Loneliness: The Quiet Epidemic With Cardiovascular, Cognitive, and Mortality Consequences
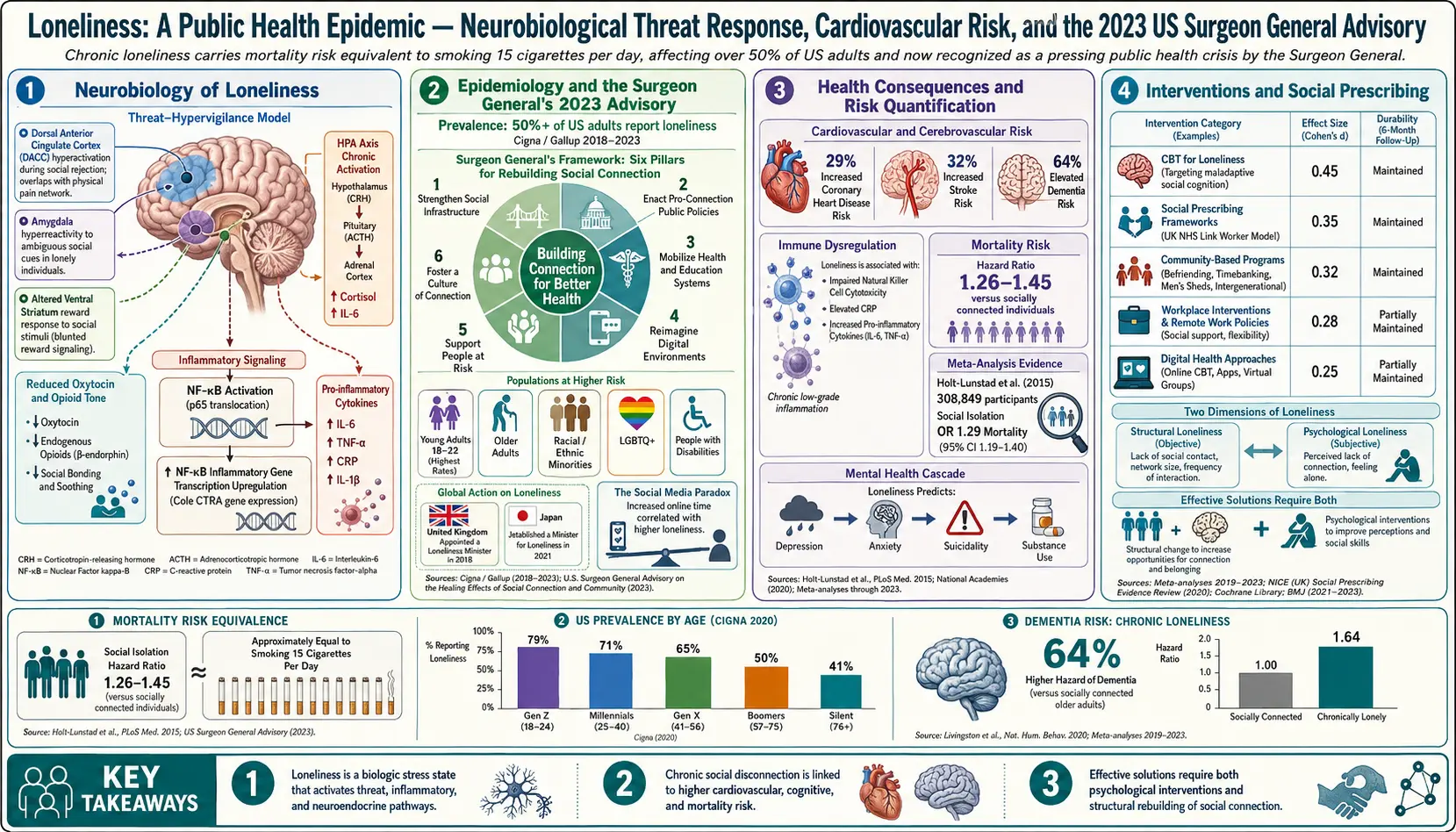
In 2023 the U.S. Surgeon General declared loneliness a public health crisis. Roughly half of American adults report measurable loneliness, and the health consequences rival smoking and obesity: loneliness is associated with a 29% increased risk of coronary heart disease, a 32% increased risk of stroke, a 40 to 50% increased risk of dementia, and a 26% increased risk of premature death. It worsens depression and anxiety, impairs immunity, and fragments sleep.
Loneliness is not simply being alone — many people live alone contentedly, and many surrounded by people feel profoundly lonely. It is the subjective experience of a gap between the social relationships one has and the relationships one wants. This article covers why loneliness drives health outcomes, who is at highest risk, and what actually works to reduce it.
Table of Contents
- What Loneliness Is
- Who Is Most at Risk
- Why Loneliness Harms Health
- How It Is Measured
- Evidence-Based Interventions
- Systemic and Community-Level Changes
- The Role of Technology
- Research Papers
- Connections
- Featured Videos
What Loneliness Is
Loneliness is the discrepancy between desired and actual social connection. Three distinct dimensions:
- Intimate or emotional loneliness — absence of a close confidant or partner.
- Relational loneliness — lack of a network of friends and family.
- Collective loneliness — disconnection from larger community, meaning, or purpose.
A person can be rich in one dimension and impoverished in another.
Who Is Most at Risk
- Young adults (ages 18–25) report the highest rates, contrary to common assumptions about the elderly.
- Older adults living alone, particularly after widowhood.
- People with chronic illness or disability.
- LGBTQ+ individuals, particularly in unsupportive environments.
- Single parents.
- Rural residents with limited mobility.
- New immigrants.
- Remote workers without workplace-based social contact.
- People who recently moved, divorced, retired, or lost a spouse.
Why Loneliness Harms Health
- Chronic inflammation. Lonely individuals show elevated CRP, IL-6, and pro-inflammatory gene expression.
- Hypothalamic-pituitary-adrenal axis dysregulation. Altered cortisol rhythm.
- Sympathetic overactivity. Higher blood pressure, reduced heart-rate variability.
- Reduced immune function and poorer vaccine response.
- Sleep fragmentation.
- Hypervigilance for social threat that paradoxically drives further withdrawal.
- Health behaviors — reduced exercise, poorer diet, increased substance use.
- Neuroplasticity and dementia risk — social engagement is one of the strongest protective factors for cognitive aging.
How It Is Measured
The UCLA Loneliness Scale (20-item or 3-item short form) is the most widely used validated instrument. The de Jong Gierveld Loneliness Scale is another standard. Clinical screening is increasingly recommended in primary care, particularly for older adults and those with chronic illness.
Evidence-Based Interventions
A 2022 meta-analysis by Hickin and colleagues found that interventions targeting maladaptive social cognition — the hypervigilance and self-protective social distortions that loneliness produces — had larger effect sizes than interventions that simply add social contact. The most effective approaches include:
- Cognitive behavioral therapy for loneliness, specifically targeting social threat perception and avoidance.
- Structured social-skills training for adults who have gaps in this area.
- Group-based interventions with shared purpose (book clubs, volunteer groups, classes).
- Intergenerational programs pairing older adults with children or teens — beneficial for both.
- Service and volunteering — meaning-making plus contact.
- Pet companionship has modest but real benefit.
- Social prescribing — a clinician refers to a community-link worker who helps connect the patient to local activities; effective in U.K. NHS models.
Systemic and Community-Level Changes
- Walkable, mixed-use neighborhoods with “third places” — cafés, libraries, community centers.
- Reduced commute times and flexible work arrangements that permit community participation.
- Religious and civic organizations where not aligned with structural harm.
- Accessible transit for older adults.
- Public-health campaigns normalizing help-seeking and reducing stigma.
- Employer investment in genuine workplace community (not performative perks).
The Role of Technology
Technology is a double-edged sword. Passive social-media scrolling correlates with increased loneliness and depressive symptoms in prospective studies; active, reciprocal communication with existing connections correlates with reduced loneliness. Video calls are meaningfully better than text or audio for emotional connection. The principle: use technology to facilitate relationship, not to replace it. Parasocial relationships with podcast hosts or streamers provide some benefit but do not substitute for reciprocal connection.
Research Papers
The PubMed topic searches below return up-to-date peer-reviewed literature for the subjects covered on this page.
- PubMed: loneliness mortality
- PubMed: loneliness cardiovascular disease
- PubMed: loneliness dementia cognitive decline
- PubMed: loneliness inflammation
- PubMed: social isolation immune
- PubMed: loneliness depression
- PubMed: loneliness intervention RCT
- PubMed: loneliness UCLA scale
- PubMed: loneliness cognitive behavioral therapy
- PubMed: loneliness technology social media
- PubMed: loneliness sleep
- PubMed: social prescribing loneliness
Connections
- Dementia
- Depression
- Anxiety
- Cardiovascular Disease
- Burnout
- Grief
- PTSD
- Stress Management
- Sleep Hygiene
- Insomnia
- Natural Anxiety Relief
- Breathwork
- Schizophrenia
- Hearing Loss