Corticosteroids for Severe Trichinellosis
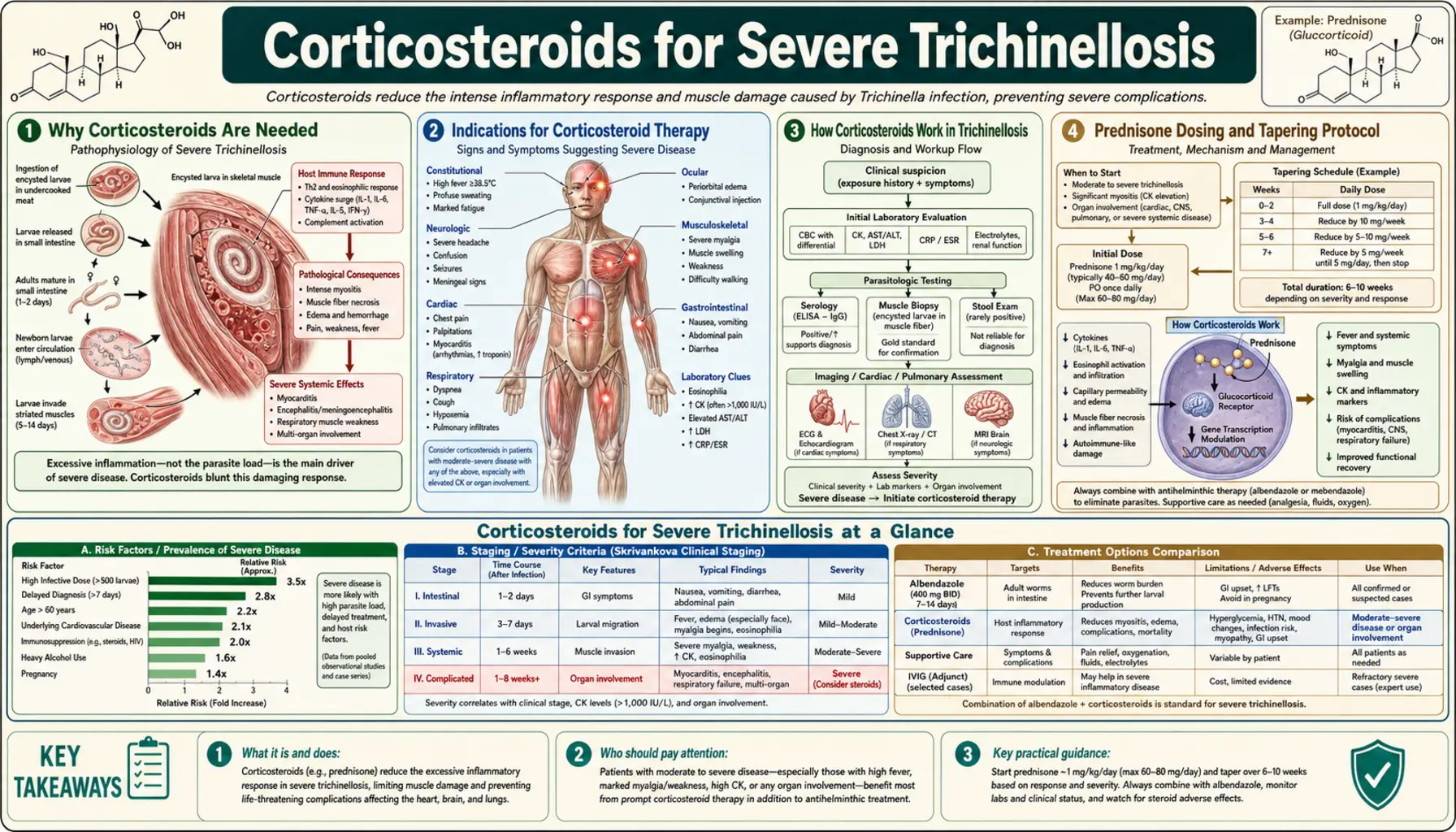
Table of Contents
- Why Corticosteroids Are Needed
- Indications for Corticosteroid Therapy
- How Corticosteroids Work in Trichinellosis
- Prednisone Dosing and Tapering Protocol
- Critical Caution: Never Without Antiparasitics
- Myocarditis Management
- CNS Involvement Management
- Respiratory Compromise
- ICU Indications and Approach
- Prognosis With and Without Treatment
- Key Research Papers
- Connections
- Featured Videos
1. Why Corticosteroids Are Needed
In severe trichinellosis, the most dangerous organ damage — myocarditis, encephalitis, pulmonary inflammation, and profound myositis — is not caused directly by the larvae themselves but by the host's immune response to the migrating and dying larvae. The inflammatory cascade triggered by massive larval invasion of tissues involves eosinophil degranulation, mast cell activation, T-lymphocyte-mediated cytotoxicity, and systemic release of inflammatory cytokines (TNF-α, IL-5, IL-6, interferon-γ). These are powerful defense mechanisms, but in heavy infections they produce so much tissue inflammation that the collateral damage exceeds the benefit — causing heart block, cerebral edema, and respiratory failure.
Corticosteroids interrupt this inflammatory cascade broadly and powerfully. By suppressing multiple arms of the immune response simultaneously, they reduce tissue edema, decrease eosinophil degranulation in heart and brain tissue, and limit the acute injury phase that is responsible for trichinellosis fatalities. The critical trade-off is that the same immune suppression that protects against inflammatory damage may also reduce eosinophil-mediated killing of adult worms and migrating larvae — which is why corticosteroids must always be combined with antiparasitic drugs, not given alone.
2. Indications for Corticosteroid Therapy
Not all patients with trichinellosis require corticosteroids. They are reserved for moderate-to-severe disease with evidence of significant organ involvement. The indications are:
- Severe myositis — myalgia and weakness severe enough to impair breathing (diaphragmatic involvement), swallowing (laryngeal/pharyngeal), or eye movement; profound fatigue limiting any functional activity.
- Myocarditis — any confirmed cardiac involvement: elevated troponin, ST-segment or T-wave changes on ECG, new arrhythmia, reduced ejection fraction on echocardiography, or clinical heart failure.
- CNS involvement — encephalitis (confusion, altered mental status, seizures), focal neurological deficits, or meningitis with cerebrospinal fluid eosinophils.
- Respiratory compromise — hypoxia (oxygen saturation <94% on room air) from diaphragmatic weakness or pulmonary larval migration vasculitis.
- High fever unresponsive to antipyretics with rapidly worsening systemic inflammatory markers in a patient with known heavy exposure.
For mild-to-moderate trichinellosis with periorbital edema, myalgia, and eosinophilia but no organ-threatening complications, antiparasitic drugs and analgesics alone are generally sufficient. The decision to add corticosteroids should be made by an experienced clinician, ideally in consultation with an infectious disease specialist.
3. How Corticosteroids Work in Trichinellosis
Corticosteroids (glucocorticoids) exert their anti-inflammatory effects through multiple mechanisms that are particularly relevant in trichinellosis:
- Eosinophil suppression: Corticosteroids rapidly reduce circulating eosinophil counts and inhibit eosinophil degranulation. This reduces tissue damage from eosinophilic cytotoxic proteins (major basic protein, eosinophil cationic protein) in the myocardium and brain, where eosinophil accumulation around larvae causes direct organ injury.
- Suppression of the cytokine cascade: Corticosteroids block the transcription of pro-inflammatory cytokines (TNF-α, IL-1β, IL-5, IL-6) by binding glucocorticoid receptors and inhibiting NF-κB signaling. This broad cytokine suppression reduces systemic inflammation, fever, and the edematous response in affected tissues.
- Reduction of vascular permeability: Inflammatory edema in the myocardium and brain is driven partly by increased vascular permeability. Corticosteroids stabilize endothelial cells and reduce vascular leak, helping to reverse cerebral edema and myocardial interstitial edema.
- Mast cell and T-cell inhibition: Corticosteroids suppress mast cell degranulation (which contributes to the local vasodilatory and edema-promoting response) and reduce T-lymphocyte proliferation and activation.
The net effect in severe trichinellosis is a rapid reduction in systemic inflammation — typically evidenced by falling fever, improving eosinophil counts, and stabilization of cardiac and neurological status within 24–72 hours of starting high-dose corticosteroids.
4. Prednisone Dosing and Tapering Protocol
The standard corticosteroid used for trichinellosis in most guidelines is oral prednisone (or prednisolone, the active metabolite; equivalent doses). IV methylprednisolone is used when the oral route is not available (impaired swallowing, vomiting, ICU intubation).
Standard dosing for severe trichinellosis:
- Starting dose: 1 mg/kg/day of prednisone, given as a single morning dose or divided twice daily, for 5–7 days. This is the dose used in published outbreak case series and recommended in WHO treatment guidelines.
- Maximum typical starting dose: 60–80 mg/day in adults.
- For myocarditis with impaired cardiac function: some experts use IV methylprednisolone 1–2 mg/kg/day initially to achieve faster therapeutic plasma levels, then transition to oral prednisone once the patient is stabilizing.
Tapering protocol:
- After 5–7 days at the initial dose, taper the dose by 10–20% every 3–5 days over a total course of 2–4 weeks.
- Tapering prevents adrenal insufficiency from abrupt discontinuation and allows gradual reduction of immune suppression as the acute inflammatory phase resolves.
- Monitor clinical status (cardiac, neurological, fever) during the taper; if worsening occurs during dose reduction, return to the previous effective dose and taper more slowly.
During corticosteroid therapy:
- Monitor blood glucose — corticosteroids cause hyperglycemia; diabetic patients require closer glucose monitoring and possible insulin adjustment.
- Monitor blood pressure — corticosteroids cause sodium retention and can raise blood pressure.
- Provide gastric protection (proton pump inhibitor) for patients also taking NSAIDs to reduce peptic ulcer risk.
5. Critical Caution: Never Without Antiparasitics
The most important safety rule in corticosteroid use for trichinellosis is: corticosteroids must never be given without concurrent antiparasitic therapy.
The reason is mechanistic and has been documented in case reports and animal studies. When corticosteroids are administered without an antiparasitic drug:
- Eosinophil-mediated killing of intestinal adult worms is suppressed — adult worms may survive longer and produce more larvae.
- T-cell-mediated clearance of the intestinal worm burden is impaired — the timing of expulsion of adult worms (normally driven by immune pressure) is delayed.
- Migrating larvae encounter less immune resistance in tissues — their transit through the myocardium and brain may be less impeded.
In experimental animals, corticosteroids given without antiparasitics have been shown to increase larval muscle burdens by reducing the immune response that limits larval production. In one documented human case series, patients inadvertently treated with corticosteroids alone (without antiparasitic drugs) in the intestinal phase had more severe subsequent muscle-phase disease than appropriately treated controls.
The clinical rule is always: start albendazole simultaneously with (or before) corticosteroids. Never add corticosteroids to a trichinellosis patient's regimen without confirming that antiparasitic therapy is also in place.
6. Myocarditis Management
Trichinellosis myocarditis requires a systematic management approach targeting both the inflammatory process and its cardiac consequences:
- Cardiac monitoring: Continuous ECG monitoring (telemetry) for patients with confirmed myocarditis, to detect arrhythmias in real time. Daily 12-lead ECGs for stable patients.
- Biomarkers: Serial troponin (I or T) measurements every 12–24 hours during the acute phase to track myocardial injury trajectory — rising troponin indicates ongoing injury; falling troponin confirms recovery.
- Echocardiography: Baseline echo at diagnosis; repeat at 48–72 hours and weekly during the acute phase to assess ejection fraction and wall motion abnormalities. Patients with reduced EF (<50%) require intensification of supportive cardiac management.
- Hemodynamic support: For cardiogenic shock (low output, hypotension), IV inotropic support (dobutamine) and vasopressors as needed, in the ICU.
- Arrhythmia management: Standard antiarrhythmic protocols for specific arrhythmias: beta-blockers for supraventricular tachycardia, amiodarone for refractory ventricular arrhythmias, temporary pacing for high-grade AV block.
- Restrict strenuous activity: All patients with myocarditis should avoid strenuous physical exertion until cardiac function normalizes — typically requiring 3–6 months of follow-up echocardiography in moderate-to-severe cases.
7. CNS Involvement Management
Neurological trichinellosis requires immediate evaluation and aggressive management because CNS complications carry the highest mortality of all manifestations.
- Neuroimaging: CT brain without contrast (rapid, widely available) to detect cerebral edema, hemorrhage, or mass lesions. MRI brain with gadolinium is more sensitive and may show multiple small enhancing lesions in the white matter and periventricular regions characteristic of trichinellosis encephalitis.
- Lumbar puncture: In patients with suspected meningitis (meningismus, photophobia), CSF analysis shows elevated protein, normal or mildly low glucose, and a mixed pleocytosis that may include eosinophils. CSF eosinophils in a patient with heavy meat exposure history is virtually diagnostic.
- Seizure management: Standard antiepileptic drugs (levetiracetam, valproate) for acute seizure control. Patients with trichinellosis encephalitis are at risk for recurrent seizures until cerebral inflammation resolves.
- IV corticosteroids for cerebral edema: High-dose IV dexamethasone (0.15–0.25 mg/kg every 6 hours) or methylprednisolone is often preferred for CNS disease because dexamethasone has excellent CNS penetration and potent anti-edema effect.
- Osmotic therapy: For severe cerebral edema with herniation risk, mannitol or hypertonic saline as bridging measures while corticosteroids reach therapeutic effect.
- Neurological follow-up: Survivors of trichinellosis encephalitis require neuropsychological assessment 3–6 months after recovery to evaluate for persistent cognitive impairment.
8. Respiratory Compromise
Respiratory compromise in trichinellosis arises from two distinct but often concurrent mechanisms: diaphragmatic and intercostal muscle myositis impairing the mechanical pump function of breathing, and pulmonary larval migration vasculitis causing an inflammatory pneumonitis.
- Diaphragmatic myositis: The diaphragm is among the most heavily infected muscles in severe trichinellosis. When severely inflamed, it fails to generate adequate negative inspiratory pressure, producing a restrictive pattern of respiratory failure (reduced tidal volumes, rapid shallow breathing). On spirometry, the FVC is reduced in proportion to the severity of diaphragmatic involvement. This type of respiratory failure responds well to corticosteroids (which reduce diaphragmatic inflammation) and to supportive ventilatory measures.
- Pulmonary involvement: Larval migration through pulmonary arterioles causes local inflammation, potentially producing symptoms of pneumonitis (cough, dyspnea, bilateral infiltrates on chest X-ray).
- Management:
- Supplemental oxygen by nasal cannula or face mask for hypoxia.
- For patients unable to maintain adequate oxygenation and ventilation on supplemental oxygen alone: non-invasive positive pressure ventilation (BiPAP/CPAP) as first-line ventilatory support.
- Mechanical ventilation (intubation) for patients with worsening respiratory failure unresponsive to non-invasive measures. Intubation itself requires careful planning in patients with severe masseter myositis (jaw stiffness may impair laryngoscopy).
- High-dose corticosteroids to reduce diaphragmatic inflammation and pulmonary vasculitis.
9. ICU Indications and Approach
Severe trichinellosis with organ-threatening complications is a critical illness requiring intensive care unit (ICU) management. Indications for ICU admission include:
- Myocarditis with hemodynamic instability (hypotension, shock, reduced ejection fraction)
- Life-threatening arrhythmias requiring continuous monitoring and immediate intervention capability
- Respiratory failure requiring mechanical or non-invasive ventilatory support
- CNS involvement with altered consciousness, seizures, or signs of cerebral herniation
- Multi-organ failure (cardiac + neurological + pulmonary involvement simultaneously)
In the ICU, the management is multidisciplinary:
- Infectious disease: Antiparasitic regimen optimization, treatment duration decisions, interpretation of evolving serologies.
- Cardiology: Management of myocarditis, arrhythmia protocols, hemodynamic monitoring.
- Neurology: Seizure management, neuroimaging interpretation, ICP monitoring if indicated.
- Critical care/pulmonology: Ventilator management, hemodynamic support.
Nutritional support should not be neglected — severe trichinellosis with dysphagia may require parenteral or nasogastric enteral nutrition. Good nutrition is essential to support the energy demands of the inflammatory response and tissue repair.
10. Prognosis With and Without Treatment
The mortality and morbidity of trichinellosis are dramatically different between treated and untreated patients, particularly in severe disease:
- Mortality in treated patients: With appropriate combination of albendazole/mebendazole + corticosteroids + ICU-level supportive care for severe complications, mortality is less than 0.2% even in outbreaks with a proportion of severe cases. Most deaths occur in patients with pre-existing cardiac disease or in those with extreme larval burdens before diagnosis is made.
- Mortality in untreated severe disease: Historically, before effective treatment was available, mortality in trichinellosis outbreaks was 5–10% for recognized cases and likely higher for the heaviest-exposure individuals. In extreme outbreaks (pre-antiparasitic era), mortality rates of 10–30% were reported. Even in the modern era, untreated severe trichinellosis with myocarditis has mortality approaching 2–3%.
- Long-term outcomes in survivors:
- Most patients with mild-to-moderate disease recover fully with no lasting sequelae.
- Patients with severe myocarditis may have residual cardiac dysfunction — reduced ejection fraction or arrhythmias — that requires long-term cardiac follow-up.
- Survivors of encephalitis may have lasting cognitive impairment, personality changes, or focal neurological deficits.
- Calcified muscle cysts persist indefinitely but are clinically silent in most patients; some report localized aching at heavily infected sites.
- Persistent fatigue lasting months to years is reported by a subset of patients after heavy infections, analogous to the post-infectious fatigue seen after other severe inflammatory illnesses.
Key Research Papers
Peer-reviewed research on corticosteroids, myocarditis, and CNS involvement in trichinellosis, with PubMed links.
- Gottstein B, Pozio E, Nöckler K. Epidemiology, diagnosis, treatment, and control of trichinellosis. Clin Microbiol Rev. 2009;22(1):127–45. PMID 19136437
- Watt G, Silachamroon U. Areas of uncertainty in the management of human trichinellosis. Expert Rev Anti Infect Ther. 2004;2(4):649–52. — Search PubMed
- Pozio E. World distribution of Trichinella spp. infections in animals and humans. Vet Parasitol. 2007;149(1-2):3–21. — Search PubMed
- Fourestié V, Douceron H, Brugieres P, et al. Neurotrichinosis: a cerebrovascular disease associated with myocardial injury and hypereosinophilic syndrome. Brain. 1993;116(3):603–16. — Search PubMed
- Murrell KD, Pozio E. Worldwide occurrence and impact of human trichinellosis. Emerg Infect Dis. 2011;17(12):2194–202. — Search PubMed
- Fichi G, Stefanelli S, Pagani P, et al. Trichinellosis outbreak caused by meat from a wild boar. Zoonoses Public Health. 2015;62(4):285–91. — Search PubMed
- Dupouy-Camet J, Murrell KD (eds). FAO/WHO/OIE Guidelines for Trichinellosis. 2007. — Search PubMed
- Takumi K, Franssen F, Swart A, et al. Trichinella infections in wildlife in the Netherlands. Parasit Vectors. 2017;10:494. — Search PubMed
- Bruschi F, Murrell KD. New aspects of human trichinellosis. Postgrad Med J. 2002;78(915):15–22. — Search PubMed
- Rostami A, Gamble HR, Dupouy-Camet J, et al. Meat sources of infection for outbreaks of human trichinellosis. Food Microbiol. 2017;64:65–71. — Search PubMed
PubMed Topic Searches
- Trichinellosis myocarditis corticosteroid treatment
- Trichinellosis encephalitis CNS management
- Trichinellosis respiratory failure diaphragm
- Trichinellosis mortality and prognosis outcomes
Connections
- All Parasites
- Trichinella Treatments Overview
- Albendazole and Mebendazole
- Prevention and Food Safety
- Muscle Invasion and Myositis
- Diagnosis: Serology and Biopsy
- Trichinella Overview
- Cardiology
- Neurology
- Myocarditis — the heart-muscle inflammation corticosteroids are given to control in severe trichinellosis.