Cod for Iodine and Thyroid Function
A single 100-gram cod fillet delivers approximately 100 micrograms of iodine — roughly 67% of the adult RDA of 150 mcg/day — and approximately 33 micrograms of selenium (60% of the adult RDA). These two trace minerals are both required for thyroid hormone production and conversion: iodine is incorporated directly into the thyroid hormones thyroxine (T4, four iodine atoms) and triiodothyronine (T3, three iodine atoms), and selenium is the essential cofactor for the deiodinase enzymes that convert the relatively inactive T4 into the metabolically active T3. Among commonly available foods, only seaweed (kelp, dulse, nori) delivers more iodine, and most Westerners eat little seaweed. Combined with the rising prevalence of mild iodine deficiency in industrialized countries that have moved away from iodized salt (UK, parts of Europe, increasingly the United States), the iodine and selenium content of cod has clinical relevance for hypothyroidism, Hashimoto's thyroiditis, pregnancy, and the broader question of whether modern dietary patterns are quietly producing subclinical thyroid dysfunction.
Table of Contents
- Thyroid Anatomy and Iodine Biochemistry
- Iodine Content of Cod and Other Foods
- Selenium and the Deiodinase Enzymes
- RDA, Deficiency, and the Iodine Status Map
- Hypothyroidism and Iodine Repletion
- Hashimoto's Thyroiditis (the Selenium Paradox)
- Pregnancy Iodine Requirements
- Pediatric Iodine and IQ
- Cretinism and the WHO Salt Iodization Program
- Iodine Prophylaxis After Nuclear Accidents
- Iodine Excess and Thyroid Risks
- Practical Cod Consumption for Thyroid Support
- Key Research Papers
- Connections
- Featured Videos
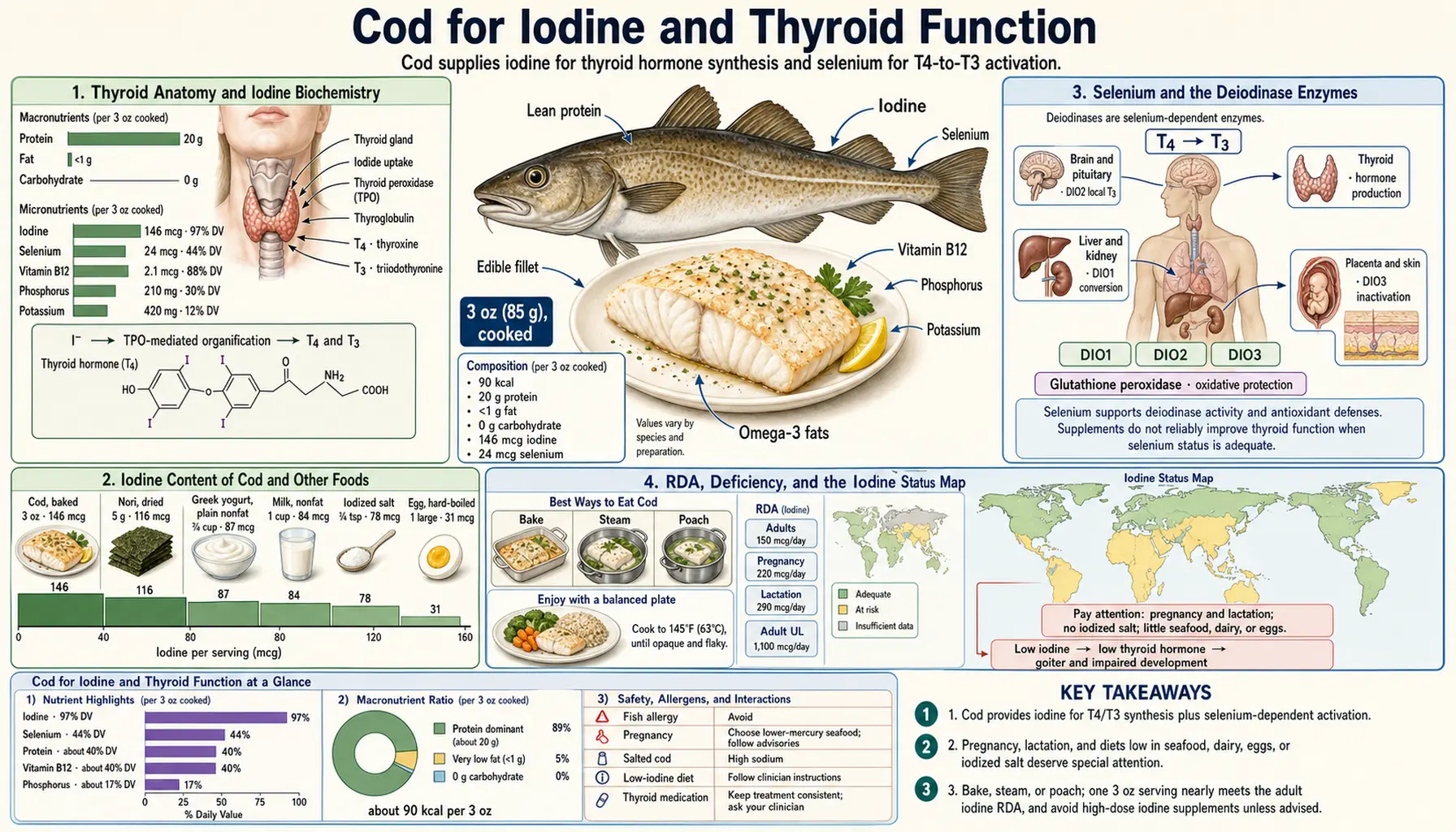
Thyroid Anatomy and Iodine Biochemistry
The thyroid gland sits in the front of the neck wrapped around the trachea, weighs about 25-30 grams in healthy adults, and contains approximately 70-80% of the body's total iodine pool. The gland actively concentrates iodide from the bloodstream against a steep concentration gradient using the sodium-iodide symporter (NIS), achieving intracellular iodide concentrations 20-40 times higher than serum.
Inside thyroid follicular cells, iodide is oxidized by thyroid peroxidase (TPO) and incorporated into tyrosine residues on thyroglobulin (Tg), a large glycoprotein scaffold. The iodinated tyrosines couple to form thyroxine (T4, containing 4 iodine atoms) and triiodothyronine (T3, containing 3 iodine atoms). Thyroglobulin with attached T4 and T3 is stored in the colloid-filled follicles until needed; on TSH stimulation, the gland endocytoses the colloid, proteolytically releases T4 and T3, and secretes them into the bloodstream.
The molecular weight of T4 is approximately 65% iodine. Producing one molecule of T4 requires four iodine atoms (atomic weight 127 each, total 508 daltons) attached to the tyrosine backbone (181 daltons). For an adult thyroid producing approximately 85 mcg of T4 daily, the iodine throughput is approximately 60 mcg per day — the absolute minimum dietary iodine requirement to maintain thyroid hormone synthesis. The RDA of 150 mcg/day provides a safety margin for variable intake, urinary losses, and gestational/lactational increases.
The thyroid's iodine pool turns over slowly — total body iodine is approximately 15-20 mg, and daily turnover is 60-80 mcg, giving a half-life of approximately 100 days. This buffer means that brief periods of iodine deficiency (a week or two) do not immediately produce hypothyroidism — the gland draws on stored iodine. Sustained deficiency over months to years gradually depletes the stores and progresses through goiter formation, hypothyroidism, and (in pregnancy or early childhood) neurodevelopmental damage.
Iodine Content of Cod and Other Foods
Why do ocean fish like cod contain so much iodine? The answer is biogeochemistry. Seawater contains approximately 50-60 mcg iodide per liter — one of the few iodine-rich natural reservoirs on Earth. Marine fish concentrate iodine from seawater through their gills and from the iodine-rich plankton and smaller fish they consume. White ocean fish like cod sequester much of this iodine in muscle and liver tissue, where it is bioavailable to consumers who eat the fish.
Approximate iodine content of common foods (mcg per typical serving):
- Kelp (kombu, dried, 1 g): 2,000-3,000 mcg (highly variable; can cause iodine excess)
- Wakame seaweed (dried, 1 g): 100-200 mcg
- Nori seaweed (1 sheet, ~2 g): 30-50 mcg
- Iodized salt (1 tsp, US standard, 5 g): 380 mcg
- Cod (cooked, 100 g): ~100 mcg (range 80-150)
- Yogurt (plain, 1 cup, 245 g): 75 mcg
- Milk (1 cup, 240 mL): 56 mcg
- Shrimp (cooked, 85 g): 35 mcg
- Egg (1 large): 24 mcg
- Tuna (canned, 85 g): 17 mcg
- Salmon (cooked, 100 g): 10-20 mcg
- Beef (100 g): 3 mcg
- Chicken (100 g): 7 mcg
- Bread (1 slice, US): 5-10 mcg (variable; depends on iodate dough conditioners)
- Apple, banana, leafy greens: <5 mcg
The numbers show two important facts. First, cod is genuinely an iodine standout among non-seaweed foods — a single 100 g serving provides more iodine than 4-5 eggs or 10 slices of bread or a half-pound of beef combined. Second, iodized salt and dairy are the two largest contributors to iodine intake in most Western diets — populations that avoid iodized salt (specialty salts, sodium-restricted diets, processed-food diets that use non-iodized salt) and avoid dairy (lactose intolerance, vegan diets) can easily fall below the 150 mcg/day RDA without realizing it.
A 6-ounce (170 g) cod fillet at dinner delivers approximately 170 mcg iodine — more than the full adult RDA in a single meal. Two cod meals per week therefore reliably push weekly average intake into the adequate range, even for individuals who otherwise have low iodine consumption.
Selenium and the Deiodinase Enzymes
Thyroid hormone biology has a two-step structure that requires two different trace minerals. The thyroid gland produces predominantly T4 (the four-iodine form), which is relatively biologically inactive. T4 must be converted to T3 (the three-iodine form) by removal of a single iodine atom from the outer ring — this is the metabolically active form that binds nuclear thyroid hormone receptors. The deiodinase enzymes that perform this conversion all contain selenocysteine at their active sites, making selenium an absolute cofactor for T4-to-T3 conversion.
Three deiodinase isoforms exist, each with distinct tissue distribution and function:
- Type 1 deiodinase (DIO1) — expressed in liver, kidney, and thyroid; primary source of circulating T3
- Type 2 deiodinase (DIO2) — expressed in brain, pituitary, brown adipose tissue, skeletal muscle; provides local T3 to those tissues
- Type 3 deiodinase (DIO3) — expressed in placenta, brain, skin; inactivates T4 and T3 by inner-ring deiodination
Selenium deficiency reduces DIO1 and DIO2 activity, producing a syndrome where serum T4 is normal or elevated but tissue T3 is low — functional hypothyroidism with apparently normal lab values on simple TSH and T4 testing. A free T3 measurement reveals the deficiency. The combination of iodine deficiency and selenium deficiency, common in some inland Chinese provinces and central African countries, produces particularly severe thyroid dysfunction including endemic goiter and high rates of congenital hypothyroidism.
Cod contains both required minerals. Selenium content in a 100-gram cooked cod fillet is approximately 33 mcg (60% of the adult RDA of 55 mcg/day). The cod selenium is predominantly in the form of selenocysteine and selenomethionine, both highly bioavailable. A single 6-ounce cod meal provides approximately 56 mcg selenium — the full adult RDA — alongside 170 mcg iodine.
This combination is uncommon in foods. Brazil nuts are higher in selenium per unit weight but have negligible iodine. Kelp is higher in iodine but has very little selenium. Cod is the rare food that hits both targets simultaneously, which is one reason traditional cod-eating populations (Norwegians, Icelanders, coastal Japanese, Newfoundland fishing communities) have historically had low rates of hypothyroidism despite cold climates and limited dietary diversity.
For deeper treatment of these minerals individually, see Iodine and Selenium.
RDA, Deficiency, and the Iodine Status Map
The Institute of Medicine RDA for iodine:
- Adults (men and non-pregnant women): 150 mcg/day
- Pregnant women: 220 mcg/day
- Lactating women: 290 mcg/day
- Children 1-8 years: 90 mcg/day
- Children 9-13 years: 120 mcg/day
- Tolerable Upper Intake Level (UL): 1,100 mcg/day for adults
Iodine deficiency is classified by WHO into severity tiers based on urinary iodine concentration (UIC) in school-age children, a population-level indicator:
- Severe deficiency: UIC <20 mcg/L — associated with cretinism, endemic goiter, intellectual disability
- Moderate deficiency: UIC 20-49 mcg/L — goiter, hypothyroidism, mild cognitive deficits
- Mild deficiency: UIC 50-99 mcg/L — subclinical hypothyroidism, mild IQ deficits
- Adequate: UIC 100-199 mcg/L — the target range
- Above requirements: UIC 200-299 mcg/L — usually no clinical concern, sometimes seen in high-seaweed populations
- Excess: UIC >300 mcg/L — risk of iodine-induced hyperthyroidism in susceptible individuals
Global iodine status has improved dramatically since the WHO and UNICEF launched the Universal Salt Iodization (USI) program in 1990. The number of severely iodine-deficient countries fell from 113 in 1993 to 25 in 2017. But the improvement is not universal:
- The UK has slipped from "adequate" in the mid-20th century to "mild deficiency" in surveys from 2008-2017, driven by reduced iodized salt and dairy consumption among teenage girls
- Several European countries (Germany, France, Italy) have intermittent mild deficiency depending on regional salt-iodization practice
- The United States is currently borderline-adequate population-wide, but pregnant women specifically have median UIC around 125 mcg/L — just below the WHO-recommended 150-249 mcg/L range for pregnancy
- Vegan populations and individuals avoiding iodized salt are at increased risk regardless of country of residence
The clinical implication is that mild iodine deficiency is common in industrialized countries despite the success of salt iodization programs, and individuals with low dairy and salt intake should consider their dietary iodine sources deliberately. Regular cod (or other ocean fish) consumption is one of the most efficient remedies.
Hypothyroidism and Iodine Repletion
Frank iodine-deficiency hypothyroidism is rare in industrialized countries but common in iodine-deficient regions of the developing world. Subclinical hypothyroidism with mild iodine deficiency is more common everywhere — characterized by mildly elevated TSH (4-10 mIU/L), normal or low-normal free T4, and symptoms of fatigue, weight gain, cold intolerance, dry skin, and constipation.
For an iodine-deficient patient with subclinical or overt hypothyroidism, iodine repletion alone can fully reverse the condition if no autoimmune thyroid disease is also present. Repletion strategies:
- Iodized salt — the most cost-effective public-health intervention; approximately 380 mcg iodine per teaspoon of US iodized salt
- Dietary iodine sources — dairy, eggs, ocean fish (cod, haddock, pollock), small amounts of seaweed
- Iodine supplements — potassium iodide tablets at 150 mcg (matching the RDA); typically used during pregnancy or in patients with verified deficiency
- Cod liver oil — not a meaningful iodine source despite the "cod" in the name (Vitamin A and D, omega-3s, but not significant iodine; the iodine is in the muscle tissue, not the liver)
The critical caveat is that not all hypothyroidism is iodine-deficiency hypothyroidism. In industrialized countries, the dominant cause of acquired hypothyroidism is Hashimoto's thyroiditis — autoimmune destruction of the thyroid gland. In Hashimoto's, iodine supplementation can paradoxically worsen the autoimmune process (discussed in the next section), so iodine repletion should not be reflexively applied without first ruling out autoimmune disease via TPO antibody testing.
For patients with documented iodine deficiency and hypothyroidism but no autoimmune markers, the typical clinical course of repletion is:
- Restore dietary iodine to 150-250 mcg/day through diet and/or supplementation
- Monitor TSH and free T4 at 6-12 week intervals
- Expect TSH normalization within 3-6 months as thyroid hormone production recovers
- Continue adequate iodine intake long-term to prevent recurrence
For severely deficient patients with longstanding goiter, the gland may not fully recover even after iodine repletion — some patients require lifelong levothyroxine despite restored iodine status.
Hashimoto's Thyroiditis (the Selenium Paradox)
Hashimoto's thyroiditis is the leading cause of acquired hypothyroidism in iodine-replete countries. The disease is an autoimmune destruction of the thyroid gland, characterized by lymphocytic infiltration and the presence of anti-thyroid peroxidase (anti-TPO) and anti-thyroglobulin (anti-Tg) antibodies in serum. Over years to decades, the gradual destruction of thyroid tissue produces progressive hypothyroidism requiring levothyroxine replacement.
The iodine relationship in Hashimoto's is paradoxical and counterintuitive. In iodine-replete populations, supplemental iodine above approximately 300-400 mcg/day can accelerate the autoimmune process by increasing the iodination of thyroglobulin, generating more antigenic targets for the existing immune response. Some patients with Hashimoto's experience rapid worsening of antibody titers and hypothyroidism when they start kelp supplements or high-dose iodine drops.
This does not mean Hashimoto's patients should avoid dietary iodine entirely — they still need 150 mcg/day for normal thyroid function. The practical guidance is to:
- Obtain iodine from food sources (cod, dairy, eggs) rather than concentrated supplements
- Avoid kelp tablets, high-dose iodine drops, and other supraphysiologic iodine sources
- Limit seaweed consumption to small amounts (a single sheet of nori, a serving of wakame in miso soup) rather than daily kombu broth
- Maintain adequate selenium intake — this is where the paradox resolves
The selenium connection is one of the more clinically useful findings in modern thyroid nutrition. Selenium supplementation at 200 mcg/day has been shown in multiple randomized trials to reduce anti-TPO antibody titers in Hashimoto's patients by approximately 30-40%. The mechanism involves selenium's role in glutathione peroxidase activity within the thyroid — the enzyme uses selenium to detoxify hydrogen peroxide generated during normal thyroid hormone synthesis. With adequate selenium, the hydrogen peroxide is efficiently cleared; with selenium deficiency, residual hydrogen peroxide damages thyroid follicular cells and exacerbates the autoimmune response.
The 2013 van Zuuren Cochrane review concluded that the evidence supports selenium supplementation for reducing antibody titers in Hashimoto's but is insufficient to recommend it for clinical thyroid function or symptoms. Some endocrinologists routinely add 200 mcg/day selenium to Hashimoto's management; others wait for stronger evidence.
For cod consumption specifically: regular cod intake delivers both the dietary iodine needed for thyroid function and the selenium that supports the antioxidant defenses against autoimmune damage. This makes cod a reasonable food choice for Hashimoto's patients — the iodine dose per serving (~100-170 mcg) is within the safe range and does not approach the autoimmune-trigger threshold. Patients should still avoid high-dose iodine supplements and excess seaweed.
For deeper coverage, see the Hashimoto's Thyroiditis page.
Pregnancy Iodine Requirements
Pregnancy increases iodine requirements substantially for three reasons:
- Maternal thyroid hormone production increases by 50% early in pregnancy to support the metabolic demands of pregnancy and to provide T4 to the fetus before fetal thyroid function develops at approximately 12-14 weeks gestation
- Renal iodide clearance increases due to increased glomerular filtration rate — more iodine is lost in urine
- Fetal thyroid hormone synthesis from week 12-14 onward draws additional iodine from the maternal pool, transferred across the placenta
The pregnancy RDA of 220 mcg/day (versus 150 mcg/day for non-pregnant adults) reflects these increased needs. Lactation increases the requirement further to 290 mcg/day because iodine is concentrated in breast milk to supply the nursing infant.
Inadequate maternal iodine intake during pregnancy has well-documented adverse fetal effects, ranging in severity from:
- Mild maternal subclinical hypothyroidism with low-normal offspring IQ at school age
- Moderate deficiency with measurable cognitive deficits (5-15 IQ point reductions in cohort studies)
- Severe deficiency with cretinism, intellectual disability, deafness, and motor impairment in offspring
The American Thyroid Association recommends that all pregnant women in the US take a prenatal vitamin containing at least 150 mcg potassium iodide daily. Many prenatal vitamins do not contain iodine, so women should check the label specifically. Regular cod consumption (2-3 servings per week) combined with normal iodine intake from dairy and salt typically provides adequate iodine without supplementation, but the safety margin is narrower in pregnancy — women who avoid dairy, use non-iodized salt, and eat little ocean fish should specifically supplement.
The cod liver oil discussion in the Vitamin D and Liver Oil page is relevant here too — cod liver oil delivers Vitamin A and D but minimal iodine (the iodine is in the cod muscle, not the liver oil). A pregnant woman who eats cod fillet provides iodine; a pregnant woman who takes cod liver oil does not.
Pediatric Iodine and IQ
The relationship between iodine status and cognitive development has been one of the most consistent findings in pediatric nutritional epidemiology. Meta-analyses of studies in iodine-deficient versus iodine-adequate regions show approximately 10-15 IQ point differences in school-age children, with the deficit beginning prenatally and partially persisting through childhood even after iodine repletion.
The neurodevelopmental damage from severe maternal iodine deficiency is largely irreversible because it occurs during critical periods of fetal brain development — particularly the period of neuronal migration and cortical organization in the second trimester. Postnatal iodine supplementation does not fully reverse the deficit.
Even mild maternal iodine deficiency, of the kind currently common in the UK and parts of Europe, appears to produce measurable cognitive effects in offspring. The Bath SC Lancet 2013 study followed children whose mothers had mild iodine deficiency during pregnancy (urinary iodine concentration 50-150 mcg/L) and compared their school-age cognitive scores to children of mothers with adequate iodine status. The deficient-mother group had statistically significant deficits in verbal IQ, reading accuracy, and reading comprehension at age 8.
This finding has been part of the motivation for renewed iodization efforts in the UK and EU. It also has clinical implications for individual families — women planning pregnancy should specifically address iodine status before conception, ideally by including iodine-rich foods (cod, dairy, eggs) regularly and considering a prenatal vitamin with iodine.
Cretinism and the WHO Salt Iodization Program
Endemic cretinism — the severe form of congenital hypothyroidism caused by maternal iodine deficiency — remains the leading preventable cause of intellectual disability worldwide. The condition has two clinical phenotypes:
- Neurological cretinism — severe intellectual disability, deafness, motor impairment, with goiter sometimes absent. Caused by severe maternal iodine deficiency during early pregnancy affecting fetal neurodevelopment.
- Myxedematous cretinism — severe growth retardation, hypothyroid facies, with goiter typically absent. Caused by combined iodine and selenium deficiency.
The WHO/UNICEF Universal Salt Iodization program, launched in 1990, has been one of the most successful public-health interventions in history. Salt iodization is technically simple (potassium iodate is mixed with salt at approximately 20-40 ppm), cheap (less than 5 cents per person per year), and effective. The number of countries with adequate iodine intake has risen from approximately 67 in 2003 to over 120 in 2020. Several billion people have been moved from at-risk iodine status to adequate status through salt iodization alone.
The remaining iodine-deficient regions are concentrated in:
- Sub-Saharan Africa with weak salt-iodization enforcement
- Mountainous regions with low-iodine soils and traditional salt sources (Andes, Himalayas, Ethiopian Highlands)
- Inland China provinces, although the situation has improved dramatically
- Specific cultural groups within otherwise iodine-replete countries (some traditional salt-avoiding diets, organic-food-only households using non-iodized sea salt)
The cod-consumption angle: traditional fish-eating coastal cultures, even in regions where the soil-iodine content is low, generally have adequate population iodine status because ocean fish provide a backup iodine source independent of salt or dairy. Norwegian, Icelandic, Faroese, and Japanese populations have historically had low cretinism rates despite living in northern latitudes with limited terrestrial iodine sources, primarily because of high cod and other ocean-fish consumption.
Iodine Prophylaxis After Nuclear Accidents
The most acute public-health application of iodine intake is the post-nuclear-accident iodine-blocking protocol. Nuclear reactor accidents (Chernobyl 1986, Fukushima Daiichi 2011, and theoretical future events) release radioactive iodine-131 (half-life 8 days), iodine-133 (half-life 20 hours), and other shorter-lived isotopes. These airborne isotopes are inhaled, deposit on food and water, and are concentrated in the thyroid gland through the same NIS-mediated transport that handles dietary iodine.
Radioactive iodine deposited in the thyroid produces localized radiation damage and dramatically increases the risk of thyroid cancer over the following 10-30 years — particularly in children whose thyroid glands are still growing. The post-Chernobyl thyroid cancer epidemic in Belarus, Ukraine, and Russia produced approximately 7,000 cases over 25 years, predominantly in individuals who were children at the time of exposure and whose iodine intake was below adequate before the accident.
Iodine prophylaxis works by saturating the thyroid with non-radioactive iodine so that subsequent radioactive iodine uptake is competitively blocked. The standard protocol is:
- Adults: 130 mg potassium iodide (KI) tablet, single dose, taken within 24 hours before or 4 hours after exposure
- Children 3-18 years: 65 mg KI
- Children 1 month - 3 years: 32 mg KI
- Infants under 1 month: 16 mg KI
The 130 mg adult dose is approximately 100 times the daily RDA but is given only once or twice in an acute emergency, not chronically. KI tablets are stockpiled in nuclear-emergency-planning zones (within 10-50 miles of operating reactors) and were distributed to school-age children near Fukushima within 24-48 hours of the 2011 accident.
Dietary iodine adequacy before a nuclear accident also matters. Individuals with iodine deficiency at baseline have an "iodine-hungry" thyroid that aggressively concentrates whatever iodine is available, including radioactive iodine. Adequate baseline iodine status reduces the proportion of radioactive iodine that is absorbed into the thyroid. The post-Chernobyl thyroid cancer epidemic was disproportionately severe in iodine-deficient regions for this reason.
The cod-consumption relevance is indirect but real: a population eating cod regularly has adequate baseline iodine status and therefore lower thyroid radioiodine uptake in the unlikely event of a nuclear accident. This is one of the smaller arguments for routine ocean-fish consumption, but it is a real biological effect.
Iodine Excess and Thyroid Risks
The flip side of iodine deficiency is iodine excess. The Tolerable Upper Intake Level (UL) for iodine is 1,100 mcg/day for adults. Above this level, susceptible individuals can develop iodine-induced thyroid dysfunction in either direction:
- Iodine-induced hyperthyroidism (Jod-Basedow phenomenon) — particularly in individuals with previously undiagnosed nodular goiter, sudden exposure to large iodine doses can trigger autonomous thyroid hormone production and clinical hyperthyroidism. Common scenarios include iodinated contrast for CT scans, amiodarone (an iodine-rich antiarrhythmic, 75 mg iodine per 200 mg tablet), and high-dose kelp supplements.
- Iodine-induced hypothyroidism (Wolff-Chaikoff effect) — very high iodine doses transiently block thyroid hormone synthesis as a protective mechanism. Normally this is brief and self-limiting (the "escape from Wolff-Chaikoff"), but in patients with autoimmune thyroiditis or after thyroid surgery, the gland may fail to escape and remain persistently underactive.
- Acceleration of autoimmune thyroiditis — as discussed in the Hashimoto's section above, supraphysiologic iodine can worsen autoimmune progression.
Cod consumption at normal dietary levels (2-3 servings per week, 100-170 mcg iodine per serving) is well within the safe range. Even daily cod consumption (700-1,200 mcg iodine per week from cod alone, plus baseline intake from other foods) is below the daily UL and below the threshold for clinical concern in healthy individuals.
The risk situations for iodine excess from cod-related products are:
- Concentrated cod-derived supplements — rare; most cod-based supplements (cod liver oil, cod collagen) deliver minimal iodine
- Kelp marketed as "natural iodine" — one tablet can deliver several thousand mcg iodine, well above the UL
- Iodine drops (Lugol's solution, SSKI) — pharmaceutical iodine preparations delivering tens of mg per drop; should only be used under medical supervision
- Iodinated radiographic contrast — a single CT scan with contrast delivers approximately 30 grams of iodine, vastly exceeding the dietary UL; can trigger Jod-Basedow in nodular goiter patients
Practical Cod Consumption for Thyroid Support
For most adults seeking to support thyroid function through diet:
- Baseline recommendation: 2-3 cod servings per week (4-6 ounces cooked per serving), providing approximately 280-510 mcg iodine per week from cod, plus background intake from dairy, eggs, and iodized salt
- For pregnant or lactating women: 2-3 cod servings per week combined with prenatal vitamin containing 150 mcg potassium iodide; verify dietary intake meets the elevated RDA of 220-290 mcg/day
- For Hashimoto's patients: 1-2 cod servings per week is fine and provides beneficial selenium; avoid kelp and high-dose iodine supplements; consider 200 mcg/day selenium supplementation under physician supervision
- For confirmed iodine-deficiency hypothyroidism (rule out autoimmune first): 3-4 cod servings per week as part of iodine repletion strategy, along with iodized salt and potentially potassium iodide supplementation; monitor TSH at 6-12 week intervals
- For sodium-restricted diets: regular cod consumption becomes more important as a substitute iodine source when iodized salt intake is restricted
- For vegan/vegetarian transitioning back to fish: cod is often a well-tolerated and easy first-fish reintroduction; its mild flavor and flaky texture are accessible to people unaccustomed to strong fish flavors
Specific patients who should be cautious about high-frequency cod consumption:
- Patients with nodular goiter or known thyroid autonomy — daily ocean fish may push iodine intake high enough to trigger Jod-Basedow
- Patients on amiodarone — the medication contains very high iodine; additional dietary iodine should be modest
- Patients on lithium — lithium interferes with thyroid hormone release; iodine status should be carefully managed
Key Research Papers
- Zimmermann MB (2009). Iodine deficiency. Endocrine Reviews. — PubMed
- Bath SC, Steer CD, Golding J, Emmett P, Rayman MP (2013). Effect of inadequate iodine status in UK pregnant women on cognitive outcomes in their children: results from the Avon Longitudinal Study of Parents and Children (ALSPAC). The Lancet. — PubMed
- van Zuuren EJ, Albusta AY, Fedorowicz Z, Carter B, Pijl H (2013). Selenium supplementation for Hashimoto's thyroiditis. Cochrane Database of Systematic Reviews. — PubMed
- Pearce EN, Andersson M, Zimmermann MB (2013). Global iodine nutrition: where do we stand in 2013? Thyroid. — PubMed
- Bizhanova A, Kopp P (2009). The sodium-iodide symporter NIS and pendrin in iodide homeostasis of the thyroid. Endocrinology. — PubMed
- Bianco AC, Salvatore D, Gereben B, Berry MJ, Larsen PR (2002). Biochemistry, cellular and molecular biology, and physiological roles of the iodothyronine selenodeiodinases. Endocrine Reviews. — PubMed
- Karl H et al. (2001). Iodine in seafood: free iodine, iodide and iodate in cod, haddock, and other commercial fish species. Lebensmittelchemie. — PubMed
- Andersson M, Karumbunathan V, Zimmermann MB (2012). Global iodine status in 2011 and trends over the past decade. Journal of Nutrition. — PubMed
- Stagnaro-Green A et al. (2011). Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and postpartum. Thyroid. — PubMed
- Cardis E et al. (2005). Cancer consequences of the Chernobyl accident: 20 years on. Journal of Radiological Protection. — PubMed
- Zhao W, Han C, Shi X, Xiong C, Sun J, Shan Z, Teng W (2014). Prevalence of goiter and thyroid nodules before and after implementation of the universal salt iodization program in mainland China from 1985 to 2014: a systematic review and meta-analysis. PLoS One. — PubMed
- Toulis KA, Anastasilakis AD, Tzellos TG, Goulis DG, Kouvelas D (2010). Selenium supplementation in the treatment of Hashimoto's thyroiditis: a systematic review and a meta-analysis. Thyroid. — PubMed
PubMed Topic Searches
- PubMed: Cod iodine and thyroid function
- PubMed: Cod selenium content
- PubMed: Selenium and Hashimoto's
- PubMed: Iodine deficiency in pregnancy and IQ
- PubMed: Salt iodization and cretinism
Connections
- Cod Hub
- Cod Benefits Deep Dive
- Cod Lean Protein Profile
- Cod Liver Oil & Vitamin D
- Mercury vs Other Fish
- Iodine
- Selenium
- Zinc (Thyroid Cofactor)
- Hashimoto's Thyroiditis
- Hypothyroidism
- Hyperthyroidism
- Goiter
- TSH Lab Test
- Free T4 Lab Test
- Free T3 Lab Test
- Salmon
- Herring
- Yogurt (Iodine Source)
- Eggs (Iodine Source)
- Milk (Iodine Source)