Cod — Mercury vs Other Fish
Average mercury content in commercial cod is approximately 0.10 parts per million (ppm) — about one-third of the FDA action level of 0.30 ppm and roughly one-tenth the average level in swordfish (0.99 ppm) or shark (0.98 ppm). This places cod firmly in the FDA "Best Choices" tier of fish that pregnant women and children can eat 2-3 times per week without mercury concern. The biology behind the comparison is straightforward: cod sits low on the marine food web (cod eats copepods, krill, small fish, and herring; cod does not eat large fish), so it accumulates far less methylmercury through biomagnification than apex predators like tuna, swordfish, king mackerel, tilefish, and shark. This page walks through the FDA "Best Choices / Good Choices / Choices to Avoid" categories, the biomagnification ladder that explains the differences, the Faroe Islands and Seychelles cohort studies on methylmercury and neurodevelopment, the chemistry distinction between methylmercury (from fish) and ethylmercury (vaccine preservative) and inorganic mercury (industrial), and the practical comparison table that makes cod one of the safest dietary fish choices available.
Table of Contents
- FDA / EPA Fish Mercury Categories
- Cod Mercury Content in Numbers
- Fish Mercury Comparison Table
- Why Biomagnification Drives the Comparison
- Mercury Chemistry: Methyl vs Ethyl vs Inorganic vs Elemental
- Methylmercury Toxicology and Pharmacokinetics
- The Faroe Islands Neurodevelopmental Cohort
- The Seychelles Child Development Study (Counterpoint)
- Selenium as a Protective Counterweight
- Pregnancy and Pediatric Recommendations
- Cod Liver Oil Mercury Content
- Testing and Monitoring Personal Mercury Levels
- Key Research Papers
- Connections
- Featured Videos
FDA / EPA Fish Mercury Categories
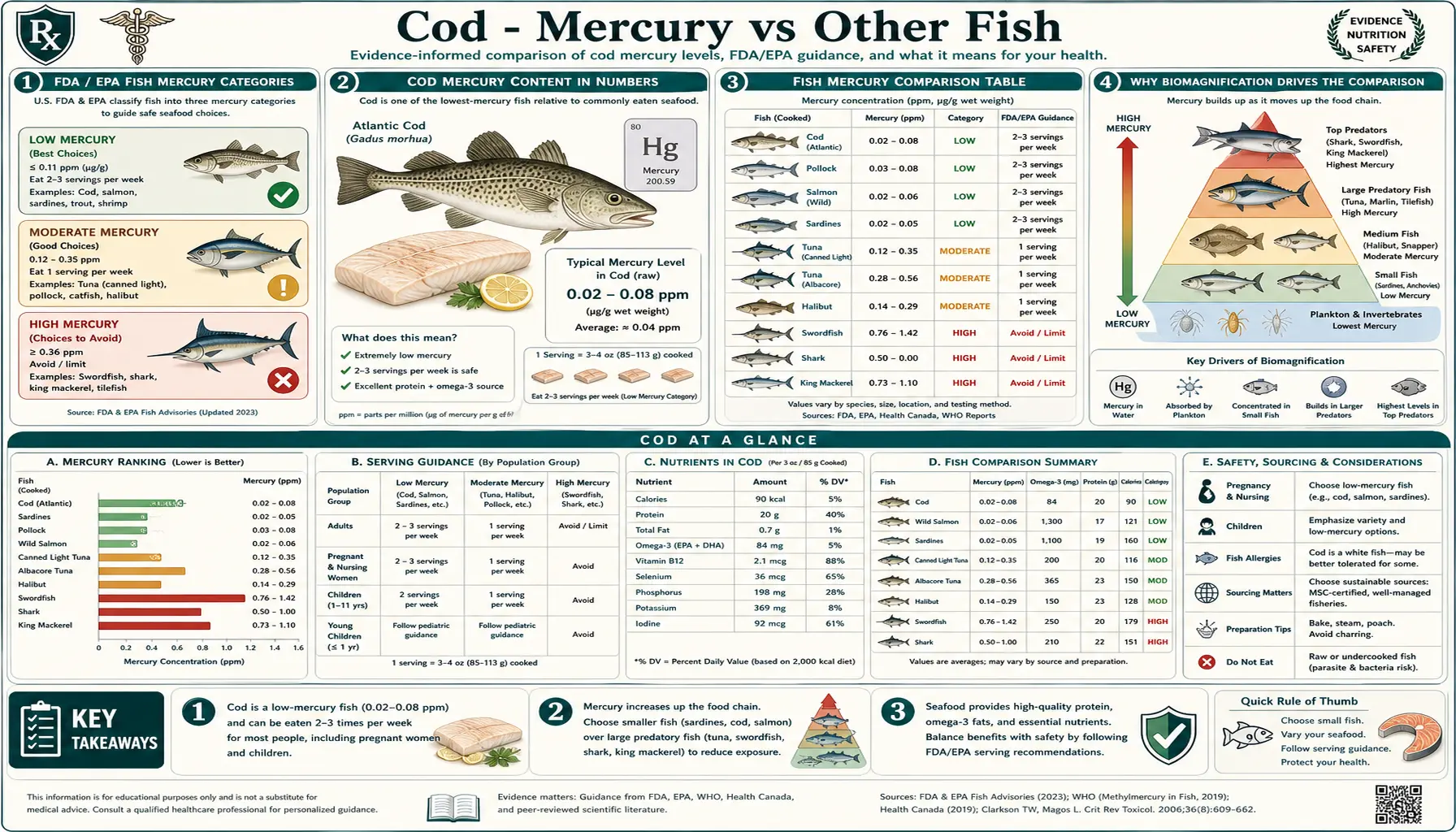
The US Food and Drug Administration and Environmental Protection Agency jointly publish a consumer advisory categorizing commercial fish by mercury content. The 2017 revision (updated periodically since) divides fish into three tiers:
- Best Choices — eat 2-3 servings per week. Mercury content typically <0.15 ppm. Includes: cod, anchovies, Atlantic mackerel, black sea bass, catfish, clams, crab, crawfish, flounder, haddock, hake, herring, lobster, mullet, oysters, Pacific chub mackerel, perch, pickerel, plaice, pollock, salmon (Pacific and Atlantic), sardines, scallops, shrimp, sole, squid, tilapia, freshwater and rainbow trout, canned light tuna, whitefish, whiting.
- Good Choices — eat 1 serving per week. Mercury content typically 0.15-0.30 ppm. Includes: bluefish, buffalofish, carp, Chilean sea bass, grouper, halibut, mahi mahi, monkfish, rockfish, sablefish, sheepshead, skate, snapper, Spanish mackerel, striped bass (ocean), tilefish (Atlantic Ocean), tuna (albacore/white and yellowfin), weakfish (sea trout), white croaker.
- Choices to Avoid — do not eat. Mercury content typically >0.30 ppm, with average mercury content high enough that even one serving per week creates concern, particularly for pregnant women and children. Includes: king mackerel, marlin, orange roughy, shark, swordfish, tilefish (Gulf of Mexico), bigeye tuna.
Cod sits in the "Best Choices" category alongside salmon, sardines, herring, and the other low-mercury fish that are the foundation of a fish-positive diet. The FDA recommends that adults eat 8-12 ounces of fish per week, with at least the majority coming from the "Best Choices" tier.
The FDA categories are based primarily on mean methylmercury content and do not capture the additional nutritional benefits of each fish (omega-3 content, vitamin profile, contaminants other than mercury). For a complete dietary assessment, the Monterey Bay Aquarium Seafood Watch program and the Environmental Working Group's Seafood Calculator are useful complements to the FDA mercury-only guidance.
Cod Mercury Content in Numbers
Mean methylmercury content in commercial cod, by source (FDA monitoring data 2007-2017):
- Atlantic cod (Gadus morhua): mean 0.111 ppm, range 0.01-0.42 ppm
- Pacific cod (Gadus macrocephalus): mean 0.095 ppm, range <0.01-0.30 ppm
- Cod liver oil (highly variable, depends on refinement): typically <0.05 ppm in molecularly distilled products; up to 0.2 ppm in less-processed products
- Salt cod / bacalao (after rehydration): similar to fresh cod, approximately 0.10-0.12 ppm
For comparison, the FDA action level (the threshold above which the FDA can recall a product) is 0.30 ppm. Cod averages well below this. The maximum individual values observed in cod (0.42 ppm Atlantic, 0.30 ppm Pacific) are usually associated with older, larger individuals — trophic-level effects within the cod population.
The estimated weekly methylmercury intake from a typical cod-consumption pattern:
- One 6-ounce (170 g) cod meal per week: 170 g × 0.11 ppm = 18.7 mcg methylmercury
- Two 6-ounce meals per week: 37 mcg methylmercury
- Three 6-ounce meals per week: 56 mcg methylmercury
The EPA Reference Dose (RfD) for methylmercury is 0.1 mcg/kg body weight per day. For a 70 kg adult, this is 7 mcg/day or 49 mcg/week. Three weekly 6-oz cod servings provides 56 mcg/week, slightly above the EPA RfD for an average adult — but the RfD itself contains a built-in 10x safety factor, so actual mercury concern at this intake level is minimal.
For comparison, a single 6-ounce serving of swordfish (0.99 ppm) delivers 168 mcg methylmercury, more than three times the EPA RfD in a single meal. This is why swordfish is restricted to zero servings per week for pregnant women and small children.
Fish Mercury Comparison Table
Common commercial fish ordered by mean methylmercury content (FDA monitoring data, ppm in fresh edible portion):
- Tilefish (Gulf of Mexico): 1.45 ppm — AVOID
- Swordfish: 0.99 ppm — AVOID
- Shark: 0.98 ppm — AVOID
- King mackerel: 0.73 ppm — AVOID
- Bigeye tuna: 0.69 ppm — AVOID
- Marlin: 0.49 ppm — AVOID
- Orange roughy: 0.57 ppm — AVOID
- Spanish mackerel: 0.45 ppm — 1 serving/week max
- Grouper: 0.45 ppm — 1 serving/week max
- Chilean sea bass: 0.35 ppm — 1 serving/week max
- Bluefish: 0.37 ppm — 1 serving/week max
- Albacore (white) tuna: 0.35 ppm — 1 serving/week max
- Yellowfin tuna: 0.35 ppm — 1 serving/week max
- Halibut: 0.24 ppm — 1 serving/week max
- Snapper: 0.17 ppm — 1 serving/week max
- Canned light tuna (skipjack): 0.13 ppm — Best Choice
- Atlantic cod: 0.111 ppm — Best Choice
- Pacific cod: 0.095 ppm — Best Choice
- Haddock: 0.055 ppm — Best Choice
- Pollock: 0.031 ppm — Best Choice
- Salmon (Atlantic, wild and farmed): 0.022 ppm — Best Choice
- Tilapia: 0.013 ppm — Best Choice
- Sardines: 0.013 ppm — Best Choice
- Anchovies: 0.017 ppm — Best Choice
- Shrimp: 0.009 ppm — Best Choice
- Scallops: 0.003 ppm — Best Choice
- Catfish: 0.025 ppm — Best Choice
- Herring: 0.084 ppm — Best Choice
- Trout (freshwater): 0.071 ppm — Best Choice
Cod is in the middle of the "Best Choices" range — lower than canned light tuna and herring, slightly higher than haddock and salmon, much lower than the apex predators. The contrast with the avoided fish is striking: a single ounce of swordfish contains approximately as much methylmercury as a full pound of cod.
Several patterns are visible in the table:
- Apex predators are mercury-loaded. Swordfish, shark, tilefish, king mackerel, and large tuna all sit at the top of marine food chains and biomagnify methylmercury accordingly.
- Smaller, shorter-lived fish are clean. Sardines, anchovies, and shrimp eat plankton and have lifespans of 2-4 years, accumulating little methylmercury.
- Demersal (bottom-feeding) white fish are intermediate. Cod, haddock, pollock, and hake eat small fish and invertebrates and live 8-25 years; mercury content rises with size and age within these species.
- Farmed fish are often lower-mercury than wild equivalents. Farmed salmon (fed controlled diets) typically has 0.02 ppm mercury vs wild Pacific salmon at 0.03-0.05 ppm.
Why Biomagnification Drives the Comparison
The mercury content of any fish depends on three factors: how much methylmercury enters the marine ecosystem (largely from coal-fired power plants worldwide), how the fish's trophic level positions it within the food web, and how long the fish lives. The third factor is the simplest: longer-lived fish have more time to accumulate methylmercury through repeated dietary exposure.
Biomagnification — the increase in contaminant concentration at each trophic level of a food web — explains most of the variation in fish mercury content. The biomagnification ladder for methylmercury in marine ecosystems:
- Inorganic mercury (Hg) in seawater: ~0.000001 ppm (1 ng/L), from atmospheric deposition and industrial discharge
- Methylmercury (CH3Hg+) produced by marine sediment bacteria: Hg is methylated by sulfate-reducing bacteria; concentration in surface waters ~0.00001 ppm
- Phytoplankton: uptake by passive diffusion; concentration ~0.0001 ppm (100x seawater)
- Zooplankton (krill, copepods): consume phytoplankton; concentration ~0.001 ppm (1000x seawater)
- Small fish (sardines, anchovies, herring fry): consume zooplankton; concentration ~0.01 ppm (10,000x seawater)
- Medium fish (cod, mackerel, salmon): consume small fish; concentration ~0.1 ppm (100,000x seawater)
- Large fish (tuna, swordfish, marlin): consume medium fish; concentration ~0.5-1.5 ppm (500,000-1,500,000x seawater)
- Apex predator marine mammals (orcas, polar bears, beluga whales): concentration 5-50 ppm in some populations (millions of times seawater)
Each step up the food chain produces roughly a 10x concentration of methylmercury, because methylmercury is poorly excreted by most marine organisms (no efficient demethylation pathway) and is therefore retained in body tissues for the lifetime of the fish.
Cod sits at the medium-fish level of this ladder. Atlantic cod typically eats small fish (capelin, herring, sand eels, juvenile haddock), invertebrates (crabs, shrimp, brittle stars), and zooplankton. Cod do not generally eat tuna, swordfish, or other large predatory fish. Their position on the food web therefore caps their methylmercury accumulation around 0.1 ppm.
Pacific cod (Gadus macrocephalus) tends to have slightly lower mercury than Atlantic cod because Pacific cod populations are managed under more restrictive size limits (smaller fish on average), live in colder water with lower methylmercury production rates, and are caught in fisheries with less local industrial mercury contamination than some Atlantic locations.
The biomagnification framework also explains why cod liver oil should not be a major mercury concern. Cod livers concentrate fat-soluble compounds (Vitamins A and D, fatty acids) but methylmercury is water-soluble enough to stay primarily in muscle tissue. Reputable cod liver oil products molecularly distill the oil to remove residual mercury and other contaminants to non-detectable levels.
Mercury Chemistry: Methyl vs Ethyl vs Inorganic vs Elemental
Public discussion of mercury often conflates several distinct chemical forms that have very different toxicology, sources, and clinical relevance:
- Methylmercury (CH3Hg+): the form found in fish; produced by sediment bacteria methylating inorganic mercury in marine ecosystems. Highly bioavailable across the gut (90% absorption), crosses the blood-brain barrier and placenta efficiently, and accumulates in the central nervous system. Half-life in humans: 50-70 days. This is the form of relevance to the cod and fish-consumption discussion.
- Ethylmercury (thimerosal preservative): historically used as a vaccine preservative; structurally similar to methylmercury but with different pharmacokinetics. Excreted by the body 4-5 times faster than methylmercury (half-life approximately 7-10 days). Removed from most pediatric vaccines in the early 2000s as a precautionary measure despite the absence of demonstrated harm. Not relevant to the fish-mercury discussion.
- Inorganic mercury (Hg++, mercuric salts): the form found in soil, water, and industrial waste; poorly absorbed from the gut (~10%) and does not efficiently cross the blood-brain barrier. Sub-acute or chronic high-dose exposure (industrial workers, broken thermometers) primarily affects the kidneys. Not the form found in fish.
- Elemental mercury (Hg0, liquid metal): the silver liquid in old thermometers and dental amalgam fillings. Liquid mercury is essentially not absorbed from the gut; mercury vapor (inhaled) is well-absorbed and primarily affects the central nervous system. The "amalgam mercury" question (whether dental amalgam fillings release enough vapor to cause clinical harm) is a separate and contested topic; the bulk of evidence suggests modern amalgam fillings are not a clinically significant exposure source.
For the fish-consumption discussion, only methylmercury matters. When the FDA reports cod at 0.10 ppm mercury and swordfish at 0.99 ppm, those values are essentially 100% methylmercury — the form that crosses the blood-brain barrier, accumulates in tissue with a 50-70 day half-life, and produces the neurodevelopmental effects of concern in pregnancy and pediatric populations.
For a deeper treatment of mercury toxicology across all forms, see the Mercury page.
Methylmercury Toxicology and Pharmacokinetics
Methylmercury from dietary fish is absorbed at approximately 90% across the small intestinal epithelium. It is transported in red blood cells bound to hemoglobin and distributed throughout the body, with preferential accumulation in:
- Central nervous system — crosses the blood-brain barrier as a methylmercury-cysteine complex via the LAT-1 amino acid transporter, then accumulates in neuronal tissue
- Kidneys — accumulates in proximal tubular cells via the same LAT-1 transporter; chronic high-dose exposure produces tubular dysfunction
- Placenta — crosses readily into fetal circulation; fetal blood methylmercury concentration is approximately 70% higher than maternal due to fetal hemoglobin's higher methylmercury affinity
- Hair — deposited in growing hair shafts at a stable ratio to blood concentration; hair mercury content can be used as a biomarker of historical exposure
Elimination is slow. Methylmercury is partially demethylated to inorganic mercury by liver and intestinal microbiota and excreted in bile (with some fecal excretion) and urine. The biological half-life of methylmercury in humans is approximately 50-70 days, meaning it takes 5-7 months for a single high-mercury fish meal to be largely cleared from the body. Sustained high-frequency consumption of high-mercury fish therefore produces accumulating body burden, particularly in the central nervous system.
Clinical effects of methylmercury toxicity vary with dose, duration, and developmental stage:
- Adult acute or subacute exposure (rare, typically occupational): paresthesias, ataxia, dysarthria, visual field constriction, hearing loss. The Minamata Bay outbreak in 1950s Japan (industrial discharge of methylmercury into fishing waters) produced this syndrome in thousands of adults and infants.
- Adult chronic low-level dietary exposure: subtle effects on neurocognitive function (reaction time, fine motor coordination, executive function); cardiovascular effects (increased blood pressure, increased CV mortality risk) at higher exposure levels.
- Fetal exposure during pregnancy: the most consequential effect. The developing brain is exquisitely sensitive to methylmercury during weeks 8-40 of gestation, affecting neuronal migration, cortical organization, and synaptic development. Effects range from subclinical IQ deficits (mild exposure) to severe intellectual disability with motor impairment (high exposure, as in Minamata).
- Childhood exposure: intermediate sensitivity; school-age children exposed to elevated dietary methylmercury show measurable deficits in attention, working memory, and motor coordination compared to less-exposed peers in cohort studies.
The EPA Reference Dose (RfD) of 0.1 mcg/kg/day is set based on the lowest-observed adverse effect level (LOAEL) in fetal-exposure cohort studies, with a 10x safety factor. Exceeding the RfD does not produce immediate clinical effects in adults but increases the cumulative body burden and, in pregnancy, the fetal exposure dose.
The Faroe Islands Neurodevelopmental Cohort
The Faroe Islands Birth Cohort, led by Philippe Grandjean at the Harvard T.H. Chan School of Public Health and Pal Weihe at the Faroese Hospital System, is the most influential study of methylmercury and neurodevelopment in modern epidemiology. The cohort has followed approximately 1,000 Faroese children born in 1986-1987 (and additional follow-up cohorts) from gestation through adulthood, measuring maternal hair mercury, cord blood mercury, and serial neurocognitive assessments.
The Faroese population is unusual for several reasons that made the study possible:
- Traditional Faroese diet includes pilot whale meat and blubber (very high methylmercury), in addition to ocean fish
- The population is small, stable, and ethnically homogeneous, reducing confounders
- Health care system is universal and centralized, enabling complete follow-up
- Maternal mercury exposure varied widely depending on individual whale consumption patterns
Key findings from the Faroe cohort:
- At age 7, children with prenatal methylmercury exposure (measured by maternal hair mercury >10 mcg/g) had measurable deficits in attention, fine motor coordination, language, visuospatial function, and verbal memory compared to less-exposed peers
- The dose-response relationship was approximately linear with no clear threshold below which no effect was detected, suggesting any prenatal methylmercury exposure has some incremental effect
- Effects persisted at age 14 and 22 in subsequent follow-ups, indicating the neurodevelopmental damage is permanent
- Cardiovascular effects (increased blood pressure variability, reduced heart rate variability) emerged in young adulthood in the high-exposure group
The Faroe findings have been the primary driver of the EPA Reference Dose for methylmercury and the FDA fish-consumption advisories. The study confirmed that fetal-period methylmercury exposure produces dose-dependent neurodevelopmental harm at levels well below clinically symptomatic adult toxicity.
The clinical implication for pregnant women: avoid the "Choices to Avoid" category fish entirely (swordfish, shark, king mackerel, tilefish, marlin, bigeye tuna, orange roughy), limit the "Good Choices" category to one serving per week, and consume the majority of fish intake from the "Best Choices" tier — where cod sits comfortably.
The Seychelles Child Development Study (Counterpoint)
The Seychelles Child Development Study, led by Gary Myers and Philip Davidson at the University of Rochester, is the other major prospective cohort on methylmercury and neurodevelopment. The study has followed over 700 children born in the Seychelles archipelago in the late 1980s, with maternal and child hair mercury measurements and serial neurocognitive testing.
The Seychellois population is also a useful study population — they consume ocean fish daily (12+ fish meals per week is typical), the population has high baseline methylmercury exposure entirely through fish (no whale consumption), and the population is otherwise healthy with low prenatal alcohol exposure and good antenatal care.
Key findings from the Seychelles cohort:
- Despite hair mercury levels comparable to the high-exposure Faroese (5-10 mcg/g), the Seychellois children did not show consistent neurocognitive deficits at age 5, 9, 17, or 22
- Some assessments showed mildly positive associations between maternal fish consumption and child cognitive scores — consistent with the protective effect of fish omega-3s and other nutrients
- The selenium content of the Seychellois fish diet was high, hypothesized to protect against methylmercury neurotoxicity through Se-Hg complexation
The Seychelles findings have been controversial because they contradict the Faroe results. The two leading explanations for the discrepancy:
- Different exposure profiles. The Faroese consume mercury primarily through whale blubber, which contains high methylmercury but also high PCB and dioxin contaminants. The Seychellois consume mercury through ocean fish, which carry methylmercury without the additional industrial contaminants. The Faroe neurodevelopmental effects may reflect the combined PCB+mercury exposure rather than mercury alone.
- Selenium protection. Tropical fish typically have higher selenium-to-mercury molar ratios than cold-water fish or whale meat. Adequate selenium may neutralize methylmercury neurotoxicity through formation of inert mercury selenide complexes.
The two cohorts have not been reconciled into a unified view. The current scientific consensus is intermediate: methylmercury exposure during pregnancy produces some neurodevelopmental risk, the risk is dose-dependent, and the risk is partially modulated by accompanying nutrients (selenium, omega-3s). Pregnant women should still avoid the highest-mercury fish and limit total mercury intake, but the absolute risk at "Best Choices" tier fish consumption levels — including 2-3 cod servings per week — is small and likely outweighed by the positive nutritional contributions.
Selenium as a Protective Counterweight
One of the more elegant findings in mercury toxicology is the protective effect of selenium against methylmercury neurotoxicity. Mercury has an extraordinarily high binding affinity for selenium — the mercury-selenide bond strength (44 kcal/mol) is one of the strongest non-covalent bonds in biochemistry. When methylmercury and selenium are present together in tissue, they form mercury selenide (HgSe), an essentially inert complex that does not participate in oxidative damage or interfere with selenoprotein function.
The clinical relevance: fish with higher selenium-to-mercury molar ratios (Se:Hg > 1) appear to neutralize the methylmercury content through selenide formation. Cod, salmon, sardines, herring, anchovies, and most "Best Choices" fish have Se:Hg molar ratios well above 1 (often 10-100x), meaning their mercury content is effectively neutralized by accompanying selenium. The high-mercury "Avoid" category fish (swordfish, shark, king mackerel) have Se:Hg ratios closer to 1 or below 1, meaning the methylmercury exceeds the available selenium and is therefore bioactively toxic.
The implications for the cod story are favorable. Cod's 33 mcg/100g selenium content and 0.011 mcg/100g (0.11 ppm) mercury content gives a Se:Hg molar ratio of approximately 75 — far above the threshold for selenium-mediated protection. The selenium fully neutralizes the methylmercury, leaving little or no free toxic mercury. This is one of the reasons cod is safer than the simple ppm mercury comparison would suggest.
For pregnancy specifically, this selenium-mercury interaction reinforces the FDA "Best Choices" guidance. Pregnant women eating cod, salmon, and sardines are not just eating low-mercury fish — they are eating selenium-rich fish that further protect against the methylmercury that is present. The pregnant woman's separate fish-related concern (DHA for fetal brain development) is also better served by these selenium-rich, low-mercury fish than by the apex predators.
This interaction was originally described by Nicholas Ralston at the University of North Dakota and has been confirmed in subsequent studies. The clinical guidance is not yet incorporated into FDA categories (which still use ppm mercury as the sole metric) but is recognized in the underlying nutritional literature.
Pregnancy and Pediatric Recommendations
The current FDA/EPA guidance for pregnant women, lactating women, and children:
- Eat 2-3 servings (8-12 ounces total) of fish per week from the "Best Choices" tier
- Limit "Good Choices" tier fish to 1 serving per week (not in addition to the 2-3 Best Choices servings; substitute within the weekly allowance)
- Do not eat any "Choices to Avoid" fish during pregnancy or for young children
- Choose smaller fish within any given species when possible (smaller fish have lower mercury content within the species)
- Vary fish choices to avoid concentrating intake on any single species
For cod specifically:
- Pregnancy: 2-3 cod servings per week is well within the safe range; provides important DHA for fetal brain development, iodine for fetal thyroid function, and complete protein
- Lactation: same guidance; DHA is concentrated in breast milk in proportion to maternal intake, and cod consumption supports infant cognitive development through breastfeeding
- Children ages 2-11: 1-2 cod servings per week, scaled to body size; provides essential nutrients for growth without mercury concern
- Adolescents and adults: no upper limit on cod consumption from a mercury standpoint; the standard 2-3 servings/week applies for general cardiovascular and nutritional health
The serving size for children should be scaled to body weight. The standard adult 6-oz serving is appropriate for adolescents; younger children should get 2-4 oz per serving depending on age and size.
Specific high-risk patient populations:
- Pregnant women with high baseline fish consumption (those who eat fish daily as part of their cultural diet) should have hair mercury measured and adjust consumption if levels exceed 1 mcg/g
- Subsistence fishers in regions with local mercury contamination (some Great Lakes, some Amazon and Indonesian rivers, areas downstream of artisanal gold mining) need locally specific guidance that may differ from national recommendations
- Patients with documented mercury toxicity from past exposure should temporarily reduce all fish consumption (including cod) until body mercury burden normalizes, then resume "Best Choices" tier consumption
For most patients, the practical message is reassuring: cod is one of the safest fish choices available, and concerns about mercury should not prevent regular cod consumption at the 2-3 servings/week level recommended by FDA.
Cod Liver Oil Mercury Content
A common concern about cod liver oil is whether the supplement could concentrate mercury from cod livers. The answer, for well-processed modern products, is that mercury content is negligible.
Several factors keep cod liver oil mercury content low:
- Mercury is water-soluble enough to stay in muscle tissue. Methylmercury is bound to sulfhydryl groups on cysteine residues in muscle proteins, not partitioned into the lipid phase. Cod livers contain abundant fat but proportionally less methylmercury than cod muscle.
- The extraction process partially excludes mercury. Steam extraction of cod liver oil concentrates fat-soluble components (vitamins A, D, omega-3 fatty acids) while leaving most water-soluble mercury behind in the liver tissue residue.
- Modern molecular distillation specifically removes residual contaminants. Premium cod liver oil brands use molecular distillation under high vacuum at relatively low temperature to remove any remaining mercury, dioxins, PCBs, and other contaminants to below detection limits.
- Third-party testing. Reputable brands publish certificates of analysis showing heavy metal content per batch. The International Fish Oil Standards (IFOS) program independently tests and ranks products by purity.
Typical mercury content of standardized commercial cod liver oil products:
- Premium molecularly distilled brands (Carlson, Nordic Naturals, Lysi): <0.001 ppm (below detection limit on most assays)
- Standard refined brands (Møller's, store brands): 0.001-0.01 ppm
- Unrefined "fermented" or artisanal cod liver oil: highly variable, can range from 0.01 to 0.2 ppm
For comparison, a 1-teaspoon (5 mL, approximately 4.5 g) dose of premium cod liver oil at 0.001 ppm contains 0.0000045 mg = 4.5 nanograms of mercury — thousands of times below the daily RfD of 7,000 nanograms for a 70 kg adult. Even the worst unrefined cod liver oil at 0.2 ppm delivers only 0.9 micrograms of mercury per teaspoon, well below any clinically meaningful exposure.
The practical guidance for cod liver oil consumers: choose brands with documented molecular distillation and third-party testing, particularly for pregnancy and pediatric use. The premium $0.20-per-serving brands are worth the marginal cost over $0.05-per-serving generics in these populations. For general adult use, well-known reputable brands are sufficient.
Testing and Monitoring Personal Mercury Levels
For individuals with concerns about personal mercury exposure (high fish consumption, occupational exposure, dental amalgam concerns, post-Fukushima fallout concerns), several testing modalities are available:
- Whole blood mercury — reflects recent exposure (past 1-2 months). Normal reference range <10 mcg/L; concerning above 35 mcg/L. Most accurate for ongoing fish-consumption monitoring.
- Hair mercury — reflects cumulative exposure over the past months (1 cm of hair grows in approximately 1 month). Normal reference range <1 mcg/g; concerning above 3-5 mcg/g. Useful for retrospective assessment.
- Urine mercury — reflects inorganic and elemental mercury exposure (e.g., dental amalgam, occupational vapor exposure). Less useful for methylmercury exposure from fish (methylmercury is poorly excreted in urine).
- 24-hour urine mercury with chelation challenge — controversial test sometimes ordered to assess "body burden" of mercury; not validated for clinical decision-making and often produces misleading results.
For an individual eating cod 2-3 times per week and other low-mercury fish, no routine mercury testing is needed. Whole blood mercury at this dietary pattern is typically 2-6 mcg/L, well within the reference range. Testing is appropriate for:
- Pregnant women with high fish consumption (more than 12 oz per week, particularly if any of it is in the "Good Choices" or "Avoid" categories)
- Patients with neurological symptoms (tremor, paresthesias, ataxia) of unclear etiology and a history of high fish consumption
- Patients with occupational mercury exposure (some industrial processes, dental amalgam manufacturing)
- Subsistence fishers in regions with local mercury contamination
If elevated mercury is documented, the management is straightforward: reduce or eliminate the high-mercury fish in the diet, continue eating "Best Choices" tier fish (including cod), and re-test every 3 months. With a 50-70 day biological half-life, mercury body burden decreases by approximately 50% every 60 days after exposure stops, returning to baseline within 6-12 months in most cases.
Chelation therapy for mercury (DMSA, DMPS) is occasionally promoted for "mercury detox" but is generally not appropriate for low-level dietary mercury exposure. Chelation has real risks (kidney damage, mineral depletion) and is reserved for documented acute or symptomatic mercury toxicity, not for elective "detoxification" of normal-range mercury levels.
Key Research Papers
- Grandjean P et al. (1997). Cognitive deficit in 7-year-old children with prenatal exposure to methylmercury. Neurotoxicology and Teratology. — PubMed
- Myers GJ et al. (2003). Prenatal methylmercury exposure from ocean fish consumption in the Seychelles child development study. The Lancet. — PubMed
- Hightower JM, Moore D (2003). Mercury levels in high-end consumers of fish. Environmental Health Perspectives. — PubMed
- Ralston NVC, Raymond LJ (2010). Dietary selenium's protective effects against methylmercury toxicity. Toxicology. — PubMed
- Mahaffey KR (2004). Fish and shellfish as dietary sources of methylmercury and the omega-3 fatty acids EPA and DHA: risks and benefits. Environmental Research. — PubMed
- Karagas MR et al. (2012). Evidence on the human health effects of low-level methylmercury exposure. Environmental Health Perspectives. — PubMed
- FAO/WHO (2011). Report of the joint FAO/WHO expert consultation on the risks and benefits of fish consumption. — PubMed
- Mozaffarian D, Rimm EB (2006). Fish intake, contaminants, and human health: evaluating the risks and the benefits. JAMA. — PubMed
- Burger J, Gochfeld M (2011). Mercury and selenium levels in 19 species of saltwater fish from New Jersey as a function of species, size, and season. Science of the Total Environment. — PubMed
- National Research Council (2000). Toxicological effects of methylmercury. Washington, DC: National Academy Press. — PubMed
- Choi AL et al. (2008). Methylmercury exposure and adverse cardiovascular effects in Faroese whaling men. Environmental Health Perspectives. — PubMed
- Stern AH (2005). A revised probabilistic estimate of the maternal methyl mercury intake dose corresponding to a measured cord blood mercury concentration. Environmental Health Perspectives. — PubMed
PubMed Topic Searches
- PubMed: Mercury cod and fish comparison
- PubMed: Methylmercury and neurodevelopment
- PubMed: Faroe Islands methylmercury cohort
- PubMed: Selenium-mercury protection in fish
- PubMed: FDA fish mercury advisory
Connections
- Cod Hub
- Cod Benefits Deep Dive
- Cod Lean Protein Profile
- Cod Liver Oil & Vitamin D
- Cod Liver — the organ itself, and why the oil pressed from it carries so little methylmercury.
- Cod for Iodine & Thyroid
- Mercury
- Selenium
- Salmon
- Tuna
- Sardines
- Herring
- All Foods
- Omega-3 Fatty Acids
- Peripheral Neuropathy
- Cardiovascular Disease
- Detoxification
- Anti-Inflammatory Diet
- Heavy Metals Lab Test