Shingles (Herpes Zoster)
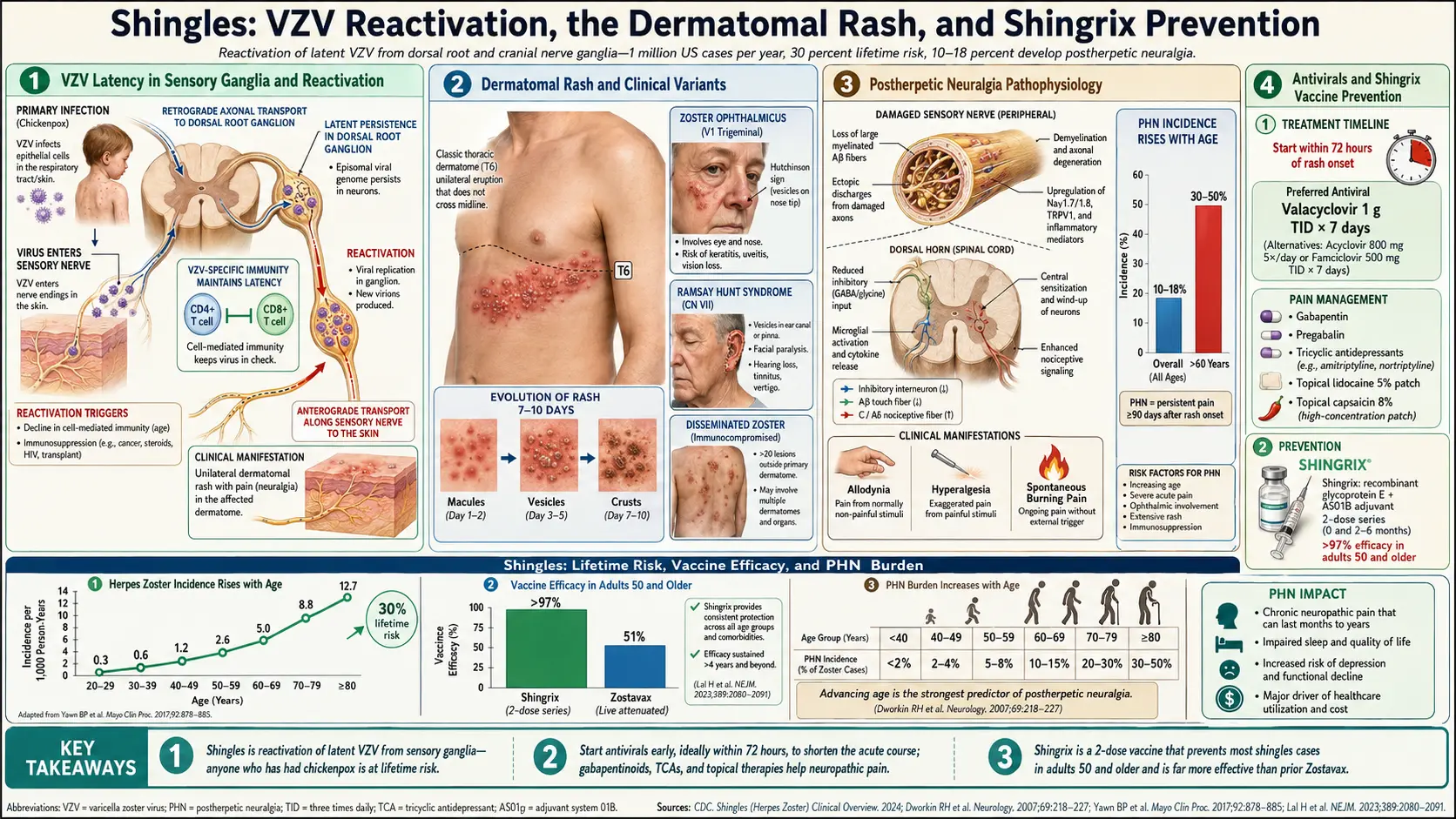
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Recent Research and Advances
- References & Research
- Featured Videos
1. Overview
Shingles, medically known as herpes zoster (HZ), is an acute, painful, vesicular skin eruption caused by the reactivation of the varicella-zoster virus (VZV), a member of the Herpesviridae family (also designated human herpesvirus 3, HHV-3). Following primary infection with VZV, which causes chickenpox (varicella) typically during childhood, the virus establishes lifelong latency in the dorsal root ganglia and cranial nerve ganglia of the sensory nervous system. When cell-mediated immunity wanes — due to aging, immunosuppression, stress, or disease — the virus reactivates, replicates within the ganglion, and travels anterograde along the sensory nerve to the corresponding dermatome, producing the characteristic unilateral, dermatomal vesicular rash accompanied by acute neuralgia.
Herpes zoster is a significant cause of morbidity, particularly in older adults and immunocompromised individuals. The most feared complication is postherpetic neuralgia (PHN), a debilitating chronic neuropathic pain syndrome that persists for months to years after the rash resolves, affecting 10-18% of all herpes zoster patients and up to 30-50% of patients over age 60. Other serious complications include herpes zoster ophthalmicus (involving the ophthalmic division of the trigeminal nerve), Ramsay Hunt syndrome (involving the facial and vestibulocochlear nerves), disseminated herpes zoster, bacterial superinfection, stroke, and meningoencephalitis.
2. Epidemiology
Herpes zoster is a common condition with significant public health impact. In the United States, approximately 1 million cases of herpes zoster occur annually, with an overall incidence of 3-5 per 1,000 person-years. The lifetime risk of developing herpes zoster is approximately 30%, rising to nearly 50% in individuals who live to age 85. Incidence increases sharply with age: approximately 1-2 per 1,000 person-years in adults under 50, rising to 5-7 per 1,000 person-years in adults aged 60-69, and 8-12 per 1,000 person-years in adults over 80.
Women have a slightly higher incidence of herpes zoster than men (1.2-1.3 fold higher risk), though the reasons for this sex disparity are not fully understood. Racial and ethnic differences are observed, with Caucasians having higher incidence rates than African Americans, possibly related to differences in VZV-specific cell-mediated immunity. Herpes zoster incidence has been increasing worldwide over recent decades, with estimated increases of 2-4% per year in many countries.
Immunocompromised patients are at markedly increased risk. HIV-infected individuals have a 12-17 fold increased risk, solid organ transplant recipients have a 2-9 fold increased risk, and patients receiving immunosuppressive therapy (corticosteroids, biologics, JAK inhibitors, chemotherapy) have a 2-5 fold increased risk. Recurrence of herpes zoster occurs in approximately 5-6% of immunocompetent individuals over 8 years and at significantly higher rates in immunocompromised populations. Postherpetic neuralgia occurs in approximately 10-18% of all herpes zoster patients, but the rate rises to 30-50% in patients over age 60 and 60-75% in patients over age 70.
3. Pathophysiology
Primary Infection and Latency
Varicella-zoster virus is a double-stranded DNA virus with a genome of approximately 125,000 base pairs encoding at least 71 open reading frames. Primary infection occurs via respiratory transmission or direct contact with vesicular fluid, with initial viral replication in the nasopharyngeal lymphoid tissue and regional lymph nodes. A primary viremia disseminates VZV to the reticuloendothelial system, followed by a secondary viremia that delivers virus to the skin, producing the generalized vesicular rash of varicella. During primary infection, VZV also undergoes retrograde axonal transport from the skin along sensory nerves to the dorsal root ganglia (DRG) and cranial nerve ganglia, where it establishes lifelong latency.
During latency, VZV resides primarily in neurons (and possibly satellite glial cells) of the sensory ganglia. The viral genome persists as a circular episome in the nucleus, with limited gene expression restricted to a small number of latency-associated transcripts (VLT) and possibly ORF63. VZV-specific cell-mediated immunity (CMI), particularly CD4+ and CD8+ T cells, is essential for maintaining latency and preventing reactivation. Periodic subclinical reactivation events are believed to boost VZV-specific immunity throughout life.
Reactivation Mechanism
When VZV-specific cell-mediated immunity declines below a critical threshold, the virus reactivates within the ganglion. Reactivation involves transition from the latent to the lytic gene expression program, with production of immediate-early (IE), early (E), and late (L) genes leading to full viral replication. The newly produced virions travel anterograde along the sensory nerve axon to the skin of the corresponding dermatome, where they infect epidermal cells and produce the characteristic vesicular rash. Viral replication in the ganglion and along the nerve causes neuronal inflammation, hemorrhagic necrosis, and demyelination of the sensory nerve, which is responsible for the intense pain of acute herpes zoster.
Postherpetic Neuralgia Pathophysiology
Postherpetic neuralgia (PHN) results from persistent neuronal damage caused by VZV replication in the dorsal root ganglion and sensory nerve. The pathological processes include: wallerian degeneration of sensory nerve fibers, dorsal horn atrophy in the spinal cord, loss of large myelinated A-beta fibers (which normally inhibit pain signaling), proliferation of small unmyelinated C fibers that transmit pain, and persistent neuroinflammation with ongoing expression of inflammatory cytokines (IL-6, TNF-alpha) in the affected ganglion. These changes result in peripheral and central sensitization, with altered pain processing including allodynia (pain from normally non-painful stimuli), hyperalgesia (exaggerated pain response), and spontaneous neuropathic pain. The severity of neural damage during the acute phase directly correlates with PHN risk.
4. Etiology and Risk Factors
Primary Cause
- Varicella-zoster virus (VZV/HHV-3) — reactivation of latent virus in sensory ganglia following primary varicella (chickenpox) infection
- Virtually all adults born before 1980 are seropositive for VZV (>99%) and at risk for herpes zoster
- The interval between primary infection and reactivation ranges from years to decades
Age-Related Immune Senescence
- Advanced age — the single most important risk factor; VZV-specific T-cell immunity declines progressively after age 50, with accelerated decline after age 60
- Immunosenescence — age-related decline in thymic output, T-cell diversity, and VZV-specific CD4+ T-cell frequency
- Risk increases approximately 5-fold from age 50 to age 80
Immunosuppressive Conditions
- HIV/AIDS — 12-17 fold increased risk; herpes zoster may be the first clinical manifestation of undiagnosed HIV
- Hematologic malignancies — lymphoma, leukemia, and multiple myeloma (5-8 fold increased risk)
- Solid organ transplant — immunosuppressive regimens increase risk 2-9 fold
- Hematopoietic stem cell transplant — herpes zoster develops in 20-50% of recipients within the first year
- Autoimmune diseases — systemic lupus erythematosus, rheumatoid arthritis, inflammatory bowel disease (both from disease and treatment-related immunosuppression)
Medications
- Systemic corticosteroids — prolonged use (>14 days at doses equivalent to prednisone >15 mg/day)
- Biologic therapies — TNF-alpha inhibitors, anti-CD20 antibodies (rituximab), IL-6 inhibitors
- JAK inhibitors — tofacitinib, baricitinib, upadacitinib (dose-dependent increased risk, 1.5-3 fold)
- Chemotherapy — particularly alkylating agents and purine analogs
- Calcineurin inhibitors — cyclosporine, tacrolimus
- Sphingosine-1-phosphate (S1P) receptor modulators — fingolimod (used in multiple sclerosis)
Other Risk Factors
- Physical trauma — surgery, spinal cord injury, or radiation to the affected dermatome
- Psychological stress — major stressful life events may trigger reactivation
- Female sex — 1.2-1.3 fold higher risk compared to males
- Caucasian race — higher incidence compared to African Americans
- Family history — first-degree relatives with herpes zoster have increased risk, suggesting genetic susceptibility to reactivation
- Diabetes mellitus — modestly increased risk (1.3-1.5 fold)
5. Clinical Presentation
Prodromal Phase
Herpes zoster typically begins with a prodromal phase lasting 1-5 days (range: hours to weeks) before the rash appears. Prodromal symptoms include dermatomal pain (burning, stabbing, throbbing, or shooting), tingling, pruritus, and hyperesthesia in the affected dermatome. The prodromal pain may be severe enough to mimic other conditions — thoracic dermatomal pain may be mistaken for myocardial infarction or pleurisy, lumbar pain for renal colic, and facial pain for dental abscess or migraine. Systemic symptoms including malaise, headache, fever, and fatigue may accompany the prodrome.
Acute Eruption
The characteristic rash evolves through a predictable sequence over 7-10 days:
- Erythematous macules and papules — appear first, clustered within a single dermatome
- Vesicles — develop within 12-24 hours; grouped, clear fluid-filled vesicles on an erythematous base ("dewdrops on a rose petal" appearance)
- Pustules — vesicles become turbid/pustular over 3-4 days
- Crusting — lesions begin to crust over 7-10 days from onset
- Healing — complete crusting and resolution typically within 2-4 weeks; may leave post-inflammatory hyperpigmentation, hypopigmentation, or scarring
The rash is characteristically unilateral and confined to a single dermatome, though a few scattered vesicles outside the primary dermatome are common. The most frequently affected dermatomes are T3-L3 (thoracic and lumbar), accounting for approximately 50-70% of cases, followed by the trigeminal nerve (particularly the ophthalmic division, V1) in 10-20% of cases. Pain during the acute eruption is typically severe, described as burning, electric, lancinating, or deep aching, and is often the most distressing symptom.
Herpes Zoster Ophthalmicus
Herpes zoster ophthalmicus (HZO) involves the ophthalmic division (V1) of the trigeminal nerve and accounts for 10-20% of all herpes zoster cases. Hutchinson's sign — vesicles on the tip or side of the nose (indicating involvement of the nasociliary branch) — predicts ocular involvement in approximately 76% of cases. Ocular complications include keratitis (epithelial and stromal), anterior uveitis, conjunctivitis, scleritis, acute retinal necrosis, secondary glaucoma, and optic neuritis, occurring in 50-72% of HZO patients without antiviral treatment.
Ramsay Hunt Syndrome
Ramsay Hunt syndrome (herpes zoster oticus) results from VZV reactivation in the geniculate ganglion of the facial nerve. The classic triad includes: ipsilateral facial nerve paralysis, vesicular eruption in the ear canal, auricle, or tympanic membrane, and ipsilateral sensorineural hearing loss or vertigo. Additional cranial nerve involvement (V, IX, X) may occur. Ramsay Hunt syndrome produces more severe facial paralysis with a poorer recovery rate (only 50-70% complete recovery) compared to Bell's palsy.
Disseminated Herpes Zoster
In immunocompromised patients, VZV may disseminate hematogenously, producing generalized vesicular eruption (>20 vesicles outside the primary and adjacent dermatomes) resembling varicella. Visceral dissemination to the lungs (pneumonitis), liver (hepatitis), and brain (encephalitis) can occur and is associated with significant mortality.
6. Diagnosis
Clinical Diagnosis
The diagnosis of herpes zoster is primarily clinical, based on the characteristic unilateral, dermatomal, vesicular eruption accompanied by pain. The classic presentation is highly recognizable and laboratory confirmation is not required in typical cases. However, atypical presentations (zoster sine herpete, disseminated disease, immunocompromised hosts) may require laboratory confirmation.
Laboratory Confirmation
- PCR (polymerase chain reaction) — the gold standard for VZV detection; performed on vesicular fluid, crusted lesions, or skin biopsy specimens; sensitivity >95%, specificity approaching 100%; differentiates VZV from HSV
- Direct fluorescent antibody (DFA) testing — rapid immunofluorescence detection of VZV antigens in smears from vesicle bases; sensitivity 80-90%; provides results within hours
- Viral culture — technically possible but impractical due to slow growth (7-14 days), fragility of VZV, and low sensitivity (30-60%)
- Tzanck smear — cytologic examination of vesicle base scrapings showing multinucleated giant cells and viral cytopathic changes; rapid but not specific for VZV (cannot distinguish from HSV); sensitivity approximately 60%
- Serology — VZV-specific IgM or rising IgG titers can support diagnosis but are not recommended for acute diagnosis; useful for confirming prior VZV exposure
CSF Analysis (for CNS Involvement)
In suspected VZV meningitis or encephalitis, cerebrospinal fluid (CSF) analysis shows lymphocytic pleocytosis, elevated protein, and normal glucose. VZV PCR of CSF is the preferred diagnostic test for central nervous system involvement. Intrathecal VZV-specific antibody (anti-VZV IgG index) may be positive even when CSF PCR is negative, particularly in cases of vasculopathy.
Differential Diagnosis
- Herpes simplex virus (HSV) — grouped vesicles, but typically recurrent at the same site; PCR distinguishes HSV from VZV
- Contact dermatitis — may produce dermatomal-appearing vesicular eruption; history of allergen exposure
- Cellulitis or erysipelas — diffuse erythema and swelling without grouped vesicles
- Prodromal herpes zoster pain (before rash) may mimic: myocardial infarction, pleurisy, cholecystitis, renal colic, dental abscess, migraine
- Zoster sine herpete — VZV reactivation producing dermatomal pain without rash; diagnosis requires VZV PCR or serology
7. Treatment
Antiviral Therapy
Antiviral therapy is most effective when initiated within 72 hours of rash onset and is recommended for all patients with herpes zoster, regardless of age or severity. Treatment should also be started after 72 hours if new vesicles are still forming, in immunocompromised patients, in patients with ophthalmic involvement, or in patients at high risk for complications. Recommended antiviral regimens:
- Valacyclovir 1,000 mg three times daily for 7 days — preferred first-line agent due to superior bioavailability (54% vs. 15-30% for acyclovir), convenient dosing, and higher and more sustained plasma levels
- Famciclovir 500 mg three times daily for 7 days — alternative first-line agent; pro-drug of penciclovir with excellent bioavailability (77%)
- Acyclovir 800 mg five times daily for 7 days — effective but requires more frequent dosing and has lower bioavailability; remains first-line for pediatric dosing and intravenous use
- Intravenous acyclovir 10-15 mg/kg every 8 hours for 7-14 days — indicated for disseminated herpes zoster, VZV encephalitis, immunocompromised patients with severe disease, and herpes zoster ophthalmicus with threatened vision
Antiviral therapy reduces the duration and severity of acute pain, accelerates rash healing, decreases viral shedding, and may reduce the incidence and duration of postherpetic neuralgia (though evidence for PHN prevention is modest).
Pain Management: Acute Phase
- Acetaminophen and NSAIDs — first-line for mild-to-moderate pain
- Opioid analgesics — tramadol, oxycodone, or morphine for moderate-to-severe pain; short-term use recommended
- Gabapentin or pregabalin — may be started during acute phase to reduce acute pain and potentially reduce PHN risk
- Short-course corticosteroids — prednisone 60 mg daily tapered over 21 days, given concurrently with antivirals; reduces acute pain and may improve quality of life; does not prevent PHN; contraindicated in immunocompromised patients
- Nerve blocks — sympathetic nerve blocks or epidural anesthesia may be considered for severe refractory acute pain
Treatment of Postherpetic Neuralgia
Treatment of established PHN employs a multimodal approach targeting neuropathic pain mechanisms:
- Gabapentin — FDA-approved for PHN; starting dose 300 mg on day 1, titrated to 1,800-3,600 mg daily in three divided doses; NNT (number needed to treat) for meaningful pain reduction is approximately 6-8
- Pregabalin — FDA-approved for PHN; starting dose 75 mg twice daily, titrated to 150-300 mg twice daily; NNT approximately 4-5
- Tricyclic antidepressants — nortriptyline or amitriptyline 25-150 mg at bedtime; among the most effective options with NNT approximately 3; limited by anticholinergic side effects, particularly in elderly
- Duloxetine — SNRI; 60 mg daily; FDA-approved for neuropathic pain
- Topical lidocaine 5% patch — FDA-approved for PHN; applied to intact skin over the painful area for up to 12 hours daily; well-tolerated with minimal systemic absorption
- Capsaicin 8% patch (Qutenza) — FDA-approved for PHN; single application to the affected area for 60 minutes provides pain relief for up to 3 months; depletes substance P from C-fiber nociceptors
- Opioids — reserved for severe, refractory cases; controlled-release oxycodone, morphine, or tramadol; long-term use carries risks of dependence and adverse effects
Herpes Zoster Ophthalmicus Management
All patients with HZO should receive systemic antiviral therapy and prompt ophthalmologic consultation. Ocular involvement may require topical antiviral drops, topical corticosteroids (for stromal keratitis and uveitis, under ophthalmologic supervision), cycloplegics, and intraocular pressure-lowering agents. Long-term follow-up is essential as ocular complications may develop or recur weeks to months after the acute episode.
8. Complications
- Postherpetic neuralgia (PHN) — the most common complication; chronic neuropathic pain persisting >90 days after rash onset; affects 10-18% of all patients and 30-50% of those over 60; may last months to years; significantly impairs quality of life, sleep, and functional status
- Herpes zoster ophthalmicus complications — keratitis, anterior uveitis, secondary glaucoma, corneal scarring, acute retinal necrosis, optic neuritis; can lead to permanent vision loss if untreated
- Ramsay Hunt syndrome — facial nerve paralysis, hearing loss, vertigo; incomplete recovery in 30-50% of cases
- Bacterial superinfection — secondary infection of vesicular lesions with Staphylococcus aureus or Streptococcus pyogenes; may progress to cellulitis, abscess, or necrotizing fasciitis
- VZV vasculopathy — VZV infection of cerebral arteries causing granulomatous arteritis; risk of ischemic stroke increased 1.3-4.5 fold in the weeks to months following herpes zoster, particularly with ophthalmic involvement
- VZV meningoencephalitis — acute encephalitis with altered mental status, seizures, and focal neurological deficits; mortality 5-10% with treatment
- Myelitis — transverse myelitis or motor neuropathy causing weakness in the affected myotome (zoster paresis); occurs in 1-5% of cases
- Disseminated herpes zoster — generalized skin involvement and potential visceral dissemination (pneumonitis, hepatitis, DIC); primarily in severely immunocompromised patients; mortality up to 5-15%
- Scarring and pigmentary changes — hypertrophic scarring, post-inflammatory hyperpigmentation or hypopigmentation in the affected dermatome
- Chronic neuropathic itch — persistent dermatomal pruritus (notalgia-paresthetica-like) as a variant of post-zoster neuropathy
9. Prognosis
The prognosis of uncomplicated herpes zoster is generally good. In immunocompetent adults, the acute rash resolves within 2-4 weeks, and acute pain typically subsides within 4-6 weeks. However, the risk of postherpetic neuralgia is age-dependent and represents the major source of long-term morbidity. In patients under 50 years old, PHN is uncommon (less than 5%), and the overall prognosis is excellent. In patients aged 60-69, approximately 20-30% develop PHN, and in those over 70, the rate rises to 30-50%. Among patients who develop PHN, approximately 50% experience resolution within one year, but 20-25% have pain persisting beyond one year, and a small proportion suffer for years.
Herpes zoster ophthalmicus has a more guarded prognosis. Without prompt antiviral treatment, ocular complications develop in 50-72% of patients. Even with treatment, 20-30% of HZO patients develop chronic or recurrent ocular inflammation requiring prolonged management. Ramsay Hunt syndrome carries a prognosis worse than idiopathic Bell's palsy, with complete facial nerve recovery in only 50-70% of cases compared to >85% for Bell's palsy.
In immunocompromised patients, the prognosis depends on the degree of immunosuppression and promptness of antiviral therapy. Disseminated herpes zoster carries a mortality rate of 5-15% even with treatment. Early initiation of intravenous acyclovir significantly improves outcomes in severely immunocompromised individuals.
10. Recent Research and Advances
Research in herpes zoster has focused on improving understanding of VZV latency and developing new treatments for postherpetic neuralgia.
Research into VZV latency and reactivation has identified novel latency transcripts, including VZV latency-associated transcript (VLT), which may play a role in maintaining latency or facilitating reactivation. Understanding the molecular switches controlling VZV reactivation could lead to interventions that prevent reactivation rather than treating its consequences.
New treatments for PHN are under investigation. High-concentration capsaicin (8%) patches have demonstrated efficacy equivalent to pregabalin with fewer systemic side effects. Botulinum toxin A injections into the affected dermatome have shown analgesic efficacy in PHN in multiple randomized controlled trials. Anti-NGF (nerve growth factor) antibodies such as tanezumab are being investigated for neuropathic pain conditions including PHN. Novel formulations of existing antivirals with improved CNS penetration are under development to potentially reduce VZV-related neurological complications.
Amenamevir, a helicase-primase inhibitor approved in Japan for herpes zoster, represents a new antiviral class with a mechanism distinct from nucleoside analogs, offering an alternative for acyclovir-resistant VZV strains.
11. References & Research
Historical Background
Herpes zoster has been recognized as a clinical entity for centuries. The name "herpes" derives from the Greek "herpein" (to creep), and "zoster" from the Greek "zone" (girdle or belt), referring to the band-like dermatomal distribution of the rash. The earliest clear descriptions of herpes zoster are attributed to the Persian physician Rhazes (Abu Bakr al-Razi) in the 9th century CE. Richard Bright first suggested the connection between herpes zoster and the sensory ganglia in 1831. The infectious nature of VZV was demonstrated by von Bokay in 1892, who observed that children exposed to herpes zoster patients developed chickenpox, suggesting a common etiological agent. Thomas Weller isolated VZV in cell culture in 1953 and demonstrated that the same virus causes both varicella and herpes zoster. Hope-Simpson published his landmark epidemiological study in 1965, demonstrating the relationship between declining cell-mediated immunity and herpes zoster reactivation.
Key Research Papers
- Cohen JI. Herpes zoster. N Engl J Med. 2013;369(3):255-263.
- Johnson RW, Rice AS. Postherpetic neuralgia. N Engl J Med. 2014;371(16):1526-1533.
- Dworkin RH, Johnson RW, Breuer J, et al. Recommendations for the management of herpes zoster. Clin Infect Dis. 2007;44(Suppl 1):S1-S26.
- Gnann JW Jr, Whitley RJ. Herpes zoster. N Engl J Med. 2002;347(5):340-346.
- Hope-Simpson RE. The nature of herpes zoster: a long-term study and a new hypothesis. Proc R Soc Med. 1965;58(1):9-20.
- Kawai K, Gebremeskel BG, Acosta CJ. Systematic review of incidence and complications of herpes zoster: towards a global perspective. BMJ Open. 2014;4(6):e004833.
- Gilden D, Cohrs RJ, Mahalingam R, Nagel MA. Varicella zoster virus vasculopathies: diverse clinical manifestations, laboratory features, pathogenesis, and treatment. Lancet Neurol. 2009;8(8):731-740.
- Depledge DP, Ouwendijk WJD, Sadaoka T, et al. A spliced latency-associated VZV transcript maps antisense to the viral transactivator gene 61. Nat Commun. 2018;9:1167.
Research Papers
The following PubMed topic searches retrieve current peer-reviewed literature on Shingles (Herpes Zoster). Each link opens a live PubMed query so you always see the most recent publications.
- Herpes zoster shingles review
- Varicella zoster virus reactivation
- Shingrix recombinant zoster vaccine
- Postherpetic neuralgia treatment
- Acyclovir valacyclovir herpes zoster
- Gabapentin postherpetic neuralgia
- Ophthalmic zoster keratitis
- Ramsay Hunt syndrome zoster
- L-lysine herpes virus
- Vitamin D herpes zoster risk
- Zoster immunocompromised antiviral
Connections
- Zinc
- Lysine
- Lemon Balm
- Silver Nanoparticles
- Vitamin C
- Vitamin D3
- Silver Nanoparticles and EBV
- Post-Viral Triggers EBV
- Meningitis
- Cellulitis
- Migraine
- Glaucoma
- Lymphoma
- Lupus
- Diabetes
- Fatigue
- JAK Inhibitors and S1P Modulators
- St Johns Wort
- Herpes Simplex
- Bell's Palsy
- Trigeminal Neuralgia