Trichinella: Trichinosis from Undercooked Pork, Wild Game, and Bear Meat
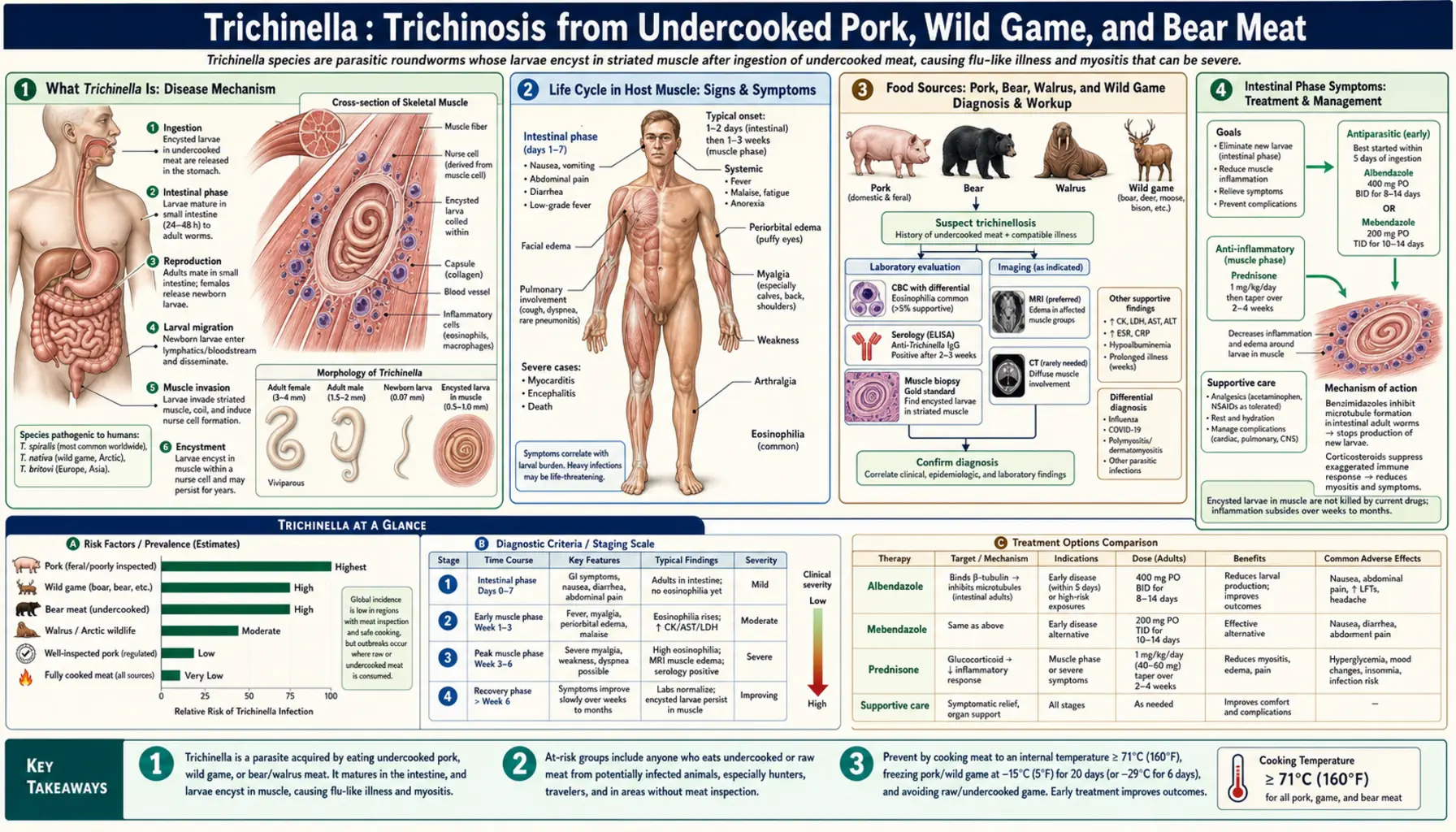
Trichinosis (trichinellosis) is caused by Trichinella roundworms that encyst in muscle tissue after eating undercooked pork or wild game. The disease progresses in two stages: an intestinal phase (diarrhea, nausea, cramping within days of eating infected meat) followed by a painful muscle phase as larvae migrate through the bloodstream and encyst in skeletal muscle — producing periorbital edema (swelling around the eyes), muscle pain and stiffness (myositis), fever, and a striking rise in blood eosinophils. Severe cases involve cardiac muscle inflammation or neurological complications and can be fatal. Cooking meat to a safe internal temperature prevents the disease entirely.
Table of Contents
- What Trichinella Is
- Life Cycle in Host Muscle
- Food Sources: Pork, Bear, Walrus, and Wild Game
- Intestinal Phase Symptoms
- Muscle Phase — Myositis and Periorbital Edema
- Cardiac and Neurological Complications
- Diagnosis
- Treatment
- Prevention — Cooking Temperatures
- Key Research Papers
- Featured Videos
1. What Trichinella Is
Trichinella is a genus of parasitic roundworms (nematodes) with a unique and remarkable biology: unlike most roundworms, which must spend part of their life cycle outside a host in soil or water, Trichinella completes its entire life cycle within a single host animal, alternating between intestinal (adult) and muscle (larval) stages in the same individual. This makes it unlike any other tissue-invasive nematode and explains why eating infected meat — rather than contact with soil or feces — is the only route of human infection.
The genus contains multiple species with slightly different biological properties and host ranges. The most important for human disease are:
- Trichinella spiralis — the most common human pathogen globally. It is primarily maintained in domestic pigs and rats and is found worldwide wherever pigs are raised outside of commercial managed-risk systems. Unlike other species, T. spiralis larvae form a distinctive collagen capsule (a "nurse cell") around themselves inside muscle fibers, providing long-term protection.
- Trichinella nativa — found in Arctic and sub-Arctic wildlife (walrus, polar bear, grizzly bear, sled dogs). It is remarkably freeze-resistant; larvae survive for years in frozen carcasses at −20°C, making frozen wild game an unreliable safety measure in northern communities.
- Trichinella britovi — the main sylvatic species in Europe, infecting wild boar, foxes, and horses. Most European outbreaks have been linked to wild boar meat or horse meat.
- Trichinella pseudospiralis — infects both mammals and birds; uniquely, its larvae do not form a nurse-cell capsule in muscle.
The global burden of trichinellosis has fallen dramatically in countries with regulated commercial pork production, but the disease persists wherever pigs have access to infected carcasses or offal, and wherever wild game is consumed without adequate cooking. Outbreaks in Europe typically trace to wild boar, horse, or bear meat; outbreaks in Arctic communities involve walrus and polar bear.
2. Life Cycle in Host Muscle
The life cycle of Trichinella is entirely intramural — both the intestinal adult stage and the larval stage occur within the same animal. Understanding this two-stage cycle is the key to understanding why the disease produces two waves of illness in humans.
Stage 1 — The intestinal phase: When a person eats meat containing encysted muscle larvae, stomach acid and digestive enzymes dissolve the surrounding nurse-cell capsule (if present), releasing the larvae into the small intestine. Within hours to a couple of days, the larvae undergo four molts and develop into sexually mature adult worms — small, thread-like creatures a few millimeters long that burrow into the lining of the upper small intestine (the jejunum). Male and female worms mate, and beginning roughly five to seven days after infection, female worms begin depositing live larvae directly into intestinal tissue (unlike most roundworms, Trichinella is viviparous — it produces live offspring rather than eggs). A single female can produce hundreds to thousands of newborn larvae over a period of about four to six weeks before the intestinal immune response expels the adult worms.
Stage 2 — The muscle phase (larval migration and encystation): The newborn larvae, each about 0.1 mm long, penetrate the intestinal wall and enter the lymphatic and blood circulations, dispersing throughout the body. They are carried to virtually every organ, but they can only complete their development and encyst in striated (skeletal) muscle fibers. Once a larva reaches a muscle fiber it penetrates it, and over the following three to four weeks the muscle fiber undergoes a radical transformation — its normal contractile machinery is replaced by a specialized structure called the nurse cell, a modified muscle fiber that nurtures and sustains the coiled larva. The nurse cell develops its own dense blood supply, which delivers nutrients directly to the encysted worm. Larvae in the capsule can remain viable and infectious for years to decades in the host's muscle, persisting even after the adult worms in the intestine have been expelled. This is why a person infected years earlier can still transmit the parasite to a predator that eats their flesh — and why freezing carcasses (except for freeze-resistant species like T. nativa) at sufficiently low temperatures for sufficient time is used as a meat safety intervention.
The cycle continues when an animal (or person) eats the infected muscle of another host. In nature, Trichinella circulates among carnivorous and omnivorous wildlife through predation and scavenging; domestic pigs acquire the parasite through contact with infected rodents, wildlife, or contaminated feed.
3. Food Sources: Pork, Bear, Walrus, and Wild Game
Almost all human trichinellosis is acquired by eating raw or undercooked meat. The specific source varies by geography and food culture:
- Pork — historically the dominant source worldwide, and still responsible for many cases in countries where pigs are raised in backyard or free-range systems with exposure to rats and wildlife. Commercial pork production in the United States, Canada, and the European Union has become largely free of Trichinella through regulated biosecurity practices, but home-butchered, free-range, and imported pork remain risk sources.
- Wild boar — the leading source of outbreaks in Europe. Wild boar are not subject to the biosecurity controls applied to commercial pork. Outbreaks linked to wild boar meat have occurred regularly in France, Italy, Spain, Romania, and other European countries, typically involving home-produced or informally distributed meat.
- Bear meat — a major source in North America, Russia, and Eastern Europe. Black bear, grizzly bear, and polar bear are all heavily infected in wild populations, and hunters who eat bear meat without cooking it adequately are at high risk. Bear meat-associated outbreaks in North America have involved hunters and their families. A critical point: smoking, drying, and curing bear meat do not reliably kill Trichinella larvae, so these preservation methods are not safe alternatives to thorough cooking.
- Walrus and other Arctic game — walrus meat is a traditional food in Arctic communities in Alaska, Canada, Russia, and Greenland. Walrus are frequently infected with T. nativa, the freeze-resistant species, which survives traditional preservation methods including freezing in permafrost. Outbreaks among Alaska Native communities have been documented repeatedly. Thorough cooking is the only reliable preventive measure.
- Horse meat — a less intuitive source, since horses are herbivores and do not normally eat meat. Horses can become infected through contaminated feed (for example, feed containing animal byproducts) or by eating carcasses in pastures. Several large outbreaks in France and Italy in the 1970s–1990s were traced to imported horse meat, infecting thousands of people.
- Other wild game — carnivorous and omnivorous wildlife including cougars, foxes, wild cats, and some marine mammals are all potential sources. Any wild carnivore or omnivore is a potential carrier.
Certain preparations that might seem to inactivate larvae actually do not: curing (smoking, salting, drying, air-curing of sausage), microwaving, and freezing domestic pork at household freezer temperatures (−17 to −18°C) for short periods have all been associated with outbreaks because they may not achieve the necessary combination of temperature and time to inactivate all larvae. T. nativa from Arctic wildlife survives indefinitely at these temperatures.
4. Intestinal Phase Symptoms
The intestinal phase of trichinellosis corresponds to the invasion, maturation, and reproduction of adult worms in the small intestinal mucosa. It begins typically one to two days after eating infected meat, though the onset can range from hours (with very heavy exposure) to a week or more (with light infection). Symptoms during this phase are caused by the physical damage and inflammatory response generated by worms burrowing into intestinal tissue.
Common intestinal-phase symptoms include:
- Diarrhea — often the first symptom, which may be watery and frequent. In very heavy infections, it can be severe.
- Nausea and vomiting
- Abdominal cramping and pain — sometimes colicky (coming in waves)
- Fatigue
In lightly infected individuals, the intestinal phase may be mild or entirely absent, and the infection may not be recognized until the muscle phase begins. In heavily infected people, intestinal symptoms can be severe and debilitating. The intestinal phase alone can occasionally cause serious illness; diarrhea from heavy Trichinella infection can lead to significant fluid and electrolyte loss.
The timing is diagnostically important: gastrointestinal illness appearing within a few days of eating pork, wild game, or bear meat, particularly if multiple people who shared the meal are affected, should immediately raise suspicion for trichinellosis. This temporal link is frequently missed because clinicians may not ask about recent consumption of wild game or home-prepared pork.
The intestinal phase begins to ease after three to four weeks as the immune system mounts a response that expels the adult worms from the gut. However, by the time the intestinal phase is resolving, the larval migration phase that causes the more dramatic systemic illness is just beginning.
5. Muscle Phase — Myositis and Periorbital Edema
The muscle phase of trichinellosis is caused by the migration of newborn larvae through the bloodstream and their subsequent invasion and encystation in skeletal muscle. It typically begins two to four weeks after infection and overlaps with, or immediately follows, the intestinal phase. The severity depends directly on the number of larvae encysting per gram of muscle tissue — a function of how heavily infected the meat was and how much of it was consumed.
The hallmark symptoms of the muscle phase are:
- Periorbital edema — swelling around the eyes, one of the most characteristic signs of trichinellosis and a feature that strongly suggests the diagnosis to a physician who recognizes it. It results from larvae encysting in the muscles around the eye and from immune-mediated inflammatory edema. It typically affects both eyes and can be dramatic, sometimes severe enough to nearly close the eyes.
- Myositis (muscle inflammation) — pain, tenderness, and stiffness of skeletal muscles, particularly muscles used in chewing (masseters), swallowing, eye movements, the diaphragm, and limb muscles. Muscle pain is often severe and worsens with movement. The diaphragm is frequently involved, causing pain with deep breathing.
- High fever — often above 39°C (102°F), sometimes with a remittent or undulating pattern. Fever reflects the intense systemic inflammatory response to larval migration.
- Marked eosinophilia — a dramatic rise in blood eosinophil count (often 20–70% of the white cell differential) is one of the most consistent laboratory findings and a key diagnostic clue. Eosinophilia reflects the immune system's response to tissue-invasive parasites.
- Skin rash — a transient rash (petechiae or urticaria) may occur during larval migration.
- Subungual hemorrhages — small splinter hemorrhages visible under the fingernails, caused by larvae migrating through capillaries.
- Fatigue and malaise — profound weakness and exhaustion are almost universal during the muscle phase and can persist for weeks to months after the acute illness resolves.
The muscle phase typically peaks at around three to four weeks and then gradually subsides over several weeks as larvae complete their encystation and the immune response dampens. In most patients with moderate infection, symptoms fully resolve over weeks to a few months. Residual muscle pain or fatigue can persist for months in more heavily infected patients.
In mild infections, the muscle phase may be subclinical — causing only mild muscle soreness that is attributed to other causes. In severe infections involving hundreds or thousands of larvae per gram of muscle, the disease can be life-threatening.
6. Cardiac and Neurological Complications
In severe trichinellosis, migrating larvae can invade tissues other than skeletal muscle, including the heart and brain. Although larvae cannot encyst in smooth muscle or cardiac muscle (because those tissue types do not support nurse-cell formation), they can still pass through and cause significant inflammatory damage. These are the most dangerous manifestations of the disease and account for most trichinellosis fatalities.
Cardiac complications
Cardiac involvement occurs in severe trichinellosis when large numbers of larvae pass through the myocardium (heart muscle) during their migration. The larvae themselves cannot encyst in cardiac tissue, but their passage triggers a local inflammatory response — myocarditis (inflammation of the heart muscle). Manifestations include:
- Tachycardia and arrhythmias — rapid or irregular heart rate is the most common cardiac finding and often the earliest warning sign of cardiac involvement.
- Electrocardiographic changes — ST-segment and T-wave abnormalities resembling those seen in other forms of myocarditis are common findings on ECG during the larval migration phase.
- Congestive heart failure — in the most severe cases, diffuse myocardial inflammation impairs the pumping function of the heart.
- Sudden cardiac death — rare but documented; attributed to fatal arrhythmias arising from inflamed myocardium.
Cardiac manifestations typically appear during the second to fifth week of illness, coinciding with the peak of larval migration. Patients with severe infection should have cardiac monitoring, and any new chest symptoms, palpitations, or shortness of breath in a trichinellosis patient should prompt ECG and cardiac enzyme evaluation.
Neurological complications
Neurological involvement is less common but more varied than cardiac involvement. The mechanisms include direct invasion of neural tissue by migrating larvae, inflammatory edema in the brain and spinal cord, and small-vessel vasculitis caused by larval passage through cerebral blood vessels.
- Headache — common during the larval migration phase, reflecting meningeal irritation or cerebral edema.
- Encephalitis — diffuse brain inflammation, presenting with confusion, altered consciousness, and in severe cases coma.
- Focal neurological deficits — weakness, sensory changes, or visual disturbances, resulting from small cerebral infarcts caused by vasculitis or from focal areas of larval damage.
- Seizures — reported in severe cases with central nervous system involvement.
- Meningitis — cerebrospinal fluid may show elevated protein and eosinophils in patients with meningeal involvement.
Brain imaging (CT or MRI) in patients with neurological trichinellosis may show multiple small enhancing lesions or areas of focal edema. Neurological trichinellosis is associated with the highest mortality of all forms of the disease. Survivors of severe CNS involvement may have lasting cognitive impairment or focal neurological deficits.
7. Diagnosis
Trichinellosis is diagnosed through a combination of clinical features, exposure history, laboratory findings, and specific confirmatory tests. The key elements are:
- Exposure history — a history of eating undercooked pork, wild boar, bear, walrus, horse, or other potentially infected meat is essential. Questioning should specifically ask about recent meals at game dinners, hunting trips, or consumption of home-prepared cured meats. When multiple people who shared a meal develop the same illness, the epidemiological link is highly suggestive.
- Clinical triad — the combination of periorbital edema, myositis, and eosinophilia in a patient with a recent exposure history is nearly diagnostic. No other common illness produces this specific combination.
- Blood tests — eosinophilia is the most consistent finding, often marked (20–70% eosinophils). Elevated creatine kinase (CK) and lactate dehydrogenase (LDH) reflect muscle damage from encysting larvae. A complete blood count, muscle enzyme panel, and liver function tests together provide a useful diagnostic profile.
- Serology — antibody tests against Trichinella antigens (enzyme-linked immunosorbent assay, ELISA; or Western blot for confirmation) become positive two to three weeks after infection. If tested in the intestinal phase (first one to two weeks), serology may be negative; a negative test early in illness does not rule out the diagnosis, and repeat testing is indicated.
- Muscle biopsy — direct demonstration of encysted larvae in a biopsy of a tender skeletal muscle (typically the gastrocnemius or biceps) provides definitive diagnosis. However, biopsy is invasive and usually reserved for cases where serology is negative or the diagnosis is uncertain, or for epidemiological investigation of outbreaks.
- Testing of implicated food — when an outbreak is suspected, laboratory examination of the remaining implicated meat (if available) for Trichinella larvae using the digestion method can confirm the source and identify the species. This is important for public health investigation.
The diagnosis of trichinellosis is often delayed or missed because clinicians in low-prevalence settings do not think of it, because the disease mimics influenza or polymyositis early in its course, and because the classic triad takes two to four weeks to fully develop. Eosinophilia is the key laboratory clue that should prompt the question: has this patient recently eaten undercooked meat?
8. Treatment
Treatment of trichinellosis has two components: antiparasitic drugs to kill the worms, and anti-inflammatory drugs (corticosteroids) to suppress the host inflammatory response that causes much of the serious organ damage. The relative importance of each depends on the stage and severity of illness at the time of diagnosis.
Antiparasitic drugs
- Albendazole is the antiparasitic drug of choice for trichinellosis. It acts by disrupting the parasite's tubulin polymerization, ultimately starving and killing the worm. It is effective against the intestinal adult stage and against newborn larvae during their migration phase; its efficacy against already-encysted larvae in muscle is limited once cyst formation is complete. Treatment during the intestinal phase (within the first two weeks of infection) is most effective — killing the intestinal adult worms before they can produce and release large numbers of larvae prevents or limits the muscle phase. Albendazole taken during the larval migration phase (weeks 2–4) can still reduce disease severity. Once cysts are fully established in muscle, antiparasitic treatment provides less benefit.
- Mebendazole is an alternative antiparasitic with a similar mechanism to albendazole. It was the standard treatment before albendazole became preferred; clinical evidence suggests both are effective, with albendazole having somewhat better bioavailability.
Corticosteroids
- Prednisone or prednisolone (corticosteroids given by mouth) are added for moderate-to-severe trichinellosis to suppress the immune-mediated inflammation that causes myocarditis, encephalitis, and severe myositis. Corticosteroids are particularly important in patients with cardiac or neurological involvement, where inflammatory damage to these organs can be life-threatening. However, they are not given alone without antiparasitic cover, because suppressing inflammation without killing the worms may allow the intestinal adult worms to persist longer and produce more larvae.
Supportive care — adequate hydration, pain management (NSAIDs or analgesics for myalgia), and management of specific complications such as cardiac arrhythmias — complements specific treatment. Hospitalization is required for severe cases with cardiac or neurological involvement. All specific treatment regimens, doses, and durations should be directed by a specialist with experience in parasitic diseases.
9. Prevention — Cooking Temperatures
Trichinellosis is entirely preventable through proper cooking. The parasite has no environmental stage, and no vaccine exists, so cooking is the cornerstone of prevention. The key facts are:
- Cook all meat to safe internal temperatures. For pork, lamb, veal, and game meat (except poultry), the USDA recommends a minimum internal temperature of 145°F (63°C) with a three-minute rest time, which reliably kills Trichinella larvae. For ground meat (including ground pork), the recommended minimum is 160°F (71°C). Poultry should be cooked to 165°F (74°C). These temperatures must be reached at the center of the thickest part of the meat.
- Bear, walrus, and other wild carnivore/omnivore meat should always be fully cooked. For wild game from potential T. nativa sources (Arctic mammals), freezing is not a reliable safety measure — this species survives at standard household freezer temperatures for years. Thorough cooking to a safe internal temperature is the only reliable protection.
- Domestic pork can be rendered safe by freezing — but only under specific conditions not achievable in most household freezers. The USDA provides tables specifying that domestic pork can be made safe by freezing at −15°C (5°F) for 20 days, or at −29°C (−20°F) for 6 days. Household freezers typically operate around −18°C (0°F), which is borderline. Freezing is therefore not recommended as the primary safety measure for wild game because of the freeze-resistant species risk and the difficulty of guaranteeing sufficient time-temperature combinations.
- Curing, smoking, drying, and marinating do not reliably kill Trichinella. Traditional preservation methods that do not involve sufficient heat cannot be relied upon for safety. Home-cured sausage and jerky have been sources of outbreaks.
- Microwave cooking is not reliable unless a calibrated food thermometer confirms that the safe internal temperature has been reached throughout, because microwaves cook unevenly.
- Use a meat thermometer. Color alone (no longer pink) is not a reliable indicator of safe internal temperature for pork, because pork can be safe while still appearing slightly pink, or unsafe while appearing cooked on the outside.
At the industrial scale, commercial pork producers in the United States, Canada, and the EU use Trichinella-controlled compartment systems — feed management to prevent access to rodents and wildlife carcasses, slaughter hygiene, and meat testing — that have effectively eliminated T. spiralis from commercial pork in regulated markets. This is why trichinellosis is now rare in countries with modern food safety systems and primarily a disease associated with wild game, home-butchered pigs, and informally traded meat.
Key Research Papers
Peer-reviewed reviews and studies on Trichinella biology, epidemiology, diagnosis, treatment, and prevention. DOI links open the full citation.
- Gottstein B, Pozio E, Nöckler K. Epidemiology, Diagnosis, Treatment, and Control of Trichinellosis. Clinical Microbiology Reviews. 2009;22(1):127–145.
- Pozio E. Clinical aspects, diagnosis and treatment of trichinellosis. Expert Review of Anti-Infective Therapy. 2003;1(3):471–482.
- Franssen F, Takumi K, Fonville M, et al. Inactivation of Trichinella muscle larvae at different time-temperature heating profiles simulating home-cooking. Experimental Parasitology. 2021;224:108099.
- Purslow PP. Parasitic zoonoses present some risks with low-temperature cooking of pork. Meat Science. 2016;119:14–15.
- Gamble HR, Pozio E, Bruschi F, et al. Trichinella spp. control in modern pork production systems. Food and Waterborne Parasitology. 2022;28:e00172.
Live PubMed Searches
Each link opens a live PubMed query so results stay current as new papers are indexed.
- Trichinella / trichinellosis review
- Trichinellosis diagnosis and eosinophilia
- Trichinellosis myocarditis / cardiac complications
- Trichinellosis neurological complications
- Albendazole treatment for trichinellosis
- Trichinella nativa / Arctic walrus and bear
- Trichinellosis wild boar outbreaks
- Trichinella cooking temperature inactivation
Connections
- All Parasites
- Trichinella Symptoms Overview
- Intestinal Phase Symptoms
- Muscle Invasion and Myositis
- Diagnosis: Serology and Biopsy
- Trichinella Treatments Overview
- Albendazole and Mebendazole
- Corticosteroids for Severe Disease
- Prevention and Food Safety
- Ascaris (Roundworm)
- Pinworm
- Hookworm
- Tapeworm
- Toxoplasma
- Schistosoma
- Leishmania (Leishmaniasis)
- Gastroenterology
- Cardiology
- Neurology
- Infectious Disease
- Pork
- All Conditions