Trichinella Intestinal Phase Symptoms
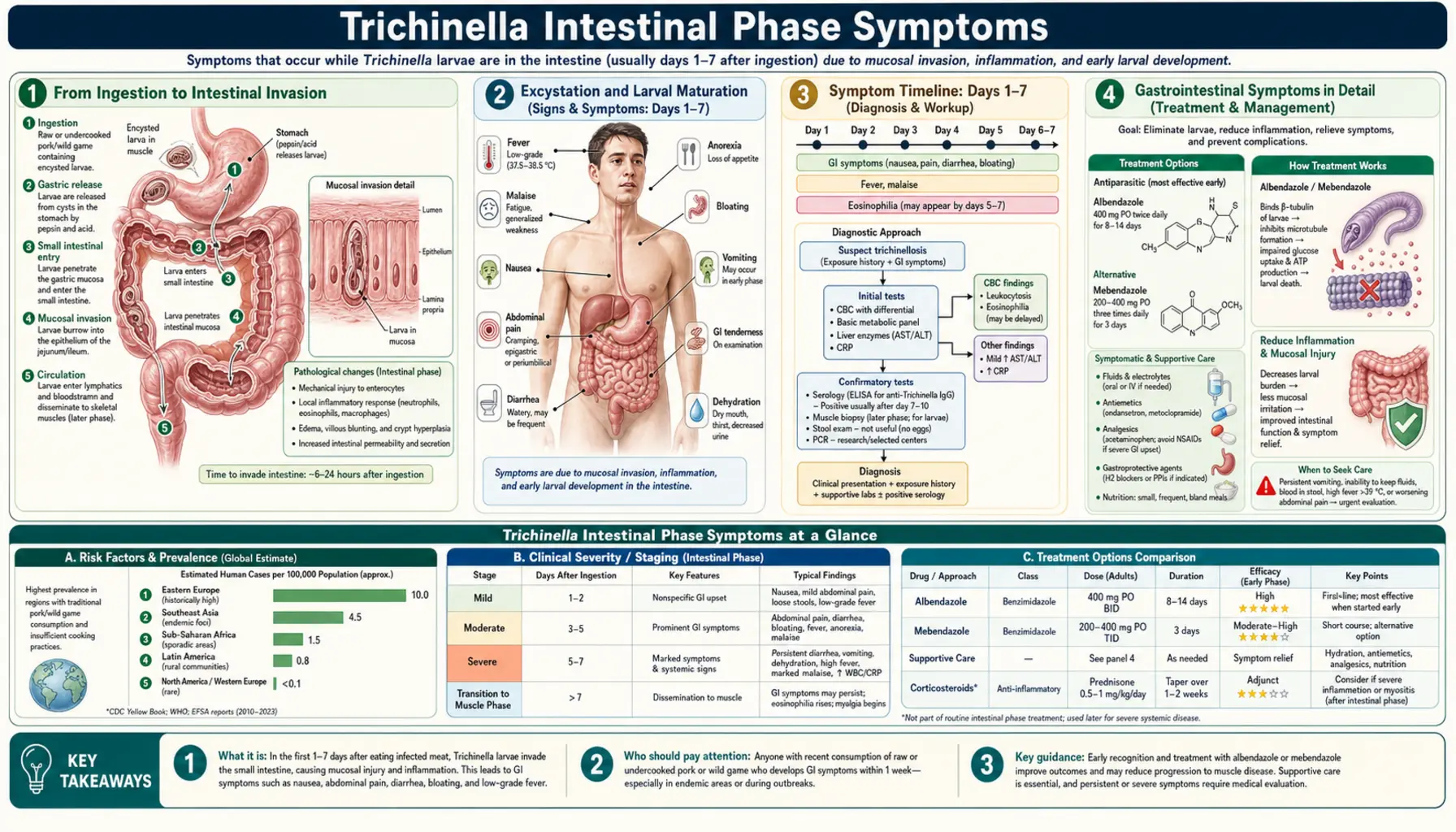
Table of Contents
- From Ingestion to Intestinal Invasion
- Excystation and Larval Maturation
- Symptom Timeline: Days 1–7
- Gastrointestinal Symptoms in Detail
- Early Eosinophilia — A Key Clue
- Larval Production and Intestinal Wall Penetration
- Factors That Determine Intestinal Phase Severity
- Why Antibiotics Don't Help
- How Intestinal Trichinellosis Is Commonly Missed
- Key Research Papers
- Connections
- Featured Videos
1. From Ingestion to Intestinal Invasion
The intestinal phase of trichinellosis begins the moment encysted Trichinella larvae reach the stomach in infected meat. Unlike many foodborne pathogens that attack through toxins or surface adhesion, Trichinella launches a direct biological invasion of the intestinal lining. The process is rapid: within hours of ingestion, the encysted larvae that have survived cooking inadequately are exposed to stomach acid and the enzyme pepsin, which digest the collagen nurse-cell capsule surrounding them.
Once freed from their capsule in the stomach and upper small intestine, the larvae — each roughly 0.1 mm long and already fully formed — are released into the gut lumen. They immediately begin actively moving toward the intestinal wall, where they will spend the next 35–40 days as developing and reproducing adults. The intestinal phase encompasses everything that happens from this point until the adult worms are expelled by the immune response: invasion, development, mating, viviparous larval production, and eventual expulsion of adults by the immune response.
2. Excystation and Larval Maturation
Excystation — the process by which encysted larvae are freed from their protective capsule — is triggered by a combination of stomach acid and digestive enzymes. The collagen capsule of encapsulated species like T. spiralis is enzymatically digested within 1–3 hours. Non-encapsulated species (T. pseudospiralis) lack this capsule and excyst even more rapidly.
Once in the small intestinal lumen, the freed larvae burrow into the columnar epithelium of the jejunum — specifically into the region between the base of the villi and the crypts of Lieberkühn. Inside the epithelium, they undergo four successive molts over approximately 30–40 hours, passing through four larval stages before emerging as sexually mature adult worms. Male adults are 1.4–1.6 mm long; females are larger at 3–4 mm. The time from ingestion to the first adult worms in place is typically 30–38 hours under experimental conditions — remarkably fast for a helminth.
Adult worms embed themselves in the columnar epithelial cells of the small intestine, with their head (anterior end) inserted between cells and their body lying free in the intestinal lumen. This intracellular embedding of the head is unique to Trichinella among intestinal nematodes and is part of what makes the infection resistant to normal gut motility mechanisms that would expel freeliving worms.
3. Symptom Timeline: Days 1–7
The intestinal phase of trichinellosis typically spans the first 1–7 days after eating infected meat, though the onset and duration depend on how many larvae were ingested. In heavy infections, symptoms begin within hours; in light infections, this phase may be entirely unnoticed.
- Hours 6–24: Larvae freed in stomach, beginning excystation. Nausea and mild abdominal discomfort may appear as larvae begin intestinal invasion. In very heavy infections, initial symptoms can appear within 1–2 hours of eating.
- Days 1–2: Adult worms embedding in intestinal epithelium. Nausea, vomiting, and diarrhea begin. Abdominal cramping, often periumbilical or diffuse. Low-grade fever possible.
- Days 3–5: First mating; female worms begin producing live larvae. The intestinal inflammatory response intensifies as the immune system detects the parasite. Diarrhea may worsen. Peripheral eosinophil count begins to rise — this is the earliest laboratory clue and can appear as early as day 2–3 in heavy infections.
- Days 5–7: Active larval production and intestinal wall penetration underway. Newborn larvae entering the bloodstream begin the systemic larval migration phase. The intestinal symptoms may partially overlap with the onset of early systemic symptoms (fatigue, low fever) as larval migration begins.
- Weeks 4–6: Adult worms are gradually expelled from the intestine as the immune response (IgE, mast cells, goblet cell hyperplasia) matures. By this point, the muscle phase is fully established and the intestinal phase symptoms have largely resolved.
4. Gastrointestinal Symptoms in Detail
The gastrointestinal symptoms of trichinellosis's intestinal phase closely resemble those of acute bacterial gastroenteritis or food poisoning, which is the most common reason for misdiagnosis at first presentation. In the absence of a known exposure history (recently eaten wild game or home-prepared pork products), nothing about the intestinal phase is clinically distinctive enough to raise immediate suspicion of a parasitic infection.
Diarrhea: The most common symptom during the intestinal phase, present in 60–75% of patients in outbreaks. It is typically watery and non-bloody, reflecting an inflammatory secretory process in the small intestine rather than colonic invasion. In very heavy infections, diarrhea can be profuse and cause dehydration. The diarrhea usually resolves over 1–2 weeks as the immune response partially controls the infection.
Nausea and vomiting: Common in the first 24–72 hours. Vomiting may eject some adult worms but does not significantly reduce the overall intestinal worm burden.
Abdominal pain and cramping: Periumbilical or diffuse cramping is typical. The pain reflects direct tissue damage from worms embedding in the intestinal epithelium, as well as the inflammatory response in the intestinal mucosa. The pain is often colicky in character.
Fever: Low-grade (37.5–38.5°C / 99.5–101°F) fever is common during the intestinal phase, reflecting the systemic inflammatory response to the developing parasites. High fever is more characteristic of the muscle phase and suggests the larval migration phase has begun.
Fatigue: Non-specific fatigue and malaise often accompany intestinal phase symptoms and may be the first sign that something beyond ordinary food poisoning is occurring.
5. Early Eosinophilia — A Key Clue
Peripheral blood eosinophilia is the single most important laboratory finding in trichinellosis. It is present in virtually all symptomatic patients and typically begins rising in the first few days of infection — sometimes before the muscle phase symptoms become apparent. A complete blood count (CBC) with differential showing marked eosinophilia in a patient with recent gastrointestinal symptoms should immediately prompt questions about meat consumption history.
The normal eosinophil count in peripheral blood is 100–500 cells/μL (roughly 1–4% of the white cell differential). In the intestinal phase of trichinellosis, eosinophils may rise to 1,000–3,000/μL. By the muscle phase they often reach 5,000–20,000/μL or more — sometimes constituting 20–70% of the circulating white blood cells.
Eosinophilia in this context reflects the immune system's recognition of the parasite as a tissue-invasive helminth. Th2-mediated immune responses (interleukin-4, IL-5, IL-13) drive eosinophil production in the bone marrow and mobilization into the tissues as part of the anti-parasitic defense. This mechanism, shared with other invasive helminths (hookworm, Ascaris), is the basis of the general clinical rule: any tissue-invasive helminth infection produces eosinophilia. The absence of eosinophilia makes Trichinella infection extremely unlikely in a symptomatic patient.
6. Larval Production and Intestinal Wall Penetration
After mating (around days 4–5), female adult worms begin the process that drives the systemic disease: viviparous production of live newborn larvae directly into the intestinal tissue. Each female can produce between 500 and 1,500 newborn larvae over her 4–6 week reproductive life. In a moderate infection involving dozens to hundreds of female worms, the total number of larvae released into the body may reach tens to hundreds of thousands.
The newborn larvae, each approximately 0.1 mm long (the same size as the infective muscle larvae that initiated the infection), penetrate the intestinal wall and enter the intestinal lymphatics and mesenteric blood vessels. From there they are carried via the thoracic duct and lymph into the venous circulation, through the right heart, through the pulmonary capillary bed, and then into the systemic arterial circulation — distributing to every tissue in the body.
Larvae reaching tissues other than striated muscle (liver, heart, brain, kidney, lung) cannot complete their development and are eventually destroyed by the inflammatory response — but not before causing significant tissue damage in the process. Only larvae reaching striated skeletal muscle fibers can encyst and complete their development. This muscle tropism is what focuses the major manifestations of the systemic phase on skeletal muscle, the diaphragm, and the muscles of chewing and eye movement.
7. Factors That Determine Intestinal Phase Severity
Not all patients with trichinellosis experience the same intestinal phase. Several biological and individual factors modulate how pronounced the intestinal symptoms are:
- Larval dose ingested: The most important factor. More larvae → more adult worms → more intestinal damage → more pronounced symptoms. Very light infections (fewer than 10 larvae/gram of meat) may cause no intestinal symptoms at all.
- Host immune status: People with prior trichinellosis or those with more robust Th2 immune responses may mount faster immune responses that limit adult worm survival and reproduction — potentially shortening the intestinal phase or limiting larval output.
- Trichinella species: T. spiralis is the most fecund (highest larval output per female) and the most intestinally pathogenic of the common species. T. britovi and T. murrelli generally cause milder intestinal phases.
- Meal composition: Meat eaten with high-fat content may slightly reduce the bioavailability of stomach acid and pepsin, potentially affecting excystation efficiency, though this is a minor factor.
- Anatomical distribution of larvae in the meat: Different muscle groups in the animal have different larval densities. Diaphragm and tongue muscles in pigs typically carry higher larval burdens than limb muscles.
8. Why Antibiotics Don't Help
A critical and frequently misunderstood point about trichinellosis is that antiparasitic drugs — even when effective — work very differently from antibiotics treating bacterial gut infections. Understanding this explains why patients often remain ill even after appropriate antiparasitic treatment begins.
Antiparasitic drugs (albendazole, mebendazole) are effective against intestinal adult worms and against migrating newborn larvae in transit through tissues. However, once larvae have fully encysted in skeletal muscle (which begins around day 15–21 of infection), they are protected inside the nurse-cell capsule, which has a limited blood supply that restricts drug penetration. The nurse cell's collagen capsule also provides physical protection. Even high doses of albendazole have poor penetration into mature muscle cysts, which is why antiparasitic therapy initiated late in the disease (after the muscle cysts are established) has limited benefit in clearing the infection.
Conventional antibiotics (against bacteria) have no effect on Trichinella whatsoever — they target bacterial cell wall synthesis, protein synthesis, or DNA gyrase, none of which are present in eukaryotic parasites. Prescribing antibiotics for what appears to be food poisoning will have no effect on a trichinellosis infection. This is one reason that trichinellosis diagnosed only in the intestinal phase (when it resembles bacterial food poisoning) and treated empirically with antibiotics results in progression to the full muscle phase unnecessarily.
9. How Intestinal Trichinellosis Is Commonly Missed
In low-prevalence settings (the US, Western Europe outside of hunting communities), the intestinal phase of trichinellosis is almost always initially misdiagnosed. Several factors conspire to delay recognition:
- Resembles ordinary food poisoning: Nausea, vomiting, diarrhea, and abdominal cramping within 24–48 hours of eating a meal — this is the textbook presentation of Salmonella, Campylobacter, or norovirus. Without a specific dietary history pointing to wild game or home-processed pork, no clinician will immediately think of Trichinella.
- Dietary history not taken: Physicians in areas where trichinellosis is rare often do not ask about consumption of wild game, bear meat, or home-made pork products. The history of eating at a communal game dinner or a hunting camp meal is the most important diagnostic clue and is frequently not elicited.
- No specific test available in the intestinal phase: Serology (ELISA for anti-Trichinella antibodies) is usually negative for the first 2–3 weeks of infection. Stool examination does not detect Trichinella (the worms live in the intestinal epithelium, not the stool, and do not shed eggs). This means standard gastroenteritis workup gives negative results.
- Cluster recognition gap: When multiple people who shared the same meal all develop gastrointestinal illness simultaneously, this should trigger investigation of the food source. But in household-scale exposures involving only a few people, the cluster may not be recognized.
- Eosinophilia may not be checked: A CBC is not standard in the initial evaluation of what looks like acute gastroenteritis. Ordering a CBC and finding eosinophilia would be the fastest route to correct suspicion in the intestinal phase.
Key Research Papers
Peer-reviewed research on the intestinal phase of trichinellosis, with PubMed links.
- Gottstein B, Pozio E, Nöckler K. Epidemiology, diagnosis, treatment, and control of trichinellosis. Clin Microbiol Rev. 2009;22(1):127–45. PMID 19136437
- Pozio E. World distribution of Trichinella spp. infections in animals and humans. Vet Parasitol. 2007;149(1-2):3–21. — Search PubMed
- Fichi G, Stefanelli S, Pagani P, et al. Trichinellosis outbreak caused by meat from a wild boar. Zoonoses Public Health. 2015;62(4):285–91. — Search PubMed
- Murrell KD, Pozio E. Worldwide occurrence and impact of human trichinellosis. Emerg Infect Dis. 2011;17(12):2194–202. — Search PubMed
- Takumi K, Franssen F, Swart A, et al. Trichinella infections in wildlife in the Netherlands. Parasit Vectors. 2017;10:494. — Search PubMed
- Dupouy-Camet J, Murrell KD (eds). FAO/WHO/OIE Guidelines for Trichinellosis. 2007. — Search PubMed
- Bruschi F, Chiumiento L. Trichinella inflammatory myopathy: host or parasite strategy? Parasit Vectors. 2011;4:42. — Search PubMed
- Pozio E, La Rosa G. Trichinella murrelli n. sp.: etiological agent of sylvatic trichinellosis in temperate areas of North America. J Parasitol. 2000;86(1):134–9. — Search PubMed
- Rostami A, Gamble HR, Dupouy-Camet J, et al. Meat sources of infection for outbreaks of human trichinellosis. Food Microbiol. 2017;64:65–71. — Search PubMed
- Watt G, Silachamroon U. Areas of uncertainty in the management of human trichinellosis. Expert Rev Anti Infect Ther. 2004;2(4):649–52. — Search PubMed
PubMed Topic Searches
- Trichinellosis intestinal phase symptoms
- Trichinella intestinal adult worm biology
- Trichinellosis early eosinophilia diagnosis
- Antiparasitic treatment intestinal phase trichinella
Connections
- All Parasites
- Trichinella Symptoms Overview
- Muscle Invasion and Myositis
- Diagnosis: Serology and Biopsy
- Albendazole and Mebendazole
- Prevention and Food Safety
- Trichinella Overview
- Gastroenterology