Pleural Effusion: History and Discovery
A pleural effusion is a build-up of fluid in the pleural space — the thin gap between the lung and the chest wall. Although the precise term is modern, the condition is one of the oldest recognized in all of medicine. More than two thousand years ago Hippocrates described pus in the chest (empyema), taught physicians to shake a patient and listen for the splashing "succussion" sound of trapped fluid, and even cut into the chest to drain it. The bedside revolution of the eighteenth and nineteenth centuries — Auenbrugger's tapping percussion (1761) and Laennec's stethoscope (1816–1819) — let doctors detect an effusion without surgery, and the Boston physician Henry Ingersoll Bowditch turned needle drainage (thoracentesis) into routine practice in the 1850s. In 1972 Richard W. Light gave clinicians a simple laboratory rule — Light's criteria — to sort effusions into "transudates" and "exudates," and that rule still guides the work-up today. This is the story of how fluid around the lung went from a death sentence shaken out by hand to a problem mapped by ultrasound and a few drops of laboratory chemistry.
Table of Contents
- What a Pleural Effusion Is
- Hippocrates, Empyema, and the Succussion Splash
- Ancient Drainage and the Long Silence After
- The Bedside Revolution: Percussion and the Stethoscope
- Bowditch and the Birth of Routine Thoracentesis
- Naming the Causes: Infection, Heart, Tuberculosis, Cancer
- Light's Criteria and the Transudate–Exudate Divide
- Imaging, Ultrasound, and the Modern Era
- Legacy: An Ancient Sign, A Modern Workup
- Research Papers and References
- Connections
- Featured Videos
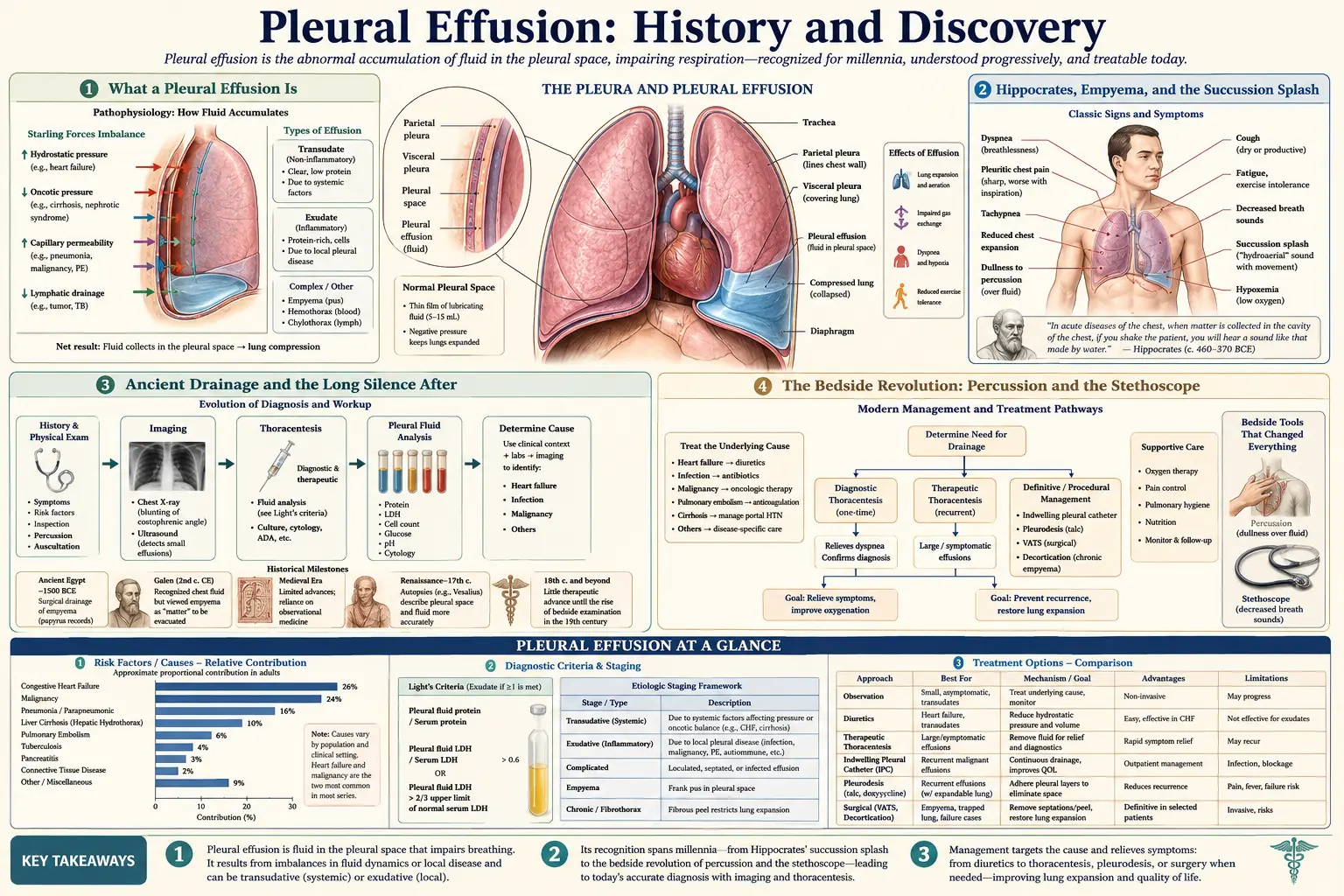
What a Pleural Effusion Is
Each lung is wrapped in a two-layered membrane called the pleura, and between those layers sits a thin film of lubricating fluid — normally only a teaspoon or two — that lets the lung glide smoothly with every breath. A pleural effusion is what happens when that small reservoir grows into a much larger collection of fluid, pressing on the lung and crowding out the air. The result is breathlessness, a dull ache or heaviness in the chest, and sometimes a dry cough. It is not itself a disease so much as a signpost: the body has accumulated fluid in the chest because something elsewhere has gone wrong.
Physicians have long divided effusions by what the fluid actually is. Watery fluid that leaks across intact membranes from pressure imbalances — classically from heart failure — is a transudate. Fluid that pours out because the pleural surface is inflamed, infected, or invaded — by pneumonia, tuberculosis, or cancer — is an exudate. When the fluid is frank pus it is an empyema; when blood, a haemothorax; when lymph, a chylothorax. The oldest of these terms, empyema, reaches all the way back to the founder of Western clinical medicine.
For most of recorded time, doctors could perceive an effusion only by its outward signs — laboured breathing, a side of the chest that moved less, the changed sound when the chest was struck or shaken. Everything that follows is the centuries-long effort to detect that hidden fluid, drain it safely, and finally read its chemistry well enough to know where it came from.
Hippocrates, Empyema, and the Succussion Splash
The recorded history of pleural effusion begins with Hippocrates and the Hippocratic Corpus around 400 BCE. Writing roughly 2,400 years ago, the Hippocratic physicians distinguished between watery fluid in the chest (what we would call hydrothorax) and pus in the chest, which they called empyema — a Greek word meaning, almost literally, "pus within." That single distinction, between clear fluid and infected fluid, is the conceptual seed of the entire later science of pleural disease, and the word empyema is still used unchanged in hospitals today.
Hippocrates also left medicine one of its most memorable bedside maneuvers, the succussion splash. Lacking any instrument, the physician would grasp the patient by the shoulders and shake the body, then listen for a sloshing, fluctuating sound from inside the chest — the splash of liquid moving against a pocket of air, exactly as a half-empty water bottle slaps when shaken. Hippocrates recognized that this "succussion" revealed fluid with a gas interface trapped in the thorax. Historians of medicine still refer to this finding as the "Hippocratic succussion," and a version of the test survived in clinical teaching into the twentieth century.
The Hippocratic writers paired observation with grim prognosis. They understood the natural course of an undrained chest infection and warned that patients with pleurisy who did not recover early would "become suppurative" — turn to pus — by around the eleventh day, watching for fever that rose at night, a dry cough, hollowed eyes, and a flush on the cheeks. In an age with no X-rays, microscopes, or antibiotics, this was acute clinical reasoning: the doctor read the hidden fluid entirely from the surface of the body and the sounds it made.
Ancient Drainage and the Long Silence After
Hippocrates did not stop at diagnosis. The Corpus describes a startlingly bold treatment for empyema: open surgical drainage of the chest. The physician was instructed to make an incision low on the side of the chest, down to a rib, and then to bore through the chest wall — in some passages with a pointed trephine, in others by resecting a portion of rib — to let the pus escape. Crucially, Hippocrates taught that the fluid should be released gradually rather than all at once, an instinct that anticipated, by more than two millennia, the modern caution against draining a large effusion too quickly. This makes the Hippocratic procedure a recognizable ancestor of today's chest-tube drainage and thoracostomy.
For several centuries this knowledge was preserved and transmitted. In the second century CE the great physician Galen cited and built upon the Hippocratic techniques for the chest, and the description of empyema drainage passed into the standard medical inheritance of the classical and medieval worlds. Yet the procedure remained dangerous and was performed rarely; without anaesthesia, antisepsis, or any understanding of why wounds became infected, opening the chest was a desperate measure reserved for the desperate.
What followed Galen was, by comparison, a long quiet. Across the medieval and early Renaissance periods the understanding of pleural fluid advanced little beyond what the Greeks had set down, and drainage of empyema was practiced cautiously and inconsistently. The decisive breakthroughs would come not from new surgery but from a different idea entirely — that a physician could learn what lay inside the living chest by listening to it. That idea arrived in the eighteenth and nineteenth centuries and changed everything.
The Bedside Revolution: Percussion and the Stethoscope
The first great advance came from Vienna in 1761, when the Austrian physician Leopold Auenbrugger published his short book Inventum Novum ("A New Discovery"). Auenbrugger described percussion: tapping the chest with the fingers and judging the sound. A healthy, air-filled lung gave a hollow, resonant note; a chest filled with fluid gave a flat, dull thud. The story goes that he drew the idea from boyhood memories of his father, an innkeeper, tapping wine barrels to gauge how full they were. For the first time, a doctor could map a hidden collection of pleural fluid through the intact chest wall by sound alone.
Auenbrugger's discovery was largely ignored for nearly fifty years, until Napoleon's physician Jean-Nicolas Corvisart translated and championed it in 1808 and percussion was suddenly adopted across European medicine. Then, in 1816, the French physician René Laennec at the Necker Hospital in Paris took the next step. Reluctant to press his ear directly to a young woman's chest, he rolled a sheet of paper into a tube and discovered that it carried the internal sounds more clearly than ever. From that improvised cylinder he developed the stethoscope, and in 1819 he published his landmark treatise on mediate auscultation, a comprehensive guide to the sounds of diseases of the lungs and heart.
Together, percussion and auscultation transformed pleural effusion from a condition guessed at by shaking the patient into one that could be reliably detected at the bedside. A physician could now percuss the dull, fluid-filled lower chest, listen for the silence where breath sounds should be, and locate the upper level of the fluid — all without a single incision. This new diagnostic precision set the stage for the next question: once you knew the fluid was there, how could you get it out safely?
Bowditch and the Birth of Routine Thoracentesis
The answer was thoracentesis — inserting a hollow needle or trocar between the ribs to draw off pleural fluid. The basic idea of tapping the chest was ancient, but as a safe, deliberate, repeatable bedside procedure it belongs largely to the nineteenth century, and in the United States its great champion was the Boston physician Henry Ingersoll Bowditch (1808–1892). Bowditch had studied in Paris under the school of Pierre Louis, where he absorbed the new French methods of auscultation and percussion, and he returned to Massachusetts convinced that physicians could and should both diagnose effusions with the stethoscope and relieve them with the needle.
In the 1850s Bowditch published influential accounts urging the medical profession to adopt trocar thoracentesis for pleural effusions, pairing precise stethoscope-and-percussion diagnosis with controlled drainage. He is widely credited with introducing systematic thoracentesis and modern chest examination into American practice, and his persistence helped turn what had been an occasional, feared intervention into an accepted, lifesaving routine. His popular teaching manual, The Young Stethoscopist, spread the new bedside skills to a generation of physicians.
Thoracentesis did two things at once, and still does. It relieves the patient, draining off the fluid that compresses the lung and easing the breathlessness almost immediately; and it diagnoses, because the fluid drawn out can be inspected, measured, and tested to learn why it accumulated. That second role — the tapped fluid as a clue, not merely a burden to remove — would become central a century later, once laboratory chemistry could read the fluid in detail. Bowditch gave medicine the safe sample; the twentieth century learned how to interpret it.
Naming the Causes: Infection, Heart, Tuberculosis, Cancer
As diagnosis and drainage matured, physicians increasingly recognized that "water on the chest" was not one disease but the shared end-point of many. The most important step was distinguishing effusions driven by simple pressure and fluid overload from those driven by disease of the pleural surface itself. Heart failure emerged as the leading cause of the watery, low-protein effusions: when the failing heart backs fluid up into the circulation, that fluid weeps across the intact pleura into the chest, often on both sides. These are the classic transudates.
On the other side stood the inflammatory and invasive causes. Pneumonia was recognized as a frequent trigger; an infection in the adjacent lung inflames the pleura and provokes a "parapneumonic" effusion that, if it becomes infected, turns into the very empyema Hippocrates had described. Tuberculosis, the great scourge of the eighteenth and nineteenth centuries, was a major cause of pleural effusion and remains so across much of the world today. And as pathology and oncology developed, physicians came to understand that cancer — whether arising in the lung, spreading from the breast or elsewhere, or, in the case of mesothelioma, growing in the pleura itself — could seed the pleural surface and produce a malignant effusion.
By the early twentieth century a working list of culprits was in place: heart failure, pneumonia and other infections, tuberculosis, and cancer, alongside less common causes such as kidney and liver disease, pulmonary embolism, and injury. What was still missing was a quick, objective way to tell, from the fluid itself, which category an effusion belonged to — a leak from pressure, or a product of local disease. That tool arrived in 1972.
Light's Criteria and the Transudate–Exudate Divide
In 1972 the American pulmonologist Richard W. Light and colleagues published a study in the Annals of Internal Medicine titled "Pleural effusions: the diagnostic separation of transudates and exudates." It offered a simple, reproducible laboratory rule — soon known universally as Light's criteria — for sorting any effusion into one of the two great categories. The insight was that exudates, born of inflamed or leaky pleura, carry much more protein and the enzyme lactate dehydrogenase (LDH) than transudates do, and that comparing the fluid to the patient's blood captures this difference cleanly.
An effusion is classified as an exudate if it meets at least one of three conditions: the ratio of pleural-fluid protein to blood (serum) protein is greater than 0.5; the ratio of pleural-fluid LDH to serum LDH is greater than 0.6; or the pleural-fluid LDH is greater than two-thirds of the upper normal limit for serum LDH. If none of the three is met, the fluid is a transudate. The practical payoff is large: a transudate points the doctor back toward systemic problems such as heart failure, cirrhosis, or kidney disease, while an exudate demands a search for local pleural disease — infection, tuberculosis, cancer, or inflammation — and usually further testing of the fluid.
More than half a century later, Light's criteria remain the cornerstone of the pleural-effusion workup and are still taught and used worldwide. They are not perfect — the rule is highly sensitive for exudates but tends to misclassify a minority of transudates as exudates, especially in patients on strong diuretics, which is why clinicians sometimes add tests such as the serum-to-fluid protein or albumin gradient. But for turning a tapped sample of fluid into an immediate, actionable diagnosis, no simpler tool has displaced it. Light's criteria are, in effect, the modern laboratory descendant of the question Hippocrates first asked at the bedside: what kind of fluid is this, and what does it mean?
Imaging, Ultrasound, and the Modern Era
The twentieth century added eyes to the physician's ears. After Wilhelm Roentgen discovered X-rays in 1895, the chest radiograph quickly became a standard way to confirm and measure an effusion, revealing the characteristic blunting of the sharp angle where the diaphragm meets the chest wall and, in larger collections, a dense white field where air should be. Computed tomography (CT), introduced in the 1970s, later allowed effusions to be measured precisely and distinguished from lung collapse, masses, and pleural thickening, and helped reveal underlying causes such as tumors.
The most important recent change at the bedside, however, has been ultrasound. Real-time ultrasound lets the clinician see the pocket of fluid directly, gauge its size, detect the strands and pockets that signal infection, and — critically — guide the needle safely into the fluid while avoiding the lung, the diaphragm, and blood vessels. Ultrasound guidance has substantially improved the safety of thoracentesis and is now considered best practice for draining pleural fluid, effectively giving Bowditch's nineteenth-century procedure a set of modern eyes.
The modern toolkit also includes thin chest tubes and indwelling catheters that let recurrent effusions be drained at home, and thoracoscopy, in which a camera is passed into the pleural space to take biopsies and treat the lining directly. Yet the bedside chain remains recognizably the one built up over two millennia: notice the breathlessness, confirm the fluid (now with imaging rather than a shaking of the shoulders), drain it safely, and analyze it — with Light's criteria — to find the cause.
Legacy: An Ancient Sign, A Modern Workup
Few conditions trace such an unbroken thread from antiquity to the modern clinic as pleural effusion. The vocabulary alone tells the story: empyema, thoracentesis, and the very idea of distinguishing watery fluid from pus all descend, in name and in concept, from the Hippocratic writers of the fifth century BCE. What changed across the centuries was not the underlying problem — fluid in the wrong place around the lung — but the steadily sharpening tools used to find it, remove it, and explain it.
Each era added one decisive layer. The Greeks contributed recognition, the succussion splash, and the audacious idea of draining the chest. Auenbrugger and Laennec made the hidden fluid audible through percussion and the stethoscope. Bowditch made needle drainage a safe and routine act of both relief and diagnosis. The causes — heart failure, pneumonia, tuberculosis, cancer — were named one by one as pathology matured. Light's criteria turned the tapped fluid into a two-minute decision, and ultrasound made the whole sequence safer than ever before.
For a patient today, the experience is almost unimaginably gentler than it once was: an ultrasound probe, a brief needle tap under local anaesthetic, a few tubes of fluid sent to the laboratory, and within hours an answer about why the fluid gathered and what to do next. Behind that quiet, ordinary procedure stand twenty-four centuries of physicians who learned, step by patient step, to read the fluid around the lung. To learn the modern clinical picture — the symptoms, causes, tests, and treatments — see the main Pleural Effusion article.
Research Papers and References
The references below combine landmark and review articles — including Richard Light's original 1972 paper defining the transudate–exudate criteria and historical studies of Hippocratic empyema and the introduction of thoracentesis — with curated PubMed topic-search links into the history and diagnosis of pleural disease. Where a stable identifier was confirmed it is given as a DOI or PMID; the remaining entries open a PubMed (National Library of Medicine) topic search in a new tab. Ancient primary sources (the Hippocratic Corpus, Galen) are named in the article as historical texts rather than as modern citations.
- Light RW, Macgregor MI, Luchsinger PC, Ball WC Jr. Pleural effusions: the diagnostic separation of transudates and exudates. Annals of Internal Medicine. 1972;77(4):507-513. — doi:10.7326/0003-4819-77-4-507
- Light RW. The Light criteria: the beginning and why they are useful 40 years later. Clinics in Chest Medicine. 2013;34(1):21-26. — doi:10.1016/j.ccm.2012.11.006
- Christopoulou-Aletra H, Papavramidou N. "Empyemas" of the thoracic cavity in the Hippocratic Corpus. The Annals of Thoracic Surgery. 2008;85(3):1132-1134. — doi:10.1016/j.athoracsur.2007.10.078
- Kaplan A. The Hippocratic splash. Journal of Emergency Medicine / NLM archive. — PMC6346804: The Hippocratic Splash
- Hippocrates introducing thoracotomy combined with tracheal intubation for parapneumonic pleural effusions and empyema thoracis. — PMID 27821625
- Henry Ingersoll Bowditch: the prominent physician who introduced thorax examination and trocar thoracentesis in the United States of America. — PMID 38371003
- History of thoracentesis and pleural drainage — from the ancient Greeks to modern technique. — PubMed: thoracentesis history and pleural drainage
- Auenbrugger and the invention of percussion of the chest (Inventum Novum, 1761). — PubMed: Auenbrugger percussion history
- Laennec and the invention of the stethoscope — mediate auscultation of chest disease. — PubMed: Laennec stethoscope history
- Parapneumonic effusion and empyema — pathophysiology, diagnosis, and management. — PubMed: parapneumonic effusion and empyema
- Tuberculous pleural effusion — diagnosis and historical context. — PubMed: tuberculous pleural effusion diagnosis
- Malignant pleural effusion — causes, mechanisms, and treatment. — PubMed: malignant pleural effusion management
- Thoracic ultrasound guidance for thoracentesis and pleural procedures. — PubMed: ultrasound-guided thoracentesis
External Authoritative Resources
- StatPearls (NCBI Bookshelf) — Pleural Effusion
- MedlinePlus — Pleural Disorders
- PubMed — Pleural Effusion: history and diagnosis
Connections
- Pulmonology
- Pleural Effusion (Main Article)
- All Conditions
- Pneumonia
- Heart Failure
- Tuberculosis
- Pulmonary Embolism
- Metastatic Cancers