Schizophrenia: History and Discovery
Schizophrenia is one of the most misunderstood conditions in all of medicine — and much of that misunderstanding begins with its name. The word was coined by the Swiss psychiatrist Eugen Bleuler in 1908 from the Greek schizein (to split) and phren (mind), but he meant a splitting within the mind — a loosening of the connections between thought, emotion, and perception — not a "split" into two or more separate personalities. This page traces how the modern concept took shape: from Emil Kraepelin's separation of "dementia praecox" from manic-depressive illness in the 1890s, through Bleuler's renaming and Kurt Schneider's symptom checklists, to the 1952 discovery of chlorpromazine and the dopamine hypothesis that grew out of it. Throughout, names, dates, and the difference between an observation and a theory are stated as precisely as the historical record allows.
Table of Contents
- Madness Before a Name: Early Descriptions
- Emil Kraepelin and "Dementia Praecox"
- Eugen Bleuler Coins "Schizophrenia" (1908–1911)
- The "Split Personality" Myth, Debunked
- Kurt Schneider and the First-Rank Symptoms
- Chlorpromazine, 1952: The Treatment Revolution
- The Dopamine Hypothesis (1960s–1970s)
- From Single Disease to Spectrum: The Modern View
- Stigma, Dignity, and Why the History Matters
- Research Papers and References
- Connections
- Featured Videos
Madness Before a Name: Early Descriptions
People have lived with what we now call schizophrenia for as long as there have been people, but the condition had no single agreed name until the turn of the twentieth century. Ancient and medieval writers described states of disordered thought, hearing voices, and withdrawal from reality, but these were lumped together with many other forms of "madness," "lunacy," or "insanity" under broad and shifting labels. There was no clear line separating the illness we now recognize from melancholia, mania, dementia, or the effects of physical disease and intoxication.
The first steps toward a modern description came in the nineteenth century. In 1852 the French psychiatrist Bénédict Augustin Morel used the phrase démence précoce ("early dementia") to describe a young patient whose mind seemed to deteriorate in adolescence. Around the same period, the German psychiatrists Karl Ludwig Kahlbaum and Ewald Hecker described distinct presentations — Kahlbaum named catatonia (1874) and Hecker named hebephrenia (1871), a disorganized form beginning in youth. These were careful clinical descriptions of pieces of the puzzle, but no one had yet argued that they were facets of a single underlying disease. That synthesis would be Emil Kraepelin's great contribution.
It is worth being precise here: Morel, Kahlbaum, and Hecker were first-describers of particular presentations and coiners of particular terms. None of them "discovered schizophrenia" in the modern sense, because the unifying concept did not yet exist. They supplied the raw observations that a later generation would weave together.
Emil Kraepelin and "Dementia Praecox"
The decisive figure in the modern history of schizophrenia is Emil Kraepelin (1856–1926), a German psychiatrist whose method was to observe large numbers of patients over the long course of their illness and to group disorders by how they began, progressed, and ended — an approach now called clinical nosology. Across the successive editions of his influential textbook (variously titled Compendium der Psychiatrie and Lehrbuch der Psychiatrie, later simply Psychiatrie), published between 1883 and 1927, Kraepelin gradually built and refined his classification of mental illness.
Kraepelin took Morel's old phrase and gave it new weight as "dementia praecox." In the fourth edition of his textbook (1893) he introduced dementia praecox as a category, and over the next two editions he brought Kahlbaum's catatonia and Hecker's hebephrenia, together with paranoid forms, under this single heading — arguing that they shared a common tendency toward progressive mental decline beginning in early adult life. The Latin name reflected exactly this idea: a dementia (a deterioration of the mind) that struck praecox (early, prematurely), in the teens or twenties rather than in old age.
Kraepelin's most consequential move came in the sixth edition (1899), where he drew a sharp and lasting distinction between dementia praecox — with its tendency toward chronic deterioration — and manic-depressive insanity (the ancestor of today's bipolar disorder and recurrent mood disorders), which tended to recur in episodes but to recover between them. This separation of the two great families of severe mental illness — one chronic and thought-centered, the other episodic and mood-centered — is one of the foundational ideas of modern psychiatry, and a version of it still structures our diagnostic manuals today.
Two cautions about Kraepelin are important for accuracy. First, his name for the disorder, "dementia praecox," carried two assumptions that later proved wrong: that the illness always begins early, and that it always ends in dementia-like decline. Neither is true — many people fall ill later, and many recover or stabilize. Second, like many of his contemporaries Kraepelin worked within "degeneration theory," a now-discredited nineteenth-century framework; modern historians (such as Hoff, and Heckers and Kendler) examine these roots critically. Kraepelin clarified the boundaries of the disorder brilliantly; the name and some of its underlying assumptions needed correcting, and that correction came from Zurich.
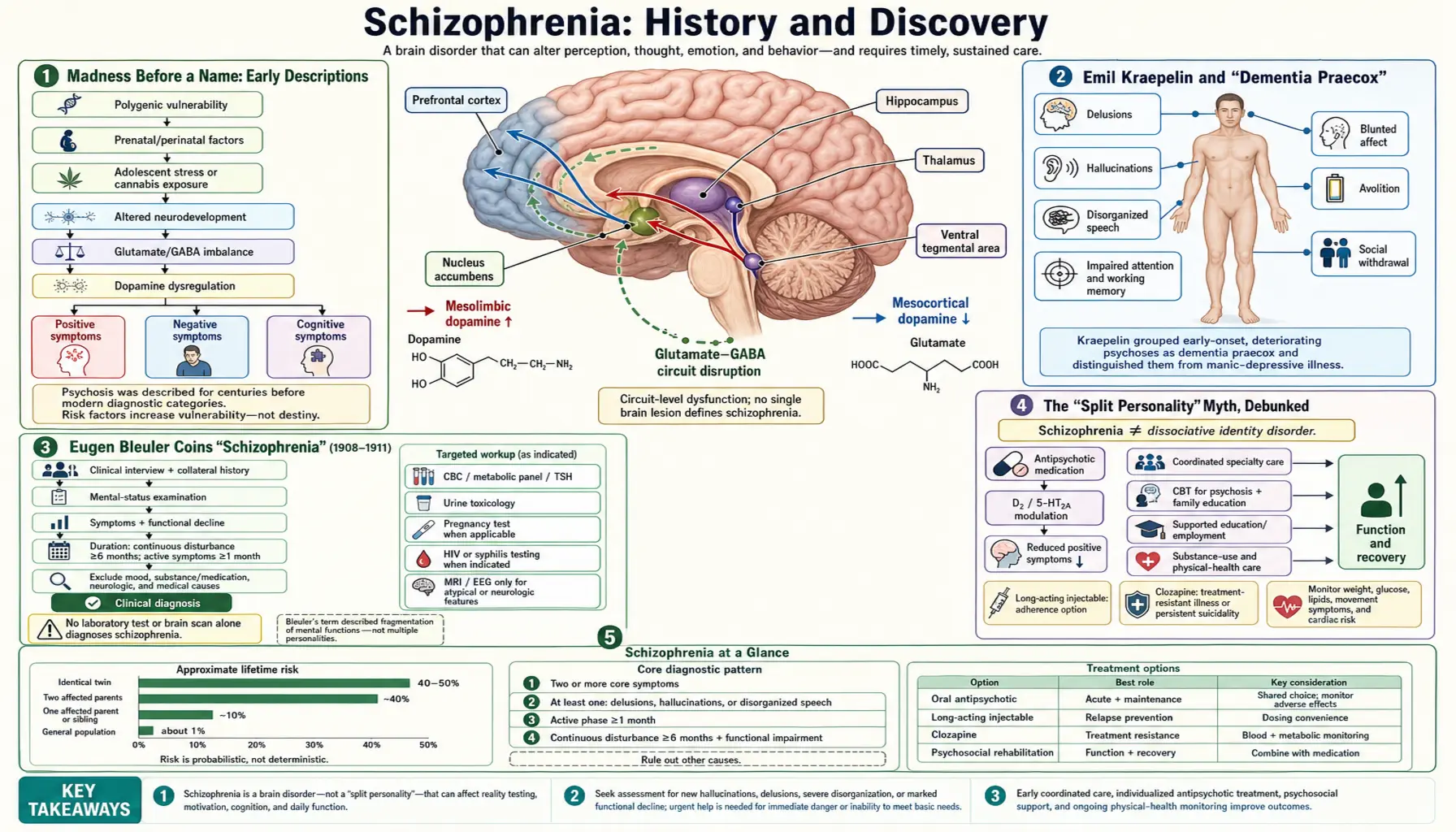
Eugen Bleuler Coins "Schizophrenia" (1908–1911)
The word "schizophrenia" was coined by Paul Eugen Bleuler (1857–1939), a Swiss psychiatrist and director of the Burghölzli clinic in Zurich. He first presented the term publicly in a lecture to the German Psychiatric Association in Berlin on 24 April 1908, and developed it fully in his landmark 1911 monograph, Dementia Praecox, oder Gruppe der Schizophrenien (Dementia Praecox, or the Group of Schizophrenias). The title itself signals two of his key arguments: that the old name should be retired, and that this was probably not one disease but a group of related conditions.
Bleuler built the new word from the Greek schizein (σχιζειν, "to split") and phren (φρην, "mind"). His intended meaning was specific and is the heart of his contribution: he saw the central feature of the illness as a splitting or loosening of the normal connections between mental functions — between thoughts and the emotions attached to them, between ideas and one another, between the inner life and outward reality. A patient might describe a tragic loss while smiling, or hold beliefs that no longer hang together logically; for Bleuler this fragmentation, this loss of the mind's normal integration, was the essence of the disorder.
Crucially, Bleuler argued that Kraepelin's name was misleading precisely because the illness is often neither a dementia nor always praecox: many patients do not deteriorate into dementia, and many do not become ill in adolescence. By renaming the condition after its characteristic psychological structure rather than its (unreliable) course and onset, he shifted the focus toward symptoms and inner experience. Bleuler also distinguished what he considered the fundamental features (often summarized as the "four A's" — disturbances of Association, Affect, Ambivalence, and Autism, meaning withdrawal into an inner world) from accessory features such as hallucinations and delusions. This emphasis on thought disorganization and blunted or incongruous emotion deeply shaped twentieth-century psychiatry.
The historical bottom line is clear and well documented across multiple sources: Kraepelin separated and characterized the disorder; Bleuler renamed it and reframed it. The name "schizophrenia" describes a split within the integration of one mind — not a split into multiple minds. That distinction is the subject of the next section, because the world got it almost universally wrong.
The "Split Personality" Myth, Debunked
Here is the single most important thing on this page: schizophrenia is not "split personality," and it is not multiple personalities. This is one of the most stubborn and damaging myths in all of mental health. Surveys by mental-health organizations have found that a majority of the public — in one widely cited National Alliance on Mental Illness survey, roughly 64 percent — wrongly believes schizophrenia means a split or multiple personality. It does not. The error comes almost entirely from a misreading of the Greek root schizein, "to split."
When Bleuler spoke of "splitting," he meant the splitting apart of mental functions within a single person — thought drifting loose from emotion, beliefs losing their logical connections, the inner world separating from shared reality. He did not mean that a person harbors two or more distinct personalities who take turns controlling their behavior. That entirely separate phenomenon is called dissociative identity disorder (DID), formerly "multiple personality disorder," and it is a dissociative condition, classified and understood quite differently from schizophrenia.
The two conditions differ in fundamental ways. Schizophrenia is a psychotic disorder: its hallmark is a loss of contact with reality — hallucinations (often hearing voices), delusions (fixed false beliefs), and disorganized thinking. A person with schizophrenia has one personality, but that single mind can become disconnected from reality and from its own normal emotional and logical coherence. Dissociative identity disorder, by contrast, involves the presence of two or more distinct identity states, typically linked to severe early trauma, and is marked by gaps in memory rather than by psychosis. As one common summary puts it, psychosis tends to add something to a person's reality (a voice, a belief), while dissociation tends to fragment the sense of self and memory.
Why does correcting this matter so much on a public-health page? Because the myth does real harm. It feeds the false and dangerous stereotype of the "unpredictable, two-faced" person, fuels fear and discrimination, and discourages people who are unwell — and their families — from seeking help. Schizophrenia is a treatable medical condition affecting roughly one in a hundred people worldwide; the great majority of those living with it are far more likely to be victims of harm than perpetrators of it. Getting the name right is the first step toward getting the dignity right.
Kurt Schneider and the First-Rank Symptoms
If Kraepelin defined the disorder's boundaries and Bleuler defined its inner character, Kurt Schneider (1887–1967), a German psychiatrist working in the tradition of Karl Jaspers, tried to make it practically diagnosable. Schneider proposed that a particular set of symptoms, while not unique to schizophrenia, were so characteristic that, in the absence of physical brain disease, their presence should carry special diagnostic weight. He called these the "first-rank symptoms" (Symptome ersten Ranges).
The dating here deserves care, because it is often oversimplified. Schneider first set out these ideas in a monograph in the late 1930s, and they appear in his concise classic Klinische Psychopathologie (Clinical Psychopathology), whose German editions date from the 1940s. The first-rank symptoms became internationally famous through the 1959 English translation of that book, which is why they are frequently associated with the 1950s. Saying they emerged "in the 1940s–1950s and became widely known through the 1959 English translation" is the accurate framing.
Schneider's first-rank symptoms include experiences in which the boundary of the self seems breached: hearing voices that argue with one another or keep up a running commentary on one's actions; hearing one's own thoughts spoken aloud; the sense that thoughts are being inserted into, or withdrawn from, one's mind, or broadcast so others can hear them; the feeling that one's impulses, feelings, or movements are being made or controlled by an outside force; and "delusional perception," in which an ordinary perception is suddenly invested with a bizarre private meaning. These symptoms heavily influenced the diagnostic criteria used in the late twentieth century, including early editions of the DSM and the ICD.
Modern psychiatry has tempered Schneider's legacy. Research showed that first-rank symptoms are not specific to schizophrenia — they can occur in bipolar disorder, in dissociative conditions, and elsewhere — so DSM-5 (2013) removed their special diagnostic status. They remain, however, a clinically useful description of the kinds of experience that disturb the sense of self in psychosis, and a landmark in the effort to turn the disorder into something that could be reliably recognized.
Chlorpromazine, 1952: The Treatment Revolution
For the first half of the twentieth century there was no specific medical treatment for schizophrenia. Care meant asylums and a series of drastic and now-abandoned interventions. Everything changed with one drug: chlorpromazine, the first antipsychotic medication, whose introduction in 1952 is rightly described as a revolution in psychiatry.
The story is a model of accidental discovery. Chlorpromazine was synthesized in 1950 by the chemist Paul Charpentier at the French firm Rhône-Poulenc, originally as part of work on antihistamines. The French naval surgeon Henri Laborit noticed that it produced a striking calm, an "artificial hibernation," in surgical patients without simply knocking them out, and he suggested it might have value in psychiatry. Acting on this lead, the psychiatrists Jean Delay and Pierre Deniker at the Sainte-Anne Hospital in Paris gave the drug to psychotic patients and, in 1952, published the first clinical reports of its dramatic effects. It did far more than sedate: agitated, hallucinating, delusional patients became calmer and clearer, and many could engage with the world in ways that had not been possible for years.
To keep the credit accurate: Charpentier synthesized the molecule; Laborit spotted its calming effect and pointed it toward psychiatry; and Delay and Deniker demonstrated and published its antipsychotic action in patients in 1952. The drug reached the market as Largactil in France in 1953 and as Thorazine in the United States in 1954. Its arrival helped launch the era of "deinstitutionalization," in which many people who would once have spent their lives in asylums could instead be treated and live in the community. (That transition was complex and, where community support was inadequate, brought its own serious problems — but the pharmacological breakthrough itself was genuine and transformative.)
Chlorpromazine's importance is not only that it helped patients, but that it opened a scientific door. Researchers naturally asked how a chemical could quiet psychosis — and the pursuit of that question led directly to the first biological theory of schizophrenia's mechanism.
The Dopamine Hypothesis (1960s–1970s)
The most influential biological theory of schizophrenia — the dopamine hypothesis — grew directly out of trying to understand why antipsychotic drugs work. It must be introduced honestly for what it is: a scientific hypothesis, supported by real evidence but incomplete, not a final or sufficient explanation of the illness.
The chain of reasoning unfolded over two decades. In 1963 the Swedish pharmacologist Arvid Carlsson (who later shared the 2000 Nobel Prize for his work on dopamine) and Margit Lindqvist reported that antipsychotic drugs like chlorpromazine and haloperidol increased the turnover of dopamine in the brain, and proposed that the drugs work by blocking dopamine receptors. In 1966 the Dutch pharmacologist Jacques van Rossum made the idea explicit, hypothesizing both that dopamine-receptor blockade explains the drugs' antipsychotic effect and that overactivity of dopamine systems might be part of the cause of schizophrenia itself. Supporting evidence accumulated through the 1970s, including the 1974–1976 finding that the clinical potency of antipsychotic drugs tracks closely with how strongly they block a specific dopamine receptor, the D2 receptor.
The hypothesis explained several observations elegantly: drugs that block dopamine reduce psychotic symptoms, while drugs that boost dopamine (such as amphetamine) can provoke psychotic states in otherwise healthy people. For a time it was the dominant biological account of schizophrenia, and it remains the basis on which most antipsychotic medicines are understood to act.
But — and this honesty is essential on a health page — the simple "too much dopamine" story is now known to be insufficient. Antipsychotics block dopamine within hours yet take weeks to work fully; they help the hallucinations and delusions (the "positive" symptoms) far more than the social withdrawal, flattened emotion, and cognitive difficulties (the "negative" symptoms); and a substantial minority of patients respond poorly. Modern models describe a more nuanced picture — abnormal dopamine signaling concentrated in particular brain pathways, interacting with glutamate and other systems — set within a broad understanding of schizophrenia as a disorder of brain development and connectivity, shaped by many genes and by environmental factors. The dopamine hypothesis was a major, genuine advance; it is one important piece of the explanation, not the whole of it.
From Single Disease to Spectrum: The Modern View
Over the past half-century, thinking about schizophrenia has moved steadily in the direction Bleuler hinted at when he wrote of a "group of schizophrenias." Rather than treating it as one disease with one cause, contemporary psychiatry increasingly understands it as a spectrum of related conditions with overlapping symptoms, varied courses, and many contributing causes. The current diagnostic manual, DSM-5 (2013), formalizes this in its chapter on "Schizophrenia Spectrum and Other Psychotic Disorders," and it abandoned the old practice of sorting patients into rigid subtypes (paranoid, catatonic, hebephrenic/disorganized) because those categories proved unstable and of limited use.
The modern causal picture is genuinely multi-factorial and is best stated without overclaiming. Schizophrenia is strongly heritable — genetics contribute substantially — but it is not caused by any single gene; rather, many genetic variants each add a small amount of risk. On top of this genetic susceptibility, a range of environmental and developmental factors — complications around pregnancy and birth, certain infections or stressors affecting early brain development, social adversity, and heavy cannabis use in vulnerable young people, among others — appear to raise risk. The leading framework is a neurodevelopmental one: subtle differences in how the brain is wired and how its circuits mature, present long before the first obvious symptoms, which then manifest as illness in late adolescence or early adulthood.
Treatment, too, has evolved well beyond that first 1952 breakthrough. Newer "second-generation" antipsychotics arrived from the 1990s with somewhat different effect and side-effect profiles, and clozapine remains uniquely effective for many whose illness resists other drugs. Equally important, medication is now understood to work best alongside psychosocial care — cognitive behavioral therapy for psychosis, family education and support, supported employment, and especially early-intervention services that aim to treat a first episode of psychosis quickly, because earlier help is associated with better long-term outcomes. The arc of the history is from confinement, to a single transformative drug, to comprehensive care for a person.
Stigma, Dignity, and Why the History Matters
The history of schizophrenia is not just a tale of clever doctors and discoveries; it is also a long record of how a misunderstood illness has been feared, sensationalized, and stigmatized — and how getting the facts right pushes back against that. Few medical conditions are so persistently distorted in popular culture, where "schizophrenic" is misused to mean "contradictory" or "two-faced," and where people living with the condition are too often portrayed as dangerous. The reality is that schizophrenia is a treatable brain condition affecting about one person in a hundred, and that those who live with it are, statistically, far more often the victims of violence and neglect than its cause.
This is exactly why the small acts of accuracy throughout this page matter. Insisting that "split mind" means a split within one mind — not multiple personalities — corrects a myth held by most of the public. Distinguishing what Kraepelin observed from what Bleuler renamed, and separating a useful hypothesis (dopamine) from a proven fact, keeps the story honest. Naming the real people behind real discoveries — Kraepelin, Bleuler, Schneider, Charpentier, Laborit, Delay and Deniker, Carlsson, van Rossum — and crediting each for precisely what they did, neither more nor less, is itself a form of respect.
For readers living with schizophrenia, or loving someone who is, the most important message of this history is one of hope grounded in fact. In little more than a century, the condition went from a one-way label of inevitable decline ("dementia praecox") to a treatable, manageable medical illness with medications, therapies, and early-intervention programs that help many people lead full and meaningful lives. Understanding the past — clearly, accurately, and with dignity — is part of how we replace fear with knowledge. This page is a companion to the main Schizophrenia article, which covers current symptoms, diagnosis, and treatment in depth.
Research Papers and References
The references below are peer-reviewed histories and primary-source analyses of how the concept of schizophrenia developed. Citations with a DOI or PMID link to a specific, verified article; the remaining entries are curated PubMed topic searches that open the broader literature. Historical primary texts — Kraepelin's Lehrbuch der Psychiatrie (editions of 1893 and 1899) and Bleuler's Dementia Praecox, oder Gruppe der Schizophrenien (1911) — are named in the article as historical sources rather than as modern citations. Each link opens at the publisher or at PubMed (National Library of Medicine) in a new tab.
- Fusar-Poli P, Politi P. Paul Eugen Bleuler and the birth of schizophrenia (1908). American Journal of Psychiatry. 2008;165(11):1407. — doi:10.1176/appi.ajp.2008.08050714 · PMID 18981075
- Ashok AH, Baugh J, Yeragani VK. Paul Eugen Bleuler and the origin of the term schizophrenia. Indian Journal of Psychiatry. 2012;54(1):95-96. — doi:10.4103/0019-5545.94660 · PMC3339235
- Heckers S, Kendler KS. The evolution of Kraepelin's nosological principles. World Psychiatry. 2020;19(3):381-388. — doi:10.1002/wps.20774 · PMID 32931122
- Adityanjee, Aderibigbe YA, Theodoridis D, Vieweg WV. Dementia praecox to schizophrenia: the first 100 years. Psychiatry and Clinical Neurosciences. 1999;53(4):437-448. — doi:10.1046/j.1440-1819.1999.00584.x · PMID 10498224
- Seeman MV. History of the dopamine hypothesis of antipsychotic action. World Journal of Psychiatry. 2021;11(7):355-365. — doi:10.5498/wjp.v11.i7.355 · PMC8311512
- Hoff P. Kraepelin and degeneration theory. European Archives of Psychiatry and Clinical Neuroscience. 2008;258(Suppl 2):12-17. — doi:10.1007/s00406-008-2002-5
- Emil Kraepelin and the concept of dementia praecox — historical development — PubMed: Kraepelin dementia praecox concept history
- Eugen Bleuler and the concept of schizophrenia — centenary reappraisals — PubMed: Bleuler schizophrenia concept centenary
- Kraepelin's separation of dementia praecox from manic-depressive insanity — PubMed: Kraepelin dichotomy dementia praecox manic-depressive
- Kurt Schneider first-rank symptoms of schizophrenia — history and diagnostic status — PubMed: Schneider first-rank symptoms schizophrenia history
- Chlorpromazine — the first antipsychotic; history, Delay and Deniker, Laborit — PubMed: chlorpromazine history first antipsychotic
- Dopamine hypothesis of schizophrenia — origins, Carlsson, van Rossum, D2 receptor — PubMed: dopamine hypothesis schizophrenia history
- Schizophrenia versus dissociative identity disorder — differential diagnosis and the split-personality misconception — PubMed: schizophrenia vs dissociative identity disorder
- Neurodevelopmental and spectrum models of schizophrenia — modern conceptual history — PubMed: schizophrenia neurodevelopmental spectrum concept
External Authoritative Resources
- NIMH — Schizophrenia (National Institute of Mental Health)
- World Health Organization — Schizophrenia Fact Sheet
- MedlinePlus — Schizophrenia (U.S. National Library of Medicine)
Connections
- Psychiatry
- Schizophrenia (Main Article)
- Bipolar Disorder
- Depression
- Dementia
- PTSD
- OCD
- All Conditions