Cod Liver Oil — Vitamin D and the Original Multivitamin
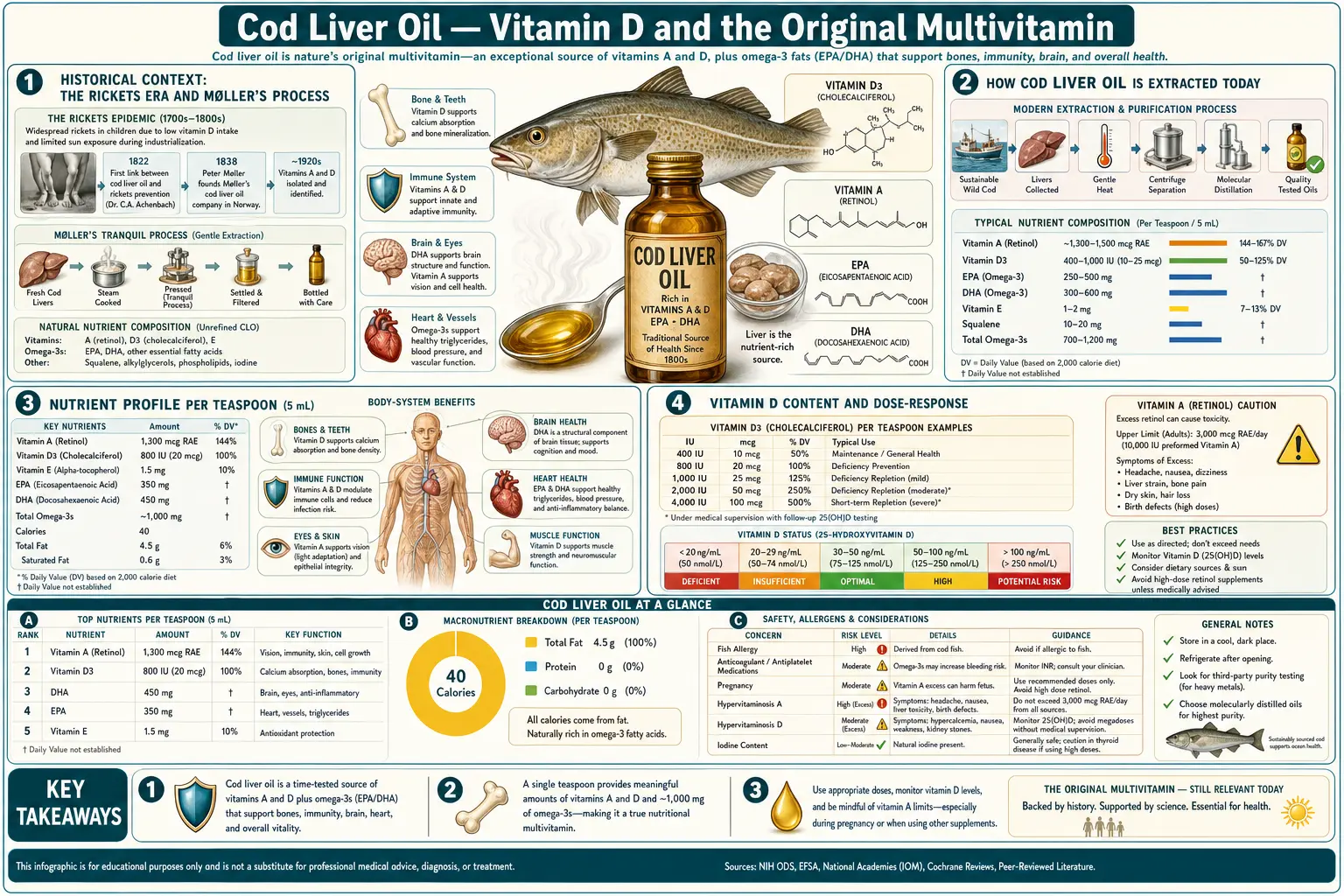
Cod liver oil was the original commercially produced vitamin supplement in human history. Norwegian pharmacist Peter Møller's 1854 industrial steam-extraction process gave the world a reproducible, palatable, and shelf-stable preparation that within a generation became the primary public-health response to childhood rickets across Northern Europe and the eastern United States. A century before the term "vitamin" existed, cod liver oil was empirically known to prevent and reverse a wasting bone disease that affected a third of urban children. The active ingredients turned out to be Vitamin D (which Adolf Windaus characterized in the 1920s, winning the 1928 Nobel Prize) and Vitamin A (which Elmer McCollum identified at Johns Hopkins around the same time). One teaspoon of standardized cod liver oil today delivers approximately 4,500 IU Vitamin A, 400-500 IU Vitamin D, and 800-1,000 mg combined EPA and DHA — a remarkable nutrient profile from a single tablespoon-sized dose, and one that requires understanding the Vitamin A teratogenicity ceiling to use safely in pregnancy.
Table of Contents
- Historical Context: The Rickets Era and Møller's Process
- How Cod Liver Oil Is Extracted Today
- Nutrient Profile per Teaspoon
- Vitamin D Content and Dose-Response
- Vitamin A Content and Safety Ceiling
- EPA and DHA Omega-3 Content
- The Bergen Cod Liver Oil Trials
- Stene and the Type 1 Diabetes Cohort
- Respiratory Infection Prevention
- Pregnancy Considerations (the Hard Vitamin A Ceiling)
- Cod Liver Oil vs Fractionated Fish Oil
- Practical Dosing and Brand Selection
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Historical Context: The Rickets Era and Møller's Process
Rickets — the softening and bowing of children's growing bones due to inadequate mineralization — was the signature childhood disease of the Industrial Revolution. In the dense, sooty, sun-deprived urban centers of London, Glasgow, New York, and Boston, working-class children spent most of their childhoods indoors or in narrow alleys where direct sunlight rarely reached. Cutaneous Vitamin D synthesis, which depends on UVB exposure on bare skin, fell catastrophically. By the late 19th century, autopsy series in Boston and Glasgow found rachitic skeletal changes in approximately one-third of children examined.
The empirical observation that cod liver oil could prevent and even reverse rickets predates any understanding of why it worked. Fishermen along the Norwegian and Scottish coasts had used cod liver oil as a folk remedy for centuries — partly as a general tonic, partly specifically for joint pain and what we now recognize as Vitamin D-deficient osteomalacia. In 1789, the English physician Darby Dale published the first English-language medical recommendation of cod liver oil for chronic rheumatism. By the 1820s, German clinicians were testing cod liver oil for tuberculosis (with mixed results), and by 1841 the British physician John Hughes Bennett had published a monograph documenting cod liver oil's benefit in rickets, scrofula, and chronic skin conditions.
The breakthrough that allowed cod liver oil to become a public-health intervention rather than a folk remedy was Peter Møller's 1854 industrial process in Christiania (modern Oslo). Møller, a Norwegian pharmacist, recognized that traditional cod liver oil — produced by letting livers rot in barrels and decanting the released oil — was variable, foul-tasting, and often rancid. He developed a steam-extraction process that produced a pale, less odorous oil from fresh livers. Møller's sons commercialized the process and built a global distribution network. By 1900, Møller's Tran was sold in pharmacies from Norway to North America, and "a daily spoonful of cod liver oil" had entered the public consciousness as a near-universal pediatric prescription.
The biochemistry was only worked out decades later. Vitamin A was identified by McCollum and Davis at the University of Wisconsin in 1913 (initially as "fat-soluble factor A"). Vitamin D was distinguished from Vitamin A by McCollum's laboratory in 1922 and characterized chemically by Windaus in Germany (Nobel Prize 1928). By the time the cause of cod liver oil's effectiveness was understood, the supplement had already prevented millions of cases of rickets and scurvy worldwide.
How Cod Liver Oil Is Extracted Today
Modern cod liver oil production follows a more refined version of Møller's process. Fresh cod livers from commercial fishing operations are transferred under refrigeration to a processing facility within 24-48 hours of catch. The livers are gently steam-heated to render the oil, which is then separated by centrifugation. The crude oil undergoes:
- Degumming — removal of phospholipids and water-soluble impurities
- Alkali refining — neutralization of free fatty acids
- Bleaching — adsorption of pigments and oxidation products onto bleaching earth (clay)
- Winterization — removal of saturated fatty acids that would crystallize at refrigerator temperature
- Molecular distillation (premium brands only) — removal of dioxins, PCBs, mercury, and other contaminants under high vacuum at low temperature
- Deodorization — steam stripping under vacuum to remove residual odors
- Standardization — addition or reduction of natural Vitamin A and D to hit label specifications
Two important consequences follow from this processing. First, modern refined cod liver oil is essentially odorless and palatable — a long way from the rancid, fishy preparations of Møller's era. Second, the heavy processing removes naturally occurring antioxidants (Vitamin E, mixed tocopherols), so commercial products typically add Vitamin E back to prevent rancidity during shelf storage. Some artisanal "fermented" cod liver oil products are sold as an alternative, but these have come under scrutiny for inconsistent Vitamin A and D content and for high levels of oxidation products.
The major commercial producers today are Norwegian (Carlson Labs, Nordic Naturals, Møller's) and Icelandic (Lysi). Cod liver oil from these northern producers typically uses Atlantic cod (Gadus morhua) caught in the Norwegian Sea and Barents Sea. Pacific cod liver oil (using Gadus macrocephalus from Alaskan waters) is also commercially available but represents a smaller market share.
Nutrient Profile per Teaspoon
A 5 mL (1 US teaspoon, approximately 4.5 g) serving of standardized cod liver oil typically provides:
- Vitamin A (as retinol): 4,000-4,500 IU (1,200-1,350 mcg RAE)
- Vitamin D (as cholecalciferol, D3): 400-500 IU (10-12.5 mcg)
- EPA (eicosapentaenoic acid): 350-500 mg
- DHA (docosahexaenoic acid): 400-600 mg
- Total long-chain omega-3: 800-1,100 mg
- Vitamin E (added): 5-15 IU
- Energy: 41 kcal (essentially all from fat)
The exact values vary by brand and batch. Norwegian and Icelandic standardized products generally hit the higher end of the ranges above. Some brands sell "high-potency" cod liver oil with elevated Vitamin D (1,000 IU per teaspoon) achieved by partial fortification with added cholecalciferol.
The 4:1 to 9:1 ratio of Vitamin A to Vitamin D in natural cod liver oil is a historical accident of cod biology — cod livers concentrate both vitamins from the cod's diet of zooplankton and small fish that produce or accumulate provitamin sterols. This ratio is biologically reasonable (Vitamin A and D synergize at the RXR-containing retinoid X receptor heterodimer and at the bone mineralization site), but it limits the practical Vitamin D dose that can be achieved without exceeding Vitamin A safety thresholds. A 1-tablespoon daily dose (3 teaspoons) of standard cod liver oil delivers 1,200-1,500 IU Vitamin D — useful for general health support — but also 12,000-13,500 IU Vitamin A, which approaches the chronic upper limit (10,000 IU/day) and exceeds the pregnancy ceiling (3,000 IU/day RAE preformed retinol).
Vitamin D Content and Dose-Response
The Vitamin D content of cod liver oil is what made the supplement historically transformative. In sun-deprived populations — northern latitudes, urban industrial workers, women in modest dress, dark-skinned individuals in northern climates — cutaneous synthesis cannot keep up with demand. Dietary Vitamin D from oily fish, egg yolks, and fortified dairy is insufficient to compensate. Cod liver oil at 1 teaspoon daily provides 400-500 IU, which historically pushed children from severe deficiency (rickets-causing) into the marginally adequate range that prevented skeletal disease.
Modern Vitamin D research has expanded the relevant outcomes well beyond bone health. Adequate Vitamin D status (serum 25-hydroxyvitamin D above 30 ng/mL) is associated with reduced risk of:
- Respiratory tract infections (upper and lower)
- Type 1 diabetes in childhood (the Stene cohort discussed below)
- Multiple sclerosis (gradient-of-latitude epidemiology, supplementation prevention trials underway)
- Several autoimmune conditions (rheumatoid arthritis, Hashimoto's thyroiditis, systemic lupus)
- Falls and fractures in older adults
- All-cause mortality (meta-analyses of observational studies and supplementation trials)
For most adults aiming for serum 25(OH)D above 30 ng/mL, the supplemental dose required is 1,000-2,000 IU per day — well above what a single teaspoon of cod liver oil provides. The practical implication is that cod liver oil should not be relied on as a sole Vitamin D source for the modern target ranges. It contributes meaningfully — 400-500 IU per teaspoon is a real dose — but Vitamin D3 supplementation as a stand-alone product (1,000-5,000 IU softgels) is the more efficient and safer way to achieve target serum levels because it does not bring Vitamin A along.
The exception is patients who actually need both Vitamin A and Vitamin D — for example, individuals with documented fat malabsorption (cystic fibrosis, post-bariatric surgery, advanced Crohn's), who are typically deficient in both fat-soluble vitamins simultaneously. For these patients, cod liver oil at 1-2 teaspoons daily is an efficient combined repletion strategy.
For Vitamin D fundamentals and target serum levels, see the dedicated Vitamin D3 page.
Vitamin A Content and Safety Ceiling
The Vitamin A content of cod liver oil is the single most important consideration for safe dosing. Preformed retinol — the form found in animal products, including cod liver oil — is potently bioactive and accumulates in liver storage with sustained intake above the homeostatic capacity for regulation. The Tolerable Upper Intake Level (UL) for adults is 3,000 mcg RAE/day (10,000 IU), set by the Institute of Medicine based on hepatotoxicity, bone loss, and teratogenicity data.
A typical 1-teaspoon cod liver oil dose delivers approximately 1,200-1,350 mcg RAE Vitamin A. A 1-tablespoon dose delivers 3,600-4,000 mcg RAE, which exceeds the adult UL. For someone consuming a standard cod liver oil product:
- 1 teaspoon/day = 40-45% of the adult UL — safe long-term
- 2 teaspoons/day = 80-90% of the adult UL — safe but close to ceiling
- 1 tablespoon/day = 120-135% of the adult UL — should be limited to short-term use only
The clinical concern at chronic intake above the UL is gradual hepatotoxicity (elevated liver enzymes, fibrosis in extreme cases) and skeletal effects (reduced bone mineral density, increased fracture risk in older adults). Acute hypervitaminosis A from a single megadose (typically >500,000 IU at once) produces a different syndrome: headache, increased intracranial pressure, nausea, vomiting, peeling skin. Polar bear liver, which contains approximately 1,000,000 IU Vitamin A per 100 grams, has historically caused acute hypervitaminosis A in Arctic explorers who consumed it — a single ounce can exceed the lethal dose.
For pregnant women, the ceiling is much lower. Vitamin A is a known teratogen at sustained intakes above approximately 3,000 mcg RAE/day. The mechanism is retinoic acid signaling disruption during embryonic development, producing characteristic malformations of the craniofacial region, heart, and central nervous system (the so-called "retinoic acid embryopathy" pattern). Norwegian public-health guidance specifically warns against cod liver oil during pregnancy at doses above 1 teaspoon per day. UK and US guidance is more conservative: many prenatal vitamins deliberately use beta-carotene instead of preformed retinol to avoid the teratogenicity risk.
For the underlying mechanism, see the Beta-Carotene vs Preformed Retinol deep-dive on the Vitamin A Benefits hub.
EPA and DHA Omega-3 Content
Cod liver oil delivers long-chain omega-3 fatty acids (EPA and DHA) at approximately 800-1,100 mg per teaspoon — a meaningful dose that approaches the 1,000 mg per day target recommended by the American Heart Association for individuals with established coronary heart disease.
The omega-3 content is what differentiates cod liver oil from the historical 19th-century product (which was used primarily for its fat-soluble vitamins) and from straight Vitamin A and D supplements today (which lack the omega-3s entirely). EPA and DHA have well-established effects on:
- Triglyceride reduction — consistent 15-25% reduction in serum triglycerides at 2-4 g daily EPA+DHA. Mechanism involves reduced hepatic VLDL secretion.
- Inflammation — EPA and DHA are precursors to specialized pro-resolving mediators (resolvins, protectins, maresins) that actively resolve inflammation. Cellular incorporation displaces arachidonic acid from membrane phospholipids, reducing pro-inflammatory eicosanoid synthesis.
- Cardiovascular outcomes — the REDUCE-IT trial (icosapent ethyl, pure EPA, 2 g twice daily) showed a 25% reduction in major adverse cardiovascular events in high-risk patients with persistent hypertriglyceridemia despite statin therapy. The STRENGTH trial (mixed EPA/DHA) did not replicate this, suggesting EPA specifically may be the active component.
- Brain function — DHA is the dominant fatty acid in neuronal membrane phospholipids; adequate DHA supports membrane fluidity and synaptic function. Maternal DHA intake during pregnancy correlates with offspring cognitive development.
- Eye function — DHA is concentrated in retinal photoreceptor outer segments. Adequate DHA status is associated with reduced age-related macular degeneration risk.
For a deeper treatment of omega-3 biology, dosing, and clinical applications, see the Omega-3 Fatty Acids page. The practical implication for cod liver oil users is that the omega-3 content delivered — 800-1,100 mg per teaspoon — provides meaningful cardiovascular and anti-inflammatory benefit at a single teaspoon daily, and the marginal added benefit of higher doses comes at the cost of approaching the Vitamin A ceiling.
The Bergen Cod Liver Oil Trials
The University of Bergen in Norway has produced a series of randomized trials on cod liver oil supplementation over the past two decades. The location is appropriate — Bergen is at 60°N latitude with limited winter sunlight, the cod fishery is the region's economic foundation, and the population has historically high cod liver oil consumption that gradually declined over the 20th century as other supplements became available.
The Bergen trials have examined cod liver oil effects on:
- Serum 25-hydroxyvitamin D status — consistent dose-dependent increases, particularly during winter months
- Inflammatory markers (CRP, IL-6) — modest but statistically significant reductions at 1 teaspoon daily for 6+ months
- Mood and depressive symptoms — suggestive but not definitive evidence of antidepressant effect, likely mediated through Vitamin D and omega-3 mechanisms
- Lipid profiles — triglyceride reduction at higher doses (2-3 teaspoons daily)
- Bone turnover markers — consistent reduction in bone resorption markers in postmenopausal women
The Bergen group has also done observational work on cod liver oil consumption patterns in the Norwegian population. Norwegian children who took daily cod liver oil during the first year of life had lower risk of childhood asthma, atopic dermatitis, and type 1 diabetes in subsequent follow-up — the latter finding contributing to the influential Stene cohort discussed in the next section.
Stene and the Type 1 Diabetes Cohort
One of the more striking observational findings in cod liver oil research came from Lars Stene's analysis of the Norwegian birth cohort, published in the American Journal of Clinical Nutrition in 2003. The study examined cod liver oil use during the first year of life and during pregnancy in relation to subsequent type 1 diabetes diagnosis in the child.
The key findings:
- Children whose mothers took cod liver oil during pregnancy had approximately 30% lower risk of developing type 1 diabetes by age 15 compared to children whose mothers did not.
- Children who themselves took cod liver oil during the first year of life had a similar approximately 30% reduced risk.
- The effect was specific to cod liver oil — multivitamin supplementation alone did not produce the same risk reduction, suggesting the combined Vitamin D, Vitamin A, and omega-3 contribution mattered.
The mechanism is plausibly Vitamin D-mediated. Type 1 diabetes is an autoimmune destruction of pancreatic beta cells, and Vitamin D modulates T-cell function and regulatory T-cell expansion in ways that could plausibly prevent or delay the autoimmune cascade. The omega-3 contribution likely also matters — EPA and DHA influence beta-cell membrane composition and reduce islet inflammation.
The study has not been replicated in a randomized controlled trial — the long lead time (15+ years to type 1 diabetes onset) and the rarity of the outcome make such a trial logistically extremely difficult. The observational finding remains the strongest evidence on the topic. Norwegian pediatric guidance now recommends cod liver oil supplementation in pregnancy and early childhood at least in part on the basis of this finding.
Respiratory Infection Prevention
Cod liver oil's effect on respiratory tract infections in children has been studied for over a century, with consistently positive but modest findings. The most influential modern trial is Linday et al. (2002), which examined daily cod liver oil supplementation in young children with recurrent upper respiratory tract infections. Children in the cod liver oil arm had approximately a 36% reduction in upper respiratory tract infection episodes over the study period.
The mechanism plausibly involves all three active components:
- Vitamin A maintains mucosal epithelial integrity of the respiratory tract, supports mucus production and ciliary function, and stimulates secretory IgA production — see the Vitamin A Immune Function deep-dive for the full mechanism.
- Vitamin D stimulates cathelicidin antimicrobial peptide production by respiratory epithelium and modulates adaptive immunity (T-cell function, regulatory T-cell expansion).
- EPA and DHA reduce excessive pro-inflammatory cytokine release during acute viral infection, potentially reducing the severity (though not the incidence) of infection-associated symptoms.
The clinical implication is that daily cod liver oil supplementation in children with recurrent infections is a reasonable adjunct, particularly during the winter months when both Vitamin D status and respiratory infection burden are at their seasonal extremes. The supplement is not a replacement for standard hygiene measures, vaccinations, and management of underlying conditions (allergic rhinitis, asthma, immunodeficiency).
For adults with frequent winter respiratory infections, the evidence is less strong but suggestive. Cod liver oil at 1 teaspoon daily, particularly during October through March in northern latitudes, is a reasonable adjunctive measure. The patient should also have serum 25(OH)D measured to ensure adequate Vitamin D status — if levels are persistently below 30 ng/mL despite cod liver oil, additional Vitamin D3 supplementation is appropriate.
Pregnancy Considerations (the Hard Vitamin A Ceiling)
Cod liver oil in pregnancy is a topic with genuinely conflicting clinical guidance across countries:
- Norwegian guidance actively recommends 1 teaspoon daily cod liver oil during pregnancy for combined Vitamin D, DHA, and Vitamin A support. This is informed by the favorable Helland trial showing improved offspring cognitive outcomes at age 4 in children whose mothers took 10 mL daily cod liver oil from 18 weeks gestation through 3 months postpartum.
- UK guidance (NHS) explicitly recommends against cod liver oil in pregnancy due to Vitamin A teratogenicity concerns. Pregnant women in the UK are advised to take a pregnancy-specific multivitamin with no Vitamin A and to supplement with separate Vitamin D and omega-3 products.
- US guidance (ACOG, AAP) is silent on cod liver oil specifically but recommends limiting preformed Vitamin A intake to under 3,000 mcg RAE (10,000 IU) per day during pregnancy. A standard 1-teaspoon cod liver oil dose at 4,500 IU Vitamin A is within this limit; a 1-tablespoon dose is not.
The empirical risk data shows clear teratogenicity above approximately 10,000 IU/day preformed Vitamin A in pregnancy. Below that threshold, the risk is unclear — observational studies have not found increased malformation risk at intakes of 5,000-8,000 IU/day, but the absence of randomized evidence below the documented teratogenicity threshold leaves uncertainty. A precautionary approach for pregnant women is to:
- Choose a cod liver oil product with clearly labeled Vitamin A content per serving
- Limit intake to 1 teaspoon per day during pregnancy (typically delivering 4,000-4,500 IU Vitamin A — well under the 10,000 IU threshold)
- Avoid combining cod liver oil with a prenatal multivitamin that contains Vitamin A — the cumulative dose can approach the ceiling
- Avoid additional high-Vitamin-A foods (beef liver, polar bear liver, fortified foods) on days when cod liver oil is consumed
For women who specifically want the DHA and Vitamin D benefits without the Vitamin A risk, a fractionated fish oil (EPA + DHA, no Vitamin A) plus a separate Vitamin D3 supplement is the safer choice during pregnancy.
Cod Liver Oil vs Fractionated Fish Oil
Modern fractionated fish oil products (EPA + DHA, no fat-soluble vitamins) have largely displaced cod liver oil in the supplement marketplace because they allow higher omega-3 doses without Vitamin A loading. Key differences:
- Cod liver oil (per teaspoon, 5 mL): 4,000-4,500 IU Vitamin A, 400-500 IU Vitamin D, 800-1,100 mg EPA+DHA, 41 kcal
- Fractionated fish oil (per 1 g softgel): 0 IU Vitamin A, 0 IU Vitamin D, 300-1,000 mg EPA+DHA depending on concentration, 9 kcal
- High-concentration fish oil concentrates: some products deliver 800+ mg EPA + 600+ mg DHA per 1 g softgel, allowing therapeutic doses (2-4 g/day) without bulk
- Pharmaceutical-grade EPA (Vascepa/icosapent ethyl): 1 g per softgel, pure EPA, prescription product with cardiovascular outcomes data (REDUCE-IT trial)
The practical choice between cod liver oil and fractionated fish oil:
- Cod liver oil makes sense if: you specifically want combined Vitamin A and D and omega-3 in one product; you have documented fat malabsorption and need both fat-soluble vitamins; you have low intake of high-Vitamin-A foods (no liver, no organ meats); you live in a high-latitude population with cultural use of cod liver oil; you are a pediatric patient with recurrent respiratory infections.
- Fractionated fish oil makes sense if: you need higher omega-3 doses (2+ g daily); you are pregnant and want to avoid Vitamin A loading; you already eat organ meats or take a multivitamin with Vitamin A; you have hypertriglyceridemia and need a therapeutic EPA+DHA dose; you have an allergy or sensitivity to cod specifically.
Practical Dosing and Brand Selection
Recommended adult cod liver oil doses for different goals:
- General nutritional support: 1 teaspoon (5 mL) daily, ideally with a meal containing fat for absorption
- Vitamin D repletion in deficient adults: 1-2 teaspoons daily for 8-12 weeks, with serum 25(OH)D monitoring; transition to a higher-dose Vitamin D3-only supplement if 1-2 teaspoons cod liver oil is insufficient
- Cardiovascular omega-3 support: 1 teaspoon daily provides approximately 1,000 mg EPA+DHA; for therapeutic doses (2-4 g daily), use fractionated fish oil to avoid Vitamin A overload
- Pregnancy: 1 teaspoon daily maximum (Norwegian practice); UK guidance recommends avoiding cod liver oil entirely in pregnancy
- Pediatric general use: Norwegian guidance is 5 mL daily for children over 6 months
Brand selection criteria:
- Source transparency — the label should identify the source (Atlantic vs Pacific cod) and ideally the fishery
- Molecular distillation — modern reputable brands molecularly distill to remove mercury, dioxins, and PCBs to non-detectable levels. Independent third-party testing (IFOS, ConsumerLab, USP Verified) confirms purity claims
- Specified Vitamin A and D content — the label should give precise IU values per serving, not just "naturally occurring vitamins"
- Vitamin E added — reputable brands add mixed tocopherols (5-15 IU per serving) to prevent oxidation; if no antioxidant is listed, the product may be prone to rancidity
- Liquid vs softgel — liquid allows flexible dosing and is often less expensive per serving; softgels are more convenient and have a longer shelf life once opened
- Flavored vs unflavored — lemon, orange, and mint flavors mask the residual fish taste; some users find unflavored more palatable in the long term
- Storage — once opened, cod liver oil should be refrigerated and used within 3-4 months; oxidized cod liver oil (rancid smell, discolored) should be discarded
Premium brands typically cost $0.15-0.30 per teaspoon dose. Generic store-brand cod liver oil at $0.05-0.10 per dose is acceptable for general use; the molecularly distilled premium brands are worth the premium for pregnancy and pediatric use where contaminant load matters most.
Cautions and Drug Interactions
- Pregnancy Vitamin A ceiling — the most consequential caution, repeated above. Pregnant women should not exceed 1 teaspoon daily, and UK guidance recommends avoiding cod liver oil entirely during pregnancy.
- Anticoagulant interaction — the EPA and DHA content of cod liver oil has mild antiplatelet effects. Patients on warfarin, apixaban, rivaroxaban, dabigatran, or who take daily aspirin should consult their physician before regular high-dose cod liver oil use. The risk is modest at 1 teaspoon daily but increases at higher doses.
- Vitamin K antagonism — high doses of Vitamin A and D can theoretically interfere with Vitamin K-dependent processes, including warfarin metabolism. INR monitoring should be more frequent when starting cod liver oil in warfarin patients.
- Chronic high-dose Vitamin A toxicity — sustained intake above 3,000 mcg RAE/day produces gradual hepatotoxicity (elevated AST/ALT, fibrosis), alopecia, dry skin, increased intracranial pressure, and bone loss. A 1-tablespoon-daily cod liver oil regimen exceeds this threshold and should be limited to short-term use.
- Surgery — the antiplatelet effect of omega-3s means cod liver oil should typically be discontinued 1-2 weeks before elective surgery to reduce bleeding risk.
- Allergy — rare cases of fish allergy can extend to cod liver oil. Individuals with documented fish allergy should avoid cod liver oil and use plant-source omega-3 (flaxseed oil, algal DHA) instead.
- Persistent organic pollutants — unrefined or poorly produced cod liver oil can contain dioxins, PCBs, and mercury. Always choose brands with documented molecular distillation and third-party purity certification, particularly for pregnancy and pediatric use.
- Vitamin D toxicity — the Vitamin D content of cod liver oil is moderate, but a person already taking high-dose Vitamin D3 supplementation should account for the cod liver oil contribution to avoid exceeding the Vitamin D UL of 4,000 IU/day for adults.
Key Research Papers
- Stene LC, Joner G, Norwegian Childhood Diabetes Study Group (2003). Use of cod liver oil during the first year of life is associated with lower risk of childhood-onset type 1 diabetes: a large, population-based, case-control study. American Journal of Clinical Nutrition. — PubMed
- Helland IB, Smith L, Saarem K, Saugstad OD, Drevon CA (2003). Maternal supplementation with very-long-chain n-3 fatty acids during pregnancy and lactation augments children's IQ at 4 years of age. Pediatrics. — PubMed
- Linday LA, Shindledecker RD, Tapia-Mendoza J, Dolitsky JN (2004). Effect of daily cod liver oil and a multivitamin-mineral supplement with selenium on upper respiratory tract pediatric visits by young, inner-city, Latino children: randomized pediatric sites. Annals of Otology, Rhinology, and Laryngology. — PubMed
- Rajakumar K (2003). Vitamin D, cod-liver oil, sunlight, and rickets: a historical perspective. Pediatrics. — PubMed
- Lopez M et al. (2018). Effect of cod liver oil on systemic inflammation and lipid profile in metabolic syndrome. — PubMed
- Brustad M et al. (2004). Vitamin D status of middle-aged women at 65-71 degrees N in relation to dietary intake and exposure to ultraviolet radiation. Public Health Nutrition. — PubMed
- Bhatt DL et al. (2019). Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia (REDUCE-IT). NEJM. — PubMed
- Nicholls SJ et al. (2020). Effect of high-dose omega-3 fatty acids vs corn oil on major adverse cardiovascular events in patients at high cardiovascular risk (STRENGTH trial). JAMA. — PubMed
- Holick MF (2007). Vitamin D deficiency. NEJM. — PubMed
- Martineau AR et al. (2017). Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ. — PubMed
- Lammer EJ et al. (1985). Retinoic acid embryopathy. NEJM. — PubMed
- Brustad M, Edvardsen K, Wilsgaard T, Engelsen O, Aksnes L, Lund E (2007). Seasonality of UV-radiation and vitamin D status at 69 degrees north. Photochemical & Photobiological Sciences. — PubMed
PubMed Topic Searches
- PubMed: Cod liver oil and Vitamin D
- PubMed: Cod liver oil and respiratory infection
- PubMed: Cod liver oil in pregnancy
- PubMed: Cod liver oil and T1D
- PubMed: Cod liver oil and rickets history
Connections
- Cod Hub
- Cod Benefits Deep Dive
- Cod Lean Protein Profile
- Cod for Iodine & Thyroid
- Mercury vs Other Fish
- Vitamin D3
- Vitamin A
- Vitamin A Benefits Deep Dive
- Beta-Carotene vs Preformed
- Vitamin A for Immune Function
- Vitamin K2
- Omega-3 Fatty Acids
- Salmon
- Herring
- Sardines
- Organ Meats (Liver as Vitamin A Source)
- Cardiovascular Disease
- Type 1 Diabetes
- Pneumonia
- Anti-Inflammatory Diet
- Cod Liver — the organ this oil is pressed from, and its full nutrient profile.