them apart.
It is probably a cold if:
- Symptoms come on gradually over a day or two.
- A sore throat and runny/stuffy nose lead the way; sneezing is common.
- Fever is absent or mild (more common in children than adults).
- Body aches and fatigue are mild; you can usually still function.
It is more likely the flu if:
- It hits suddenly — you can often name the hour you felt terrible.
- High fever, severe body aches, and exhaustion dominate — you feel knocked flat and want to stay in bed.
- Headache and dry cough are prominent; runny nose is less central than in a cold.
It is more likely allergies if:
- Symptoms last weeks or recur every year at the same season, not 7–10 days.
- Itchy, watery eyes and itchy nose with lots of sneezing and clear drainage.
- No fever, no body aches, and you don't feel sick all over.
- Symptoms flare with a clear trigger (pollen, dust, pets) and ease with antihistamines.
6. Diagnosis
A cold is a clinical diagnosis — meaning it is recognized by its typical story and symptoms, not by a test. No blood work, swab, or imaging is needed for an ordinary cold, and ordering them would only add cost and worry. The main job of a clinician (or of you, at home) is really to rule out the look-alikes that do need treatment: influenza, strep throat, a bacterial sinus infection, bronchitis, or pneumonia.
Testing is reserved for specific situations — for example, a rapid flu or strep test when those are suspected and treatment would change, or imaging if pneumonia is a concern. For the vast majority of colds, the right “test” is simply time: a cold that follows the normal arc and improves within about a week confirms itself.
7. Treatment
This is the section most people came for, so we will be thorough and honest. Nothing cures a cold or makes the virus vanish. Everything below either shortens a cold modestly, eases symptoms, or — in several popular cases — does nothing at all. We give you the real effect sizes from real trials so you can choose well.
Remedies with genuine (if modest) evidence
Zinc lozenges — the strongest natural option, but the details matter. Meta-analyses by Harri Hemilä and colleagues found that zinc acetate lozenges, used correctly, shortened colds by roughly one-third on average. To get this effect you need: the lozenge form (not pills or syrup, because zinc has to contact the throat tissue), a high daily dose of around 75 mg or more of elemental zinc spread across the day, and you must start within about 24 hours of the first symptom. Started late, it does little. One firm warning: avoid intranasal zinc (gels and sprays) — these have been linked to permanent loss of smell (anosmia) and were pulled from some markets. Zinc lozenges can cause nausea and a bad taste; do not use high-dose zinc for more than a week or two at a time.
Vitamin C — helpful as a daily habit, not as a rescue. This is the most misunderstood remedy of all. The large Cochrane review (Hemilä & Chalker) is clear on two points. First, taking vitamin C only after you already feel a cold coming on does not help — the trials show no benefit when started at onset. Second, taking it regularly every day, before you get sick, shortens the average cold by a small amount: about 8% in adults and 14% in children — trimming a 7-day cold by roughly half a day. There is one striking exception: in people under extreme physical stress — marathon runners, soldiers in subarctic training, skiers — regular vitamin C roughly halved the risk of catching a cold. For the average person, megadosing vitamin C once symptoms start is the wrong strategy; a steady modest daily intake is the evidence-based one.
Honey — the best-supported cough remedy, and it's in your kitchen. In pediatric randomized trials (Paul et al.), a spoonful of honey at bedtime relieved nighttime cough and improved sleep better than dextromethorphan (the “DM” in many cough syrups) and better than no treatment. Honey is cheap, pleasant, and safe for adults and children over one year. Never give honey to an infant under 12 months — risk of infant botulism.
Nasal saline irrigation — real but modest. Rinsing the nose with salt water (neti pot, squeeze bottle, or saline spray) provides a real, if small, reduction in congestion and symptoms in upper-respiratory infections (King et al., Cochrane). It is safe and drug-free. Critical safety rule: use only distilled, sterile, or previously boiled-and-cooled water — never straight tap water — to avoid rare but dangerous infections.
Echinacea — mixed, possibly a small benefit. The evidence is genuinely inconsistent. The Cochrane review (Karsch-Völk et al.) concluded that any benefit, if present, is small, and that products vary so much (different species, plant parts, and preparations) that results don't transfer between them. Reasonable to try, honest to say it may do little.
Elderberry (Sambucus nigra) — promising but limited. Small randomized trials and a meta-analysis (Tiralongo et al.; Hawkins et al.) suggest elderberry extract may modestly reduce the duration and severity of cold and flu-like symptoms. The studies are small and some were industry-funded, so this is “encouraging but not proven.”
Pelargonium sidoides (umckaloabo, South African geranium) — some positive trials, low certainty. Several trials suggest this herbal extract may ease symptoms and shorten cold and bronchitis episodes, but the Cochrane review (Timmer et al.) rated the certainty of evidence as low. A reasonable option for some, with realistic expectations.
Garlic — one trial, not enough to know. The Cochrane review (Lissiman et al.) found only a single decent randomized trial suggesting fewer colds with daily garlic, which is far too little evidence to recommend it confidently. Harmless to try; don't expect much.
What does NOT work (save your money)
- Antibiotics. Colds are viral, and antibiotics kill bacteria, not viruses. They cannot help a cold, they cause side effects (rashes, diarrhea, yeast infections), and overusing them breeds antibiotic resistance. Taking an antibiotic “just in case” for a cold is all risk and no benefit.
- Oral phenylephrine. This is the decongestant in many “non-drowsy” daytime cold pills sold on open shelves (look for “PE” on the box). A meta-analysis (Hatton et al.) and, in September 2023, an FDA advisory panel concluded that oral phenylephrine does not work as a decongestant at approved doses — it is broken down before enough reaches your nose. The decongestant that does work is pseudoephedrine, which is kept behind the pharmacy counter (you show ID, but no prescription). This is one of the most practical things on this page: if you want a real oral decongestant, ask the pharmacist for pseudoephedrine and skip the phenylephrine products.
- Megadosing vitamin C after symptoms start — as above, no proven benefit once the cold has begun.
Symptomatic care — the unglamorous things that genuinely help you feel better
None of these touch the virus, but they make the week far more bearable, and several have a real evidence base behind them:
- Rest and fluids. Sleep supports your immune response; fluids keep mucus thinner and you hydrated. Warm drinks — tea, broth, hot water with honey and lemon — provide genuine, if temporary, relief of runny nose, cough, sore throat, and that “tired and chilly” feeling, partly through the soothing warm vapor and partly through simple comfort.
- NSAIDs (ibuprofen, naproxen) or acetaminophen for headache, sore throat, body aches, and fever. NSAIDs in particular target the inflammatory aches and pains of a cold. Use the lowest effective dose and follow the label; combine carefully if you are also taking a multi-symptom cold product that already contains acetaminophen.
- A humidifier or steamy shower to ease congestion and a raw throat. Keep humidifiers clean to avoid mold.
- Saltwater gargle and throat lozenges for sore throat — cheap, safe, and soothing.
- Menthol rubs and vapors create a cooling sensation that can make breathing feel easier even when they don't measurably open the airway — a small comfort benefit, especially at bedtime.
- First-generation antihistamine + decongestant combinations give a modest reduction in runny nose and sneezing in adults (De Sutter et al., Cochrane); antihistamines alone do little for colds. The older sedating antihistamines may help slightly by drying secretions, at the cost of drowsiness. Do not give over-the-counter cough and cold medicines to children under 4 — they don't help and can cause real harm. For young children, honey (over age 1), fluids, saline drops, and a humidifier are the safe mainstays.
8. Complications
The vast majority of colds resolve with no trouble at all. But because a cold inflames and congests the airways, it occasionally sets the stage for a secondary problem — usually when blocked sinuses or ears can't drain.
- Acute sinusitis — if a sinus stays blocked, bacteria can take hold. The classic clue is a cold that lasts more than 10 days without improving, or that gets better and then noticeably worse again (a “double-sickening” pattern), often with facial pain and pressure.
- Middle-ear infection (otitis media) — common in children, when the tube draining the middle ear gets blocked.
- Asthma or COPD flare-ups — in people with these conditions, a cold is a frequent trigger for wheezing and shortness of breath.
- Bronchitis — the cough drops into the chest; usually still viral and self-limited.
- Pneumonia — uncommon as a complication of a simple cold, but a concern in older adults, infants, and people with weak immune systems.
When it is NOT just a cold — red flags
Watch for these. They suggest something beyond an ordinary cold and a reason to seek care:
- Symptoms lasting more than 10 days with no improvement, or a biphasic course (better, then suddenly worse) — think sinusitis.
- A severe sore throat without a cough, often with fever and swollen glands — think strep throat, which needs a test and possibly antibiotics.
- Sudden high fever with severe body aches and exhaustion — think influenza (antiviral treatment helps most if started early).
- Wheezing, shortness of breath, chest pain, or coughing that worsens rather than fades.
- Infants, the elderly, and immunocompromised people — lower the threshold to seek care; in babies and frail seniors, a “cold” can be RSV or another more serious respiratory virus.
9. Prognosis
The outlook for a common cold is excellent. It is, by definition, a self-limiting illness: the average cold runs its course in about 7 to 10 days, with the worst of it concentrated in the first three or four days and a tail-end cough that may linger a week or two longer. Full recovery is the rule, with no lasting effects.
The main thing that worsens the prognosis is not the cold itself but its occasional complications — a sinus infection, an ear infection, or a flare of asthma or COPD — or mistaking a more serious illness (flu, strep, pneumonia, RSV) for a simple cold. For the otherwise healthy person, the realistic expectation is simple: you will feel rotten for a few days, gradually better over a week, and then fine, whether or not you take anything.
10. Prevention
Prevention is where you have the most real power — and the most effective measures cost nothing.
- Wash your hands — the number-one defense. Frequent soap-and-water handwashing (or alcohol-based sanitizer) directly interrupts the hand-to-face route that drives so many colds. Reviews of physical interventions (Jefferson et al., Cochrane) consistently find hand hygiene reduces respiratory infection spread. This beats every pill on this page.
- Keep your hands away from your eyes and nose. This is the other half of the same coin — even clean hands shouldn't ferry virus to your mucous membranes.
- Sleep. This is one of the most striking findings in cold research. In rhinovirus-challenge studies, people sleeping fewer than 7 hours had about three times the risk of getting sick after exposure compared with those getting 8+ hours, and poorer sleep efficiency raised risk further (Prather et al.; Cohen et al.). Sleep is a legitimate, evidence-based cold-prevention strategy.
- Exercise — in moderation. Regular moderate exercise is associated with fewer and shorter upper-respiratory infections; data from David Nieman and colleagues link regular activity to reduced sick-days. (Note that extreme exertion like a marathon can briefly raise infection risk — the one situation where vitamin C clearly helps.)
- Vitamin D — correct a deficiency, don't megadose. Honestly stated: vitamin D supplementation reduces respiratory infections mainly in people who are actually deficient. If your level is low, correcting it is reasonable; if it is already adequate, more is not better.
- Manage stress. Sheldon Cohen's classic studies showed that sustained psychological stress measurably increases susceptibility to colds after viral exposure. Stress reduction is a real, if indirect, prevention tool.
- Don't smoke, and ventilate indoor spaces in winter.
11. Recent Research and Advances
Cold research has quietly produced some genuinely useful and surprising findings in recent years. Ellen Foxman's temperature work gave a mechanistic answer to the old “why winter” question by showing that the cooler temperature of the nasal passages weakens the innate (interferon) antiviral response, letting rhinovirus replicate more freely — a clean explanation for the cold-weather peak that doesn't rely on folk wisdom.
The sleep–immunity link has been put on firm experimental footing by Aric Prather and Sheldon Cohen, whose rhinovirus-challenge studies quantified just how much short sleep raises infection risk. On the treatment side, the zinc acetate lozenge meta-analyses by Harri Hemilä refined exactly which form, dose, and timing of zinc actually shortens colds — turning a muddled field into a clear, if demanding, protocol.
Perhaps the most consequential recent development for everyday consumers was the September 2023 FDA advisory panel conclusion that oral phenylephrine is ineffective as a decongestant — a finding that affects a huge category of products on pharmacy shelves and that redirects people toward pseudoephedrine, which works. Meanwhile, drug developers continue to chase broad-spectrum antiviral strategies (for example, targeting host proteins that many rhinovirus strains depend on), but the sheer diversity of cold viruses — 200-plus, with rhinovirus alone having well over a hundred serotypes — remains the fundamental obstacle to any universal cure or vaccine.
12. References & Research
Historical Background
Humanity has battled the cold for millennia without ever conquering it, and the modern scientific story is surprisingly recent and rather British. From 1946 to 1989, the United Kingdom's famous Common Cold Unit near Salisbury ran one of the most unusual research programs in medical history: thousands of paid volunteers spent ten days in isolation, were deliberately given cold viruses through nose drops, and were studied in detail — sometimes while researchers tested whether getting chilled or sitting in wet socks made any difference (it didn't, on its own). It was at this unit and in parallel work that the leading cause of the common cold, rhinovirus, was identified in 1956. Later, psychologist Sheldon Cohen used the same controlled-exposure approach to prove that psychological stress and poor sleep genuinely raise the odds of falling ill. The central reason we still have no cure and no vaccine is also the reason the Common Cold Unit never “solved” the cold: there are more than 200 causative viruses, and rhinovirus alone has well over a hundred serotypes, so there is no single target to aim at.
Key Research Papers
- Hemilä H, Chalker E. Vitamin C for preventing and treating the common cold. Cochrane Database of Systematic Reviews. 2013;(1):CD000980.
- Hemilä H. Zinc lozenges and the common cold: a meta-analysis comparing zinc acetate and zinc gluconate, and the role of zinc dosage. JRSM Open. 2017;8(5):2054270417694291.
- Paul IM, Beiler J, McMonagle A, et al. Effect of honey, dextromethorphan, and no treatment on nocturnal cough and sleep quality for coughing children and their parents. Archives of Pediatrics & Adolescent Medicine. 2007;161(12):1140-1146.
- Foxman EF, Storer JA, Fitzgerald ME, et al. Temperature-dependent innate defense against the common cold virus limits viral replication at warm temperature in mouse airway cells. Proceedings of the National Academy of Sciences. 2015;112(3):827-832.
- Karsch-Völk M, Barrett B, Kiefer D, et al. Echinacea for preventing and treating the common cold. Cochrane Database of Systematic Reviews. 2014;(2):CD000530.
- Prather AA, Janicki-Deverts D, Hall MH, Cohen S. Behaviorally assessed sleep and susceptibility to the common cold. Sleep. 2015;38(9):1353-1359.
- Cohen S, Tyrrell DA, Smith AP. Psychological stress and susceptibility to the common cold. New England Journal of Medicine. 1991;325(9):606-612.
- Cohen S, Doyle WJ, Alper CM, et al. Sleep habits and susceptibility to the common cold. Archives of Internal Medicine. 2009;169(1):62-67.
- Tiralongo E, Wee SS, Lea RA. Elderberry supplementation reduces cold duration and symptoms in air-travellers: a randomized, double-blind placebo-controlled clinical trial. Nutrients. 2016;8(4):182.
- Hawkins J, Baker C, Cherry L, Dunne E. Black elderberry (Sambucus nigra) supplementation effectively treats upper respiratory symptoms: a meta-analysis of randomized, controlled clinical trials. Complementary Therapies in Medicine. 2019;42:361-365.
- King D, Mitchell B, Williams CP, Spurling GK. Saline nasal irrigation for acute upper respiratory tract infections. Cochrane Database of Systematic Reviews. 2015;(4):CD006821.
- Timmer A, Günther J, Motschall E, et al. Pelargonium sidoides extract for treating acute respiratory tract infections. Cochrane Database of Systematic Reviews. 2013;(10):CD006323.
- Lissiman E, Bhasale AL, Cohen M. Garlic for the common cold. Cochrane Database of Systematic Reviews. 2014;(11):CD006206.
- Hatton RC, Winterstein AG, McKelvey RP, et al. Efficacy and safety of oral phenylephrine: systematic review and meta-analysis. Annals of Pharmacotherapy. 2007;41(3):381-390.
- De Sutter AIM, Saraswat A, van Driel ML. Antihistamines for the common cold. Cochrane Database of Systematic Reviews. 2015;(11):CD009345.
- Heikkinen T, Järvinen A. The common cold. The Lancet. 2003;361(9351):51-59.
- Eccles R. Understanding the symptoms of the common cold and influenza. The Lancet Infectious Diseases. 2005;5(11):718-725.
- Allan GM, Arroll B. Prevention and treatment of the common cold: making sense of the evidence. Canadian Medical Association Journal. 2014;186(3):190-199.
Research Papers
The links below run live searches on PubMed, the U.S. National Library of Medicine's database of biomedical literature. Use them to explore the latest peer-reviewed studies on the common cold, its remedies, and its prevention — each opens current results in a new tab.
- Common cold and rhinovirus
- Zinc lozenges for the common cold
- Vitamin C and cold duration
- Honey for cough in children
- Echinacea for the common cold
- Elderberry and respiratory infection
- Nasal saline irrigation
- Oral phenylephrine efficacy
- Sleep and infection susceptibility
- Hand hygiene and respiratory infection
- Pelargonium sidoides for infection
- Vitamin D and respiratory infections
Connections
- Influenza (the flu)
- Sinusitis
- Bronchitis
- Pneumonia
- Allergies
- Asthma
- Insomnia & sleep
- Vitamin C
- Zinc
- Echinacea
- Elderberry
- Garlic
- Ginger
- Honey
- Strep Throat
- Ear Infections
- RSV
- Measles
- Whooping Cough