Trichinella Symptoms
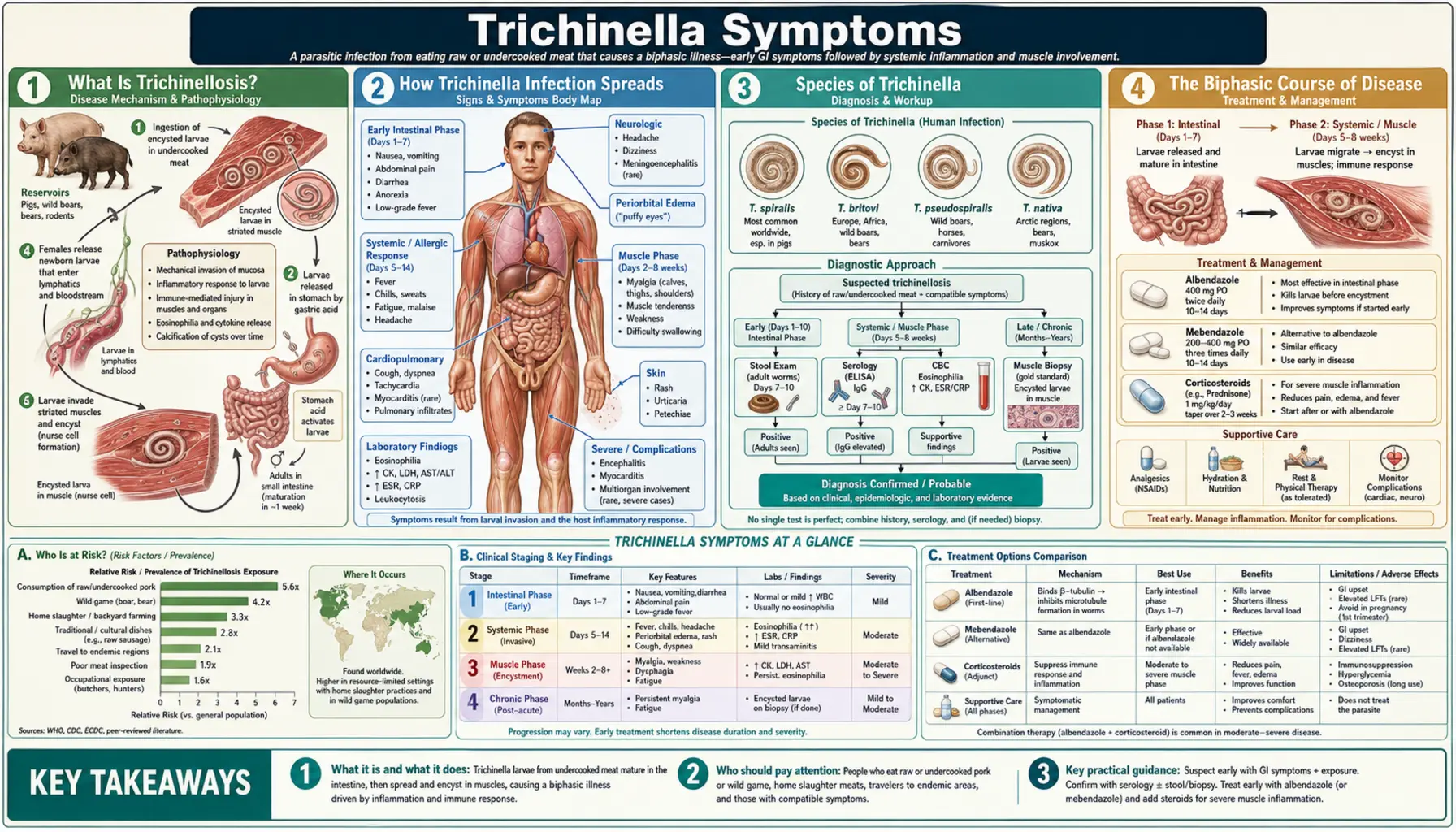
Table of Contents
- What Is Trichinellosis?
- How Trichinella Infection Spreads
- Species of Trichinella
- The Biphasic Course of Disease
- Severity Spectrum
- Global Outbreaks and At-Risk Populations
- Complications Overview
- Prognosis
- Key Research Papers
- Connections
- Featured Videos
1. What Is Trichinellosis?
Trichinellosis (also called trichinosis) is a zoonotic parasitic disease caused by roundworms of the genus Trichinella. Unlike most intestinal parasites, Trichinella completes its entire life cycle within a single host, cycling between an adult intestinal stage and a larval muscle-dwelling stage in the same animal. Humans become infected by eating undercooked meat that contains encysted larvae — most commonly pork, wild boar, bear, walrus, or horse meat. Approximately 11 million people worldwide are estimated to be chronically infected, with hundreds of new outbreak-linked cases reported annually. The disease is notifiable in most countries and is subject to international meat safety regulations.
The name comes from the Greek thrix (hair), referring to the thread-like adult worms. Though globally distributed, the disease burden falls most heavily on communities that consume wild game, home-butchered pork, or traditional cured-meat preparations in regions where food inspection is limited.
2. How Trichinella Infection Spreads
Transmission is exclusively foodborne — there is no person-to-person spread, no environmental stage, and no vector. The entire cycle depends on predation and scavenging within animal populations. When a predator or omnivore eats infected muscle tissue, digestive enzymes release the encysted larvae, which then mature into adult worms in the small intestine, mate, and produce a new generation of larvae that migrate to and encyst in the new host's skeletal muscle.
Key transmission routes to humans:
- Undercooked pork — historically the dominant route globally; commercial pork is now largely Trichinella-free in regulated markets (US, EU, Canada), but backyard and free-range pigs remain a risk.
- Wild boar meat — the leading source of outbreaks in Europe, where wild boar are not subject to commercial biosecurity controls.
- Bear meat — a major source in North America and Russia; North American black bear and grizzly bear carry high larval loads.
- Walrus, polar bear, and Arctic game — primary exposure route in Alaskan Native, Canadian Inuit, and Russian Arctic communities.
- Horse meat — herbivores that can be contaminated through feed containing animal byproducts; responsible for large outbreaks in France and Italy.
- Traditional cured or dried meats — smoking, salting, drying, and air-curing do not reliably kill larvae; home-made sausage from wild game is a documented risk.
3. Species of Trichinella
The genus Trichinella contains at least 12 recognized species and genotypes. They differ in host range, geographic distribution, freeze resistance, and pathogenicity in humans. Understanding species differences matters clinically because some are far more dangerous than others and because certain common food safety measures (freezing) fail against specific species.
- T. spiralis (T1) — the most prevalent human pathogen. Found worldwide in domestic pigs and synanthropic rats. Forms a collagen nurse-cell capsule in skeletal muscle. Sensitive to freezing under controlled conditions. Responsible for the majority of human cases historically.
- T. nativa (T2) — the Arctic/sub-Arctic wildlife species (walrus, polar bear, grizzly bear). Exceptionally freeze-resistant — larvae survive years in frozen carcasses at −20°C. Conventional household freezing is not protective against this species. Responsible for outbreaks in indigenous Arctic communities.
- T. britovi (T3) — the main sylvatic (wildlife) species in Europe and Asia. Infects wild boar, fox, and horse. Most European wild boar outbreaks involve T. britovi. Moderately freeze-resistant.
- T. pseudospiralis (T4) — uniquely infects both mammals and birds. Larvae do not form a capsule (non-encapsulated), making muscle biopsy diagnosis more difficult. Found on multiple continents.
- T. murrelli (T5) — found in North American wildlife (black bear, cougar). Less pathogenic in humans than T. spiralis.
- T. papuae (T10) and T. zimbabwensis (T11) — non-encapsulated species from Papua New Guinea and sub-Saharan Africa; infect reptiles and mammals.
4. The Biphasic Course of Disease
Trichinellosis classically produces two distinct phases of illness that reflect the parasite's two developmental stages inside the human body. Recognizing this biphasic course is essential for timely diagnosis, because the initial gastrointestinal phase is often attributed to food poisoning and the true cause only becomes apparent when the systemic muscle phase begins weeks later.
Phase 1 — Intestinal (enteral) phase (days 1–7 after ingestion): After encysted larvae are ingested and released in the stomach, they migrate to the small intestine (jejunum) and rapidly mature into adult worms over 30–40 hours. The adult worms burrow into intestinal villi and begin mating. Female worms start depositing live larvae (viviparous) into the intestinal mucosa starting around day 5–7. Symptoms during this phase result from intestinal mucosal invasion: nausea, vomiting, diarrhea, abdominal cramping, and low-grade fever. In light infections this phase may be subclinical. Adult worms are expelled from the intestine by the immune response over 4–6 weeks, but by then larval production and migration are already underway.
Phase 2 — Systemic (parenteral) muscle phase (weeks 2–5): Newborn larvae penetrate the intestinal wall, enter the lymphatics and bloodstream, and disperse throughout the body. They survive only in striated (skeletal) muscle fibers, where they encyst over 3–4 weeks and induce transformation of the muscle cell into a specialized "nurse cell" with its own blood supply. The systemic inflammatory response to migrating larvae drives the hallmark symptoms: periorbital edema, myositis, high fever, and a striking eosinophilia. Serious complications — myocarditis, encephalitis — arise during this phase.
5. Severity Spectrum
The severity of trichinellosis depends almost entirely on the larval burden — the number of infectious larvae per gram of ingested meat, how much meat was consumed, and which species is involved. This produces a wide clinical spectrum ranging from entirely subclinical infections to life-threatening disease.
- Subclinical / mild (fewer than ~10 larvae/gram): Most infections worldwide fall into this category, particularly those from partially controlled meat sources. Symptoms may be absent or limited to mild gastrointestinal upset. Periorbital edema and myositis, if present, are mild. The infection is often never diagnosed. Larvae calcify in muscle over years without further consequence.
- Moderate (10–100 larvae/gram): Classic biphasic disease with clearly recognizable intestinal and muscle phases. Periorbital edema, myositis, fever, and marked eosinophilia are present. Patients require treatment and usually recover fully over several weeks to months.
- Severe (100–300+ larvae/gram): Intense systemic inflammation. Severe myositis may impair swallowing (dysphagia), breathing (diaphragmatic involvement), and eye movement. Myocarditis and neurological involvement appear in this range. Hospitalization is required.
- Very severe / fatal (>300 larvae/gram, massive exposure): Multi-organ failure. Death results most commonly from myocarditis (cardiac arrhythmias or heart failure) or encephalitis. Historically, untreated very severe trichinellosis had mortality rates of 5–10%; with modern treatment, mortality is well below 1% in treated patients but approaches 2–3% if severe disease goes untreated.
6. Global Outbreaks and At-Risk Populations
Trichinellosis occurs in isolated cases and in explosive common-source outbreaks. Outbreaks are characteristically linked to a single shared food event — a meal, a gathering, or a batch of home-processed meat — where multiple people are exposed to the same infected product. Cluster recognition is diagnostically important: when several people who shared a wild game meal present with fever, periorbital edema, and eosinophilia within 2–6 weeks of the event, the clinical picture is nearly unmistakable.
Key outbreak settings and populations:
- European wild boar outbreaks: Italy, France, Romania, Bulgaria, Croatia, and other countries report outbreaks linked to home-produced or informally distributed wild boar sausage and other products. Wild boar are not regulated like commercial pigs.
- North American bear meat outbreaks: Hunters and their families are the primary at-risk group. A notable 2020 outbreak in the US involved bear meat jerky that had been shared across multiple states.
- Arctic indigenous communities: Alaska Native and Canadian Inuit communities experience outbreaks linked to walrus, polar bear, and other marine mammals traditionally prepared by fermentation, drying, or freezing — methods that do not kill T. nativa.
- Eastern European home sausage: Home-butchered pigs and traditional raw sausage preparations (bierwurst, salami, sujuk) in Eastern Europe and Central Asia where biosecurity is variable.
- Horse meat outbreaks (historical): Major French and Italian outbreaks in the 1970s–1990s. The risk from horse meat is now better controlled in the EU through mandatory testing.
- Travelers returning from endemic regions: Trichinellosis is a recognized travel-related illness among people who have consumed wild game or local pork in countries where the disease is endemic.
7. Complications Overview
While most patients with trichinellosis recover fully with treatment, severe infections carry the risk of serious, life-threatening complications. These arise primarily during the muscle phase when large numbers of migrating larvae pass through organs that cannot support encystation.
- Myocarditis: Inflammation of the heart muscle from larval transit. Affects 1–3% of recognized cases in outbreaks but is the leading cause of death in fatal trichinellosis. Manifests as tachycardia, ECG changes, elevated troponin, and in severe cases cardiac failure or fatal arrhythmia. See the Muscle Invasion and Myositis page.
- Encephalitis and neurological disease: CNS involvement occurs in severe infections. Confusion, focal deficits, seizures, and coma are reported. Brain imaging may show multiple enhancing lesions or edema. See the Muscle Invasion and Myositis page.
- Pulmonary involvement: Larvae migrating through the pulmonary vasculature can cause pneumonitis; diaphragmatic myositis impairs breathing. Respiratory failure requiring ventilatory support occurs in the most severe cases.
- Ocular complications: Macular hemorrhage (bleeding into the retina) and retinal edema from vascular involvement are rare but vision-threatening.
- Prolonged myalgia and fatigue: Even after the acute phase resolves and larvae have calcified in muscle, some patients experience months to years of residual muscle pain and fatigue — particularly after heavy infections.
8. Prognosis
The prognosis of trichinellosis is strongly dependent on the infecting dose (larval burden), the infecting species, timeliness of diagnosis, and initiation of antiparasitic therapy. With prompt treatment during the intestinal or early muscle phase, the large majority of patients recover fully. Key prognostic factors:
- Larval dose: The most important determinant. Light infections almost always resolve without sequelae. Heavy infections carry a risk of cardiac or neurological complications even with treatment.
- Species: T. spiralis is more pathogenic than T. britovi or T. murrelli; all produce broadly similar disease but with different severity thresholds.
- Timing of treatment: Antiparasitic therapy during the intestinal phase (first 7–14 days) prevents or significantly reduces the muscle phase. Treatment begun during the muscle phase dampens the inflammatory response but cannot remove established muscle cysts.
- Cardiac and CNS involvement: Myocarditis and encephalitis are the most dangerous complications; patients with these require intensive monitoring and are at highest risk of death even with treatment.
- Overall mortality in treated cases: Below 0.2%. Untreated severe disease historically 2–5%, occasionally higher in mass exposures.
- Long-term muscle cysts: Encysted larvae eventually calcify over years and are visible on X-ray. The calcified cysts themselves cause no ongoing disease in the vast majority of patients, though some report persistent localized aching at heavily infected muscle sites.
Key Research Papers
Peer-reviewed research on Trichinella epidemiology, disease course, and outcomes. PMID links open in PubMed.
- Pozio E. World distribution of Trichinella spp. infections in animals and humans. Vet Parasitol. 2007;149(1-2):3–21. — Search PubMed
- Murrell KD, Pozio E. Worldwide occurrence and impact of human trichinellosis, 1986–2009. Emerg Infect Dis. 2011;17(12):2194–202. — Search PubMed
- Gottstein B, Pozio E, Nöckler K. Epidemiology, diagnosis, treatment, and control of trichinellosis. Clin Microbiol Rev. 2009;22(1):127–45. PMID 19136437
- Bruschi F, Murrell KD. New aspects of human trichinellosis. Postgrad Med J. 2002;78(915):15–22. — Search PubMed
- Dupouy-Camet J, Murrell KD (eds). FAO/WHO/OIE Guidelines for the Surveillance, Management, Prevention and Control of Trichinellosis. 2007. — Search PubMed
- Rostami A, Gamble HR, Dupouy-Camet J, et al. Meat sources of infection for outbreaks of human trichinellosis. Food Microbiol. 2017;64:65–71. — Search PubMed
- Pozio E, Darwin Murrell K. Systematics and epidemiology of Trichinella. Adv Parasitol. 2006;63:367–439. — Search PubMed
- Krivokapich SJ, Pozio E, Gatti GM, et al. Trichinella patagoniensis n. sp. in carnivorous mammals from Patagonia, Argentina. Int J Parasitol. 2012;42(10):903–10. — Search PubMed
- Fichi G, Stefanelli S, Pagani P, et al. Trichinellosis outbreak caused by meat from a wild boar hunted in an Italian region. Zoonoses Public Health. 2015;62(4):285–91. — Search PubMed
- Takumi K, Franssen F, Swart A, et al. Trichinella infections in wildlife in the Netherlands. Parasit Vectors. 2017;10:494. — Search PubMed
PubMed Topic Searches
- Trichinellosis epidemiology review
- Trichinellosis outbreaks — wild boar and bear
- Trichinella nativa Arctic freeze-resistance
- Trichinellosis severity and larval burden
Connections
- All Parasites
- Intestinal Phase Symptoms
- Muscle Invasion and Myositis
- Diagnosis: Serology and Muscle Biopsy
- Trichinella Treatments
- Trichinella Overview