Lightheadedness on Standing
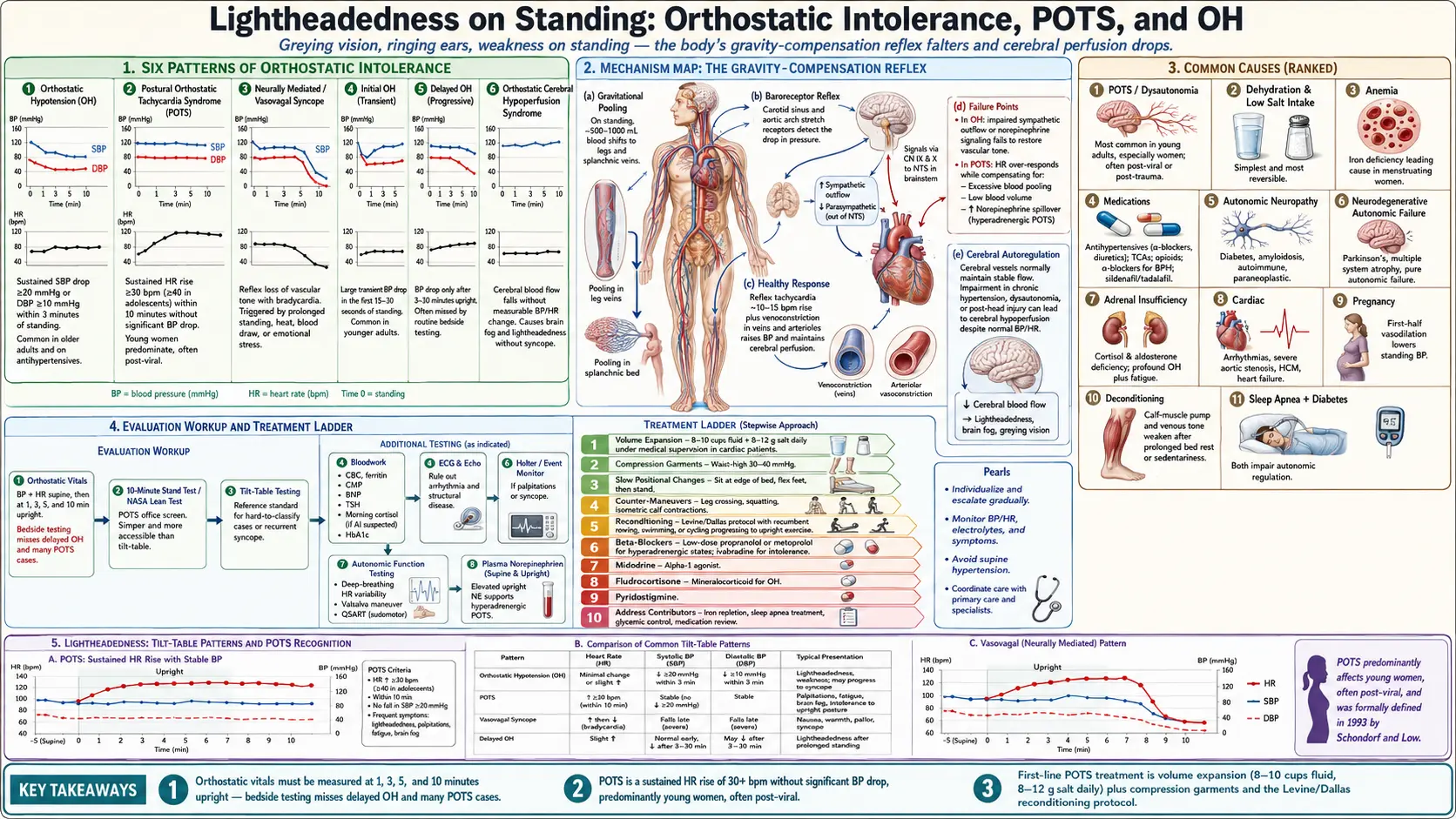

Table of Contents
- Overview
- Types of Orthostatic Intolerance
- Common Causes
- Mechanisms
- Evaluation
- Management
- When to Seek Medical Care
- Connections
- References & Research
- Featured Videos
Overview
Lightheadedness on standing — the sense of being about to faint, with graying vision, ringing in the ears, weakness, and sometimes nausea — is the cardinal symptom of orthostatic intolerance. The body normally compensates for the gravitational pull on blood as you stand by tightening the leg veins and increasing heart rate; when that reflex falters, cerebral perfusion drops and you feel faint. Most cases are benign (dehydration, deconditioning, vasovagal sensitivity) but persistent or severe orthostatic symptoms can signal autonomic dysfunction, anemia, structural heart disease, or autonomic failure from neurodegenerative disease, and warrant evaluation.
Types of Orthostatic Intolerance
- Orthostatic hypotension (OH) — sustained drop in systolic blood pressure of at least 20 mmHg or diastolic of at least 10 mmHg within 3 minutes of standing. Common in older adults and on antihypertensives.
- Postural orthostatic tachycardia syndrome (POTS) — sustained heart-rate rise of 30 bpm or more (40 in adolescents) within 10 minutes of standing, without a significant drop in blood pressure. Predominantly affects young women.
- Neurally mediated syncope (vasovagal) — reflex loss of vascular tone with bradycardia, often triggered by prolonged standing, heat, blood draws, or emotional stress.
- Initial orthostatic hypotension — large transient blood-pressure drop in the first 15–30 seconds of standing; common in younger adults.
- Delayed orthostatic hypotension — blood pressure drop only after 3–30 minutes upright; often missed by routine bedside testing.
- Orthostatic cerebral hypoperfusion syndrome — cerebral blood flow falls without measurable BP or HR change; produces brain fog and lightheadedness without overt syncope.
Common Causes
- POTS and dysautonomia — the most common cause in young adults, especially women. Often follows a viral illness or trauma. See deep dives: Subtypes, Medications Guide.
- Dehydration and low salt intake — the simplest and most reversible cause; often combined with hot environments or vigorous exercise.
- Anemia — reduced oxygen-carrying capacity exaggerates orthostatic symptoms; iron deficiency is the leading cause in menstruating women.
- Medications — antihypertensives (especially alpha-blockers and diuretics), tricyclic antidepressants, opioids, alpha-blockers for prostatic hyperplasia, sildenafil and tadalafil.
- Autonomic neuropathy — from diabetes, amyloidosis, autoimmune disease, or paraneoplastic syndromes.
- Neurodegenerative autonomic failure — Parkinson's disease, multiple system atrophy, pure autonomic failure.
- Adrenal insufficiency — cortisol and aldosterone deficiency cause profound orthostatic hypotension and fatigue.
- Cardiac causes — arrhythmias, severe aortic stenosis, hypertrophic cardiomyopathy, heart failure.
- Pregnancy — vasodilation in the first half lowers standing blood pressure.
- Deconditioning — after prolonged bed rest or sedentary lifestyle, the calf-muscle pump and venous tone weaken.
- Sleep apnea and diabetes — both impair autonomic regulation.
Mechanisms
- Gravitational pooling — on standing, 500–1,000 mL of blood shifts into the legs and splanchnic veins. The healthy response is reflex tachycardia (~10–15 bpm rise) and venoconstriction.
- Baroreceptor reflex — carotid and aortic stretch receptors detect the drop and trigger sympathetic activation via the brainstem.
- Failure points — in OH, sympathetic outflow or norepinephrine signaling fails. In POTS, the heart rate over-responds to compensate for excessive blood pooling, low blood volume, or increased norepinephrine spillover.
- Cerebral autoregulation — the brain normally maintains constant blood flow across a wide BP range; this autoregulation is impaired in chronic hypertension, dysautonomia, and after head injury.
- Hypovolemia — many POTS patients have low total blood volume; correcting it with salt and fluids is often the first effective treatment.
Evaluation
- Orthostatic vitals — blood pressure and heart rate supine, then at 1, 3, 5, and 10 minutes upright. Bedside testing misses delayed OH and many POTS cases.
- 10-minute stand test (NASA Lean Test) — the in-office screen for POTS; simpler than tilt-table and reproduces symptoms in most patients.
- Tilt-table testing — the reference standard for hard-to-classify cases or recurrent syncope.
- Bloodwork — CBC, ferritin, comprehensive metabolic panel, BNP, TSH, morning cortisol if adrenal insufficiency suspected, HbA1c.
- ECG and echocardiogram — rule out arrhythmia and structural disease.
- Holter or event monitor — if palpitations or syncope.
- Autonomic function testing — deep-breathing heart-rate variability, Valsalva, QSART.
- Plasma norepinephrine supine and upright — to identify hyperadrenergic POTS.
Management
- Volume expansion — 8–10 cups of fluid daily, 8–12 grams of salt for most adults with POTS or OH (under medical supervision in cardiac patients).
- Compression garments — waist-high 30–40 mmHg compression reduces venous pooling.
- Slow positional changes — sit at the edge of the bed, flex feet, then stand.
- Counter-maneuvers — leg crossing, squatting, isometric calf contractions during standing.
- Reconditioning — recumbent exercise (rowing, swimming, cycling) progressing to upright. The Levine / Dallas protocol is widely used in POTS.
- Beta-blockers — low-dose propranolol or metoprolol for hyperadrenergic symptoms; ivabradine for those who do not tolerate beta-blockers.
- Midodrine — alpha-1 agonist that increases vascular tone; useful in OH.
- Fludrocortisone — mineralocorticoid that expands volume; second-line for OH.
- Pyridostigmine — cholinergic agent useful in some POTS subtypes.
- Address contributors — iron repletion, sleep apnea treatment, glycemic control, medication review.
When to Seek Medical Care
- Loss of consciousness or near-loss with injury, exertional syncope, or while driving.
- Chest pain, shortness of breath, or palpitations accompanying orthostatic symptoms.
- Family history of sudden cardiac death.
- New focal neurologic signs, rapidly progressive autonomic symptoms.
- Severe orthostatic symptoms in a patient over 60, or with known heart, kidney, or neurologic disease.
- Symptoms not improving with adequate hydration, salt, and conditioning.
Connections
- All Symptoms
- POTS
- Diabetes
- POTS Subtypes
- Anemia
- Arrhythmia
- POTS Medications Guide
- Parkinson's Disease
- Obstructive Sleep Apnea
- Addison's Disease
- Brain Fog
- Fatigue
- Iron
- Heart Palpitations
- MCAS
- POTS/MCAS/EDS Triad
- Cardiomyopathy
- Atrial Fibrillation
- Dizziness
References & Research
Historical Background
Orthostatic intolerance was systematically studied in the post-WWII era when pilots experienced syncope during high-G flight. Subsequent NASA bed-rest studies revealed how rapidly the cardiovascular and autonomic systems decondition without gravitational stress. POTS was formally defined in 1993 by Schondorf and Low, and the diagnosis has expanded steadily as clinicians recognize subtler hyperadrenergic and hypovolemic forms.
Key Research Papers
- Schondorf R, Low PA. Idiopathic postural orthostatic tachycardia syndrome: an attenuated form of acute pandysautonomia? Neurology. 1993;43(1):132-137.
- Sheldon RS, Grubb BP, Olshansky B, et al. 2015 Heart Rhythm Society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome. Heart Rhythm. 2015;12(6):e41-e63.
- Freeman R, Wieling W, Axelrod FB, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Autonomic Neuroscience. 2011;161(1-2):46-48.
- Low PA, Singer W. Management of neurogenic orthostatic hypotension: an update. Lancet Neurology. 2008;7(5):451-458.
- Fu Q, Vangundy TB, Galbreath MM, et al. Cardiac origins of the postural orthostatic tachycardia syndrome. Journal of the American College of Cardiology. 2010;55(25):2858-2868.
- Low PA, Sandroni P, Joyner M, Shen WK. Postural tachycardia syndrome (POTS). Journal of Cardiovascular Electrophysiology. 2009;20(3):352-358.
- Stewart JM, Boris JR, Chelimsky G, et al. Pediatric disorders of orthostatic intolerance. Pediatrics. 2018;141(1):e20171673.
- Brignole M, Moya A, de Lange FJ, et al. 2018 ESC guidelines for the diagnosis and management of syncope. European Heart Journal. 2018;39(21):1883-1948.
- Raj SR, Guzman JC, Harvey P, et al. Canadian Cardiovascular Society position statement on POTS and related disorders of chronic orthostatic intolerance. Canadian Journal of Cardiology. 2020;36(3):357-372.
- Vernino S, Bourne KM, Stiles LE, et al. Postural orthostatic tachycardia syndrome (POTS): state of the science and clinical care from a 2019 National Institutes of Health expert consensus meeting. Autonomic Neuroscience. 2021;235:102828.
PubMed Topic Searches
- Postural orthostatic tachycardia syndrome (POTS)
- Orthostatic hypotension management
- Tilt-table testing and syncope
- Hyperadrenergic POTS
- Autonomic neuropathy in diabetes
- Levine / Dallas exercise protocol for POTS