Insulin Types and Dosing Strategies
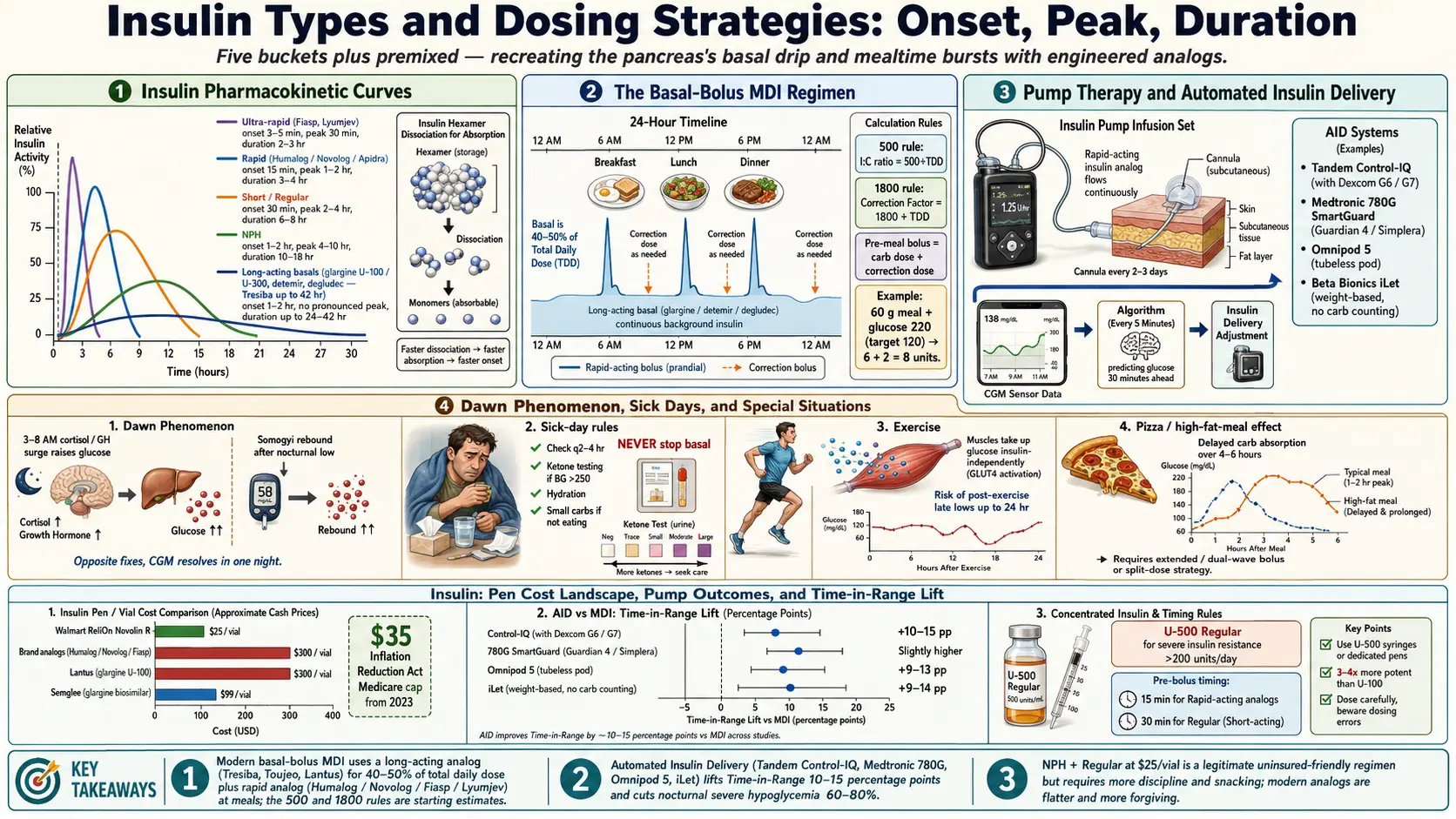
Table of Contents
- Why There Are So Many Insulins
- Rapid-Acting Bolus Insulins
- Ultra-Rapid and Inhaled
- Short-Acting (Regular) Insulin
- Intermediate — NPH
- Long-Acting Basal Insulins
- Premixed Insulins
- Pump-Compatible Insulins
- The Basal-Bolus MDI Regimen
- Pump Therapy and AID Systems
- Carb Counting Basics
- I:C Ratio, Correction Factor, and the 500/1800 Rules
- Basal Dosing and Basal Testing
- Dawn Phenomenon vs Somogyi
- Sick-Day Rules
- Exercise Adjustments
- Hypoglycemia Prevention in Brittle T1D
- Insurance and Cost Realities
- Key Research Papers
- Connections
- Featured Videos
Why There Are So Many Insulins
A healthy pancreas releases insulin in two patterns. There is a slow background drip that runs twenty-four hours a day to keep the liver from dumping too much glucose into the blood, and there are fast bursts at every meal that shove dietary carbohydrate into muscle and fat cells. When you take insulin by injection, you are trying to recreate both of those patterns with products that come out of a vial. No single insulin can do both jobs well — fast and short for meals, slow and flat for background — so pharmaceutical companies have engineered a menu of molecules, each tuned to a different onset and duration. This article walks through every major category, how to choose between them, and how to dose them safely.
If you are new to insulin, the sheer number of names is intimidating. But the logic is simple: everything falls into one of five buckets — ultra-rapid, rapid, short, intermediate, long — plus premixed combinations. Once you understand the onset, peak, and duration of each bucket, the brand names stop mattering and you can speak fluently with your endocrinologist.
Rapid-Acting Bolus Insulins
Rapid-acting analogs are the workhorses of mealtime dosing. They appeared in the 1990s and replaced Regular insulin for most people because they match the speed of a carbohydrate meal far better. Three molecules share nearly identical pharmacology:
- Insulin lispro (Humalog, Admelog biosimilar, Lyumjev ultra-rapid variant).
- Insulin aspart (Novolog, Fiasp faster variant).
- Insulin glulisine (Apidra).
All three have an onset of roughly 15 minutes, a peak between 1 and 2 hours, and a total duration of 3 to 4 hours. In practice that means you inject 10 to 15 minutes before eating (not at the first bite) and the dose is mostly gone by the time you sit down to the next meal. The tail is short enough that stacking — giving a second dose before the first is finished — is less dangerous than with Regular insulin, but it is still the most common cause of unexpected lows.
There is no clinically important difference between Humalog, Novolog, and Apidra for most people. Choice is usually driven by insurance formulary, pump compatibility, or personal response. If one brand gives you site irritation or unpredictable absorption, switching is reasonable.
Ultra-Rapid and Inhaled
Two newer analogs squeeze the onset even shorter. Fiasp (faster-aspart) adds niacinamide to aspart, which speeds absorption. Lyumjev (ultra-rapid lispro) adds treprostinil and citrate, which dilate the capillary bed around the injection and pull the drug into circulation faster. Both have onsets around 3 to 5 minutes, with a peak roughly 30 minutes earlier than the older analogs.
The practical advantage is postprandial control — the 1- and 2-hour glucose after a meal. If your CGM traces show a big spike between eating and the two-hour mark even with pre-bolusing, switching to Fiasp or Lyumjev often flattens that curve. They also shine for people who cannot reliably pre-bolus (toddlers, people with gastroparesis, people who have to eat unpredictably at work).
Afrezza is inhaled human insulin powder. You load a single-use cartridge into a small inhaler and breathe the dose in at the start of a meal. Onset is about 12 minutes, peak 35 to 55 minutes, duration under 3 hours — the fastest clinically available insulin. It suits people who hate needles or want very tight postprandial numbers. Drawbacks: it comes only in 4-, 8-, and 12-unit cartridges (you round to the nearest cartridge), it requires a baseline pulmonary function test before starting, and it is not appropriate for smokers or people with asthma or COPD.
Short-Acting (Regular) Insulin
Regular insulin — also called R, Humulin R, or Novolin R — is plain recombinant human insulin. It has an onset of 30 minutes, peak at 2 to 4 hours, and duration of 6 to 8 hours. For decades it was the only mealtime option. Today it is mostly used for three reasons: cost, high-protein meals, and severe insulin resistance.
For cost: Walmart sells ReliOn Novolin R for about $25 a vial without a prescription in most U.S. states. Compared with $300 for a brand-name analog, that is life-saving for people without insurance, even though it is harder to use.
For high-protein meals: Regular's longer tail actually helps cover the delayed glucose rise from pizza, cheeseburgers, or a big steak dinner — the so-called "pizza effect," where dietary protein and fat slow carbohydrate absorption for hours. Some pump users run a "combo" or "dual-wave" bolus of rapid insulin, but a small dose of Regular in addition to rapid can do the same thing with a pen.
For severe insulin resistance: U-500 Regular insulin (Humulin R U-500) is five times more concentrated than standard U-100. It is reserved for people requiring more than about 200 units per day of total insulin, where U-100 volumes become impractical (imagine injecting 2 mL five times a day). U-500 dosing is a specialist-only territory because the timing and stacking behavior change — it behaves more like an intermediate than a true short-acting insulin.
Intermediate — NPH
NPH (Neutral Protamine Hagedorn) is Regular insulin mixed with a fish-sperm-derived protein that slows its release. Onset is 1 to 2 hours, peak 4 to 10 hours, duration 10 to 18 hours. It is cloudy — you have to roll the vial or pen between your palms to resuspend the crystals before drawing a dose.
NPH is the cheapest basal option — about $25 a vial at Walmart ReliOn — and still the global workhorse outside wealthy countries. The downside is the peak. A 10-hour peak means that if you take NPH at bedtime, you run a real risk of 3 a.m. hypoglycemia, and if you take it at breakfast you may crash in the late afternoon. Variability vial-to-vial and day-to-day is worse than with the true long-acting analogs.
For most insured patients, NPH has been replaced by glargine or degludec. For uninsured patients who cannot afford analogs, NPH plus Regular is a completely legitimate regimen — it is the regimen that kept people alive from the 1950s until the 1990s. It simply requires more discipline, more snacks, and more glucose monitoring.
Long-Acting Basal Insulins
Modern basal insulins are engineered to release at a slow, flat rate for roughly a full day or longer. Five products matter:
- Insulin glargine U-100 (Lantus, Basaglar biosimilar, Semglee interchangeable biosimilar). Onset 1–2 hours, minimal peak, duration about 24 hours. Once-daily dosing in most people, split twice-daily in a minority who run out before 24 hours.
- Insulin glargine U-300 (Toujeo). Same molecule, three times more concentrated. The smaller injection depot releases even more slowly, giving a flatter profile and duration up to 36 hours. Less hypoglycemia than U-100 in head-to-head trials.
- Insulin detemir (Levemir). Binds reversibly to albumin in the blood, which smooths absorption. Often used twice daily because its duration is closer to 18–22 hours. Popular in pregnancy because of its safety data.
- Insulin degludec (Tresiba). Forms multi-hexamer chains at the injection site that slowly release monomers for up to 42 hours. Effectively impossible to overdose within a single day — if you skip a dose by 8 hours, your next injection simply resumes steady state. The flattest, most forgiving basal on the market. Lower nocturnal hypoglycemia than glargine U-100 in the SWITCH trials.
The practical question most patients ask is: "Does it matter which one I am on?" For a person whose numbers are stable on Lantus or Basaglar, it does not matter. For a person waking up low at 3 a.m. despite careful dosing, switching to Toujeo or Tresiba often fixes it. For a person who works rotating shifts or travels across time zones, Tresiba's flatness is a real quality-of-life gain.
Premixed Insulins
Premixed insulins combine a basal and a bolus in one pen. Common ratios:
- 70/30 — 70% NPH + 30% Regular (Humulin 70/30, Novolin 70/30), or 70% aspart protamine + 30% aspart (Novolog Mix 70/30).
- 75/25 — 75% lispro protamine + 25% lispro (Humalog Mix 75/25).
- 50/50 — half-and-half for people with larger meal boluses.
Premixed regimens are usually twice daily, before breakfast and before dinner. They are simpler than basal-bolus — two injections instead of five — and they suit people with steady schedules and steady meal sizes: older adults, people with cognitive impairment, people whose caregivers do the dosing. The trade-off is flexibility. You cannot separately adjust the basal when you are sick or the bolus when you skip a meal. For type 1 diabetes, premixed is generally not adequate. For stable type 2, it can be an excellent pragmatic choice.
Pump-Compatible Insulins
Insulin pumps deliver continuous subcutaneous infusion through a small cannula you change every 2 to 3 days. Only rapid-acting analogs are used in pumps: Humalog, Novolog, Fiasp, and Lyumjev. Apidra is FDA-approved for pump use but tends to crystallize in tubing over 48 hours and is less popular. Regular insulin is not used in modern pumps because its long tail destroys the math of automated dosing.
Some pump users prefer Fiasp or Lyumjev for the faster meal response; others find the ultra-rapid formulations more likely to cause infusion-set irritation and stick with Humalog or Novolog. This is an individual trial.
The Basal-Bolus MDI Regimen
MDI means multiple daily injections. It is the gold-standard regimen for type 1 diabetes when not using a pump, and an excellent regimen for insulin-requiring type 2. The structure is:
- Long-acting basal once daily (Lantus, Basaglar, Semglee, Toujeo, Tresiba) or twice daily (Levemir). Usually 40–50% of total daily dose.
- Rapid-acting bolus before each meal. Dose = (carbs ÷ I:C ratio) + (correction for high glucose).
- Correction doses between meals for out-of-range highs, using the same rapid-acting insulin.
Four to five injections a day sounds like a lot until you realize that the pen needle is 4 mm long and thinner than a human hair. Most patients describe the injections as painless within two weeks. The tight glucose control that basal-bolus enables is worth the learning curve.
Pump Therapy and AID Systems
An insulin pump replaces the basal insulin (with a programmable micro-drip of rapid insulin delivered every few minutes) and replaces mealtime pens (you push buttons instead). Since about 2020, pumps have evolved into automated insulin delivery (AID) systems — also called hybrid closed-loop systems — that read your continuous glucose monitor (CGM) in real time and adjust the basal rate minute-by-minute.
The current commercial options in the U.S.:
- Tandem t:slim X2 with Control-IQ — pairs with Dexcom G6 or G7. Adjusts basal every 5 minutes, delivers automatic correction boluses once an hour if glucose is trending high.
- Medtronic MiniMed 780G — pairs with Guardian 4 or Simplera CGM. Auto-corrects every 5 minutes, including micro-boluses.
- Omnipod 5 — tubeless, disposable 3-day pod. Pairs with Dexcom G6/G7 or Libre 2 Plus. Adjusts basal by a personalized target glucose.
- Beta Bionics iLet (Bionic Pancreas) — dosing algorithm is weight-based only, with no carb counting required. User announces meals as "usual, less, or more" and the pump estimates the dose.
AID systems reliably lift time-in-range (70–180 mg/dL) by 10 to 20 percentage points compared with MDI in most studies, with less nocturnal hypoglycemia. They are not magic — you still bolus for meals (except on iLet), still change sites, still replace CGM sensors — but they dramatically reduce the mental load of T1D.
Carb Counting Basics
Carb counting means measuring the grams of carbohydrate in each meal so you can calculate the correct bolus. In practice you use three tools in combination:
- Nutrition labels. Look at "Total Carbohydrate" (not "net carbs" and not "sugars"). Subtract fiber only if you use the net-carb approach your educator taught you. Multiply by the serving size you actually ate.
- Apps. MyFitnessPal has the largest crowd-sourced database but accuracy is uneven. CalorieKing is the gold standard for restaurant and packaged foods. Carb Manager skews toward low-carb and keto users. Figwee uses photo portion estimates.
- Restaurant disclosure. U.S. chains with more than 20 locations are federally required to publish calorie and often carbohydrate counts. Grab the printed menu or their website before you order.
Protein and fat matter too. A pure-carb meal (toast with jam) hits the bloodstream within 30 minutes. A high-fat, high-protein meal (pizza, lasagna, cheeseburger and fries) releases glucose over 4 to 6 hours — the pizza effect. Pump users handle this with extended or combo boluses. MDI users either split the bolus (half before the meal, half at the 90-minute mark) or add a small dose of Regular insulin. Every T1D eventually learns which foods do this to them. Dinner leftovers for lunch usually behave differently than the same food fresh — another quirk to log.
I:C Ratio, Correction Factor, and the 500/1800 Rules
Two numbers drive every bolus calculation:
Insulin-to-carb ratio (I:C) is how many grams of carbohydrate one unit of rapid insulin covers. If your I:C is 1:10, you take 1 unit per 10 grams of carb. A 60-gram meal = 6 units.
The classic starting estimate is the 500 rule: divide 500 by your total daily dose (TDD) of insulin. If you take 50 units a day total, your I:C is about 500 ÷ 50 = 10, so 1 unit per 10 g carb. For Regular insulin instead of rapid, use the 450 rule.
Correction factor (CF), also called insulin sensitivity factor (ISF), is how much one unit of rapid insulin will drop your glucose. If your CF is 50, one unit lowers blood sugar by 50 mg/dL. A reading of 220 with a target of 120 means a 100-point drop needed = 2 units of correction.
Starting estimate: the 1800 rule (some endocrinologists use 1700). Divide 1800 by your TDD. For a 50-unit-per-day person: 1800 ÷ 50 = 36 mg/dL per unit.
A pre-meal dose is the sum: carb dose + correction dose. If your meal has 60 g carb and your pre-meal glucose is 220 with a target of 120, you give 6 + 2 = 8 units.
These are starting points. Real I:C and CF vary by time of day — most people are more insulin-resistant in the morning — by menstrual cycle, by exercise, by illness, and by stress. Pumps let you program three or four different ratios across the day. MDI users can simply note that, say, breakfast needs 1:8 while dinner needs 1:12.
Basal Dosing and Basal Testing
Basal insulin should cover your glucose between meals without pushing you low. The usual split is 40 to 50% of total daily dose as basal, with the rest as mealtime bolus. For a 50-unit-per-day person that means roughly 20 to 25 units of long-acting.
To confirm the basal dose is right, endocrinologists use basal testing. The method: skip a meal (say, lunch), do not bolus, and check glucose every 2 to 3 hours for the next 6 hours. If glucose stays flat within about 30 mg/dL of starting, your basal in that window is correct. If it drifts up, basal is too low. If it drifts down, basal is too high. Repeat across breakfast, lunch, and dinner windows on different days to map the whole 24-hour profile. CGM users can do this passively by scanning the CGM line during accidental skipped meals.
Adjust no faster than 10% every 3 days. Basal insulins take 3 to 5 days to reach a new steady state, so faster adjustments chase ghosts.
Dawn Phenomenon vs Somogyi
Many people with diabetes wake up with higher glucose than they went to bed with. The two classic explanations:
- Dawn phenomenon. Between 3 and 8 a.m., cortisol and growth hormone rise to prepare the body for waking. These hormones push the liver to release glucose and reduce insulin sensitivity. Most people — diabetic or not — have this surge; in diabetes it simply is not absorbed. A CGM trace shows a smooth upward curve from about 3 a.m. onward. Fix: bump basal slightly, move the basal injection from evening to morning, or use a pump with a higher overnight basal rate.
- Somogyi effect (rebound hyperglycemia). A nocturnal low around 2–3 a.m. triggers counter-regulatory hormones that overshoot, leaving you high by 7 a.m. CGM shows a dip before the rise. Fix: lower the basal dose. This is the opposite treatment from dawn phenomenon and why guessing is dangerous.
Somogyi is much rarer than it used to be thought — modern CGM data suggest dawn phenomenon accounts for the vast majority of morning highs. But the distinction matters because the two conditions need opposite adjustments. CGM answers the question in one night.
Sick-Day Rules
Infections, fevers, vomiting, and surgery all push glucose up and, in type 1 diabetes, can push ketones up fast. Core sick-day principles:
- Never stop basal insulin. Even if you cannot eat, your liver is still releasing glucose and your body still needs basal coverage. Stopping basal during a stomach bug is the classic path to DKA.
- Increase checks. Glucose every 2 to 4 hours, around the clock. CGM covers this automatically.
- Check ketones. Use urine ketone strips (Ketostix, about $10 for 50) or, better, a blood beta-hydroxybutyrate meter (Precision Xtra or Keto-Mojo GK+). Blood ketone readings are real-time; urine readings lag by hours. Any ketones above trace while sick need action.
- Bump basal for fever. Infection and fever raise insulin resistance. A 10–20% increase in basal for the duration of illness is a reasonable starting adjustment, guided by glucose trends.
- Correction doses every 2–3 hours for high glucose plus ketones, with clear fluids and electrolyte replacement (Pedialyte, broth, diluted juice if glucose is low).
- Go to the ER if you cannot keep fluids down, ketones are moderate or large, breath smells fruity, breathing is deep and fast, or you cannot think clearly. DKA is a medical emergency.
Exercise Adjustments
Exercise is one of the most powerful glucose-lowering tools you have, and also one of the most common causes of hypoglycemia. Three patterns matter:
- Planned exercise within 2 hours of a meal bolus. Reduce the pre-meal rapid dose by 25 to 75% depending on intensity and duration. A 45-minute walk after dinner might need 25% less bolus; a 2-hour hike needs 50–75% less.
- Long-duration aerobic exercise (cycling, running, hiking more than an hour) raises insulin sensitivity for up to 24 hours afterward. Reduce basal by 10–20% the evening before and the night after. Pump users program a temporary basal rate at 70–80% for the workout window plus the recovery night.
- Resistance training and high-intensity intervals release adrenaline, which can push glucose up during the workout and crash it afterward. A small correction dose during the workout, followed by reduced basal for recovery, is a common pattern.
Carry fast carbs (glucose tabs, juice box, Smarties) to every workout. CGM users set a low-alert threshold around 90 mg/dL during exercise so they get warning before symptoms.
Hypoglycemia Prevention in Brittle T1D
Some people, especially long-duration T1D patients, develop hypoglycemia unawareness — they no longer feel the shakiness, sweating, or hunger that warn of a low. Numbers can drop into the 40s before they notice. The standard toolkit:
- Rule of 15. For a low (under 70 mg/dL), take 15 grams of fast carbs (4 glucose tabs, 4 oz juice, 1 tablespoon honey). Re-check in 15 minutes. Repeat if still low. Do not over-treat — stacking 60 g of juice into a 55 mg/dL low launches you to 250 an hour later.
- Glucagon. For severe lows when the person cannot swallow. Modern options: Baqsimi (nasal powder, no mixing required), Gvoke (prefilled pen or syringe), Zegalogue (prefilled pen). These have replaced the old red emergency kit. Keep one in the house, one in the car, one at work. Train family members.
- Pump auto-suspend. Control-IQ, 780G, and Omnipod 5 all predict low glucose and reduce or suspend basal automatically.
- CGM alerts. Set urgent-low threshold at 55 mg/dL, predictive low alert at 80–90 mg/dL with a 20–30 minute look-ahead window. Share readings with a partner or parent for overnight peace of mind.
- Hypoglycemia unawareness can reverse. Two to three weeks of strict avoidance of any glucose under 70 often restores awareness. This is hard and usually requires CGM plus basal loosening, but it is worth the effort.
Insurance and Cost Realities
U.S. insulin pricing has been a national scandal for a decade. The picture in 2026:
- Retail prices for brand-name analogs (Humalog, Novolog) historically exceeded $300 per vial or $500 per box of pens. Biosimilars (Admelog, Semglee, Basaglar) cut that roughly in half, to about $160 per vial.
- 2023 list-price reductions. Under pressure from federal legislation and public outcry, Eli Lilly, Novo Nordisk, and Sanofi all announced large list-price cuts. Lilly dropped Humalog and Humulin list prices by 70%. Novo cut Novolog and Levemir by 75%. Sanofi capped Lantus and Admelog at $35/month out-of-pocket for commercially insured patients. These cuts are finally visible at the pharmacy counter in 2025–2026.
- Medicare Part D $35 cap. Since January 2023, all insulins covered under Part D are capped at $35 per month copay. This applies to every Medicare beneficiary automatically — no enrollment needed.
- Manufacturer copay programs. Commercially insured patients can use manufacturer savings cards to cap most insulins at $35 per month. These do not work with Medicare, Medicaid, or TriCare.
- Walmart ReliOn. Novolin R, Novolin N (NPH), and Novolin 70/30 are sold at Walmart for about $25 per vial with no prescription in most states. ReliOn NovoLog (aspart) analog is about $73 per vial. These are the fallback for uninsured patients. They keep people alive, but the older formulations require more discipline.
- Afrezza inhaled insulin runs around $200–$300 per month with insurance coverage and typically more without.
- Biosimilar landscape. Semglee is an interchangeable biosimilar of Lantus — pharmacists can substitute without a new prescription. Basaglar is a non-interchangeable biosimilar that requires the prescription to specifically name it. Rezvoglar is another glargine biosimilar. For aspart, Novolog Mix has several biosimilar candidates in late-stage development.
If you are staring down an unaffordable insulin bill: call the manufacturer's patient assistance program (Lilly Cares, NovoCare, Sanofi Patient Connection) before you cut doses. Most will provide free insulin to uninsured patients below about 400% of the federal poverty line. Never ration insulin silently — the mortality risk is real and help exists.
Key Research Papers
Foundational peer-reviewed work on insulin analog pharmacology, basal-bolus and pump regimens, and the move toward automated insulin delivery. Each citation links to the full text via DOI.
- Hirsch IB. Insulin Analogues. New England Journal of Medicine. 2005;352(2):174–183.
- Russell-Jones D, Bode BW, De Block C, et al. Fast-Acting Insulin Aspart Improves Glycemic Control in Basal-Bolus Treatment for Type 1 Diabetes (onset 1). Diabetes Care. 2017;40(7):943–950.
- Bergenstal RM, Garg S, Weinzimer SA, et al. Safety of a Hybrid Closed-Loop Insulin Delivery System in Patients with Type 1 Diabetes. JAMA. 2016;316(13):1407–1408.
- Brown SA, Kovatchev BP, Raghinaru D, et al. Six-Month Randomized, Multicenter Trial of Closed-Loop Control in Type 1 Diabetes (iDCL). New England Journal of Medicine. 2019;381(18):1707–1717.
- Pickup JC, Sutton AJ. Severe Hypoglycaemia and Glycaemic Control in Type 1 Diabetes: Meta-Analysis of Multiple Daily Insulin Injections Compared with Continuous Subcutaneous Insulin Infusion. Diabetic Medicine. 2008;25(7):765–774.
- Holman RR, Farmer AJ, Davies MJ, et al. Three-Year Efficacy of Complex Insulin Regimens in Type 2 Diabetes (4-T). New England Journal of Medicine. 2009;361(18):1736–1747.
- The Diabetes Control and Complications Trial Research Group. The Effect of Intensive Treatment of Diabetes on the Development and Progression of Long-Term Complications in Insulin-Dependent Diabetes Mellitus (DCCT). New England Journal of Medicine. 1993;329(14):977–986.
- UK Prospective Diabetes Study (UKPDS) Group. Intensive Blood-Glucose Control with Sulphonylureas or Insulin Compared with Conventional Treatment and Risk of Complications in Patients with Type 2 Diabetes (UKPDS 33). Lancet. 1998;352(9131):837–853.
- American Diabetes Association Professional Practice Committee. Standards of Care in Diabetes—2024. Diabetes Care. 2024;47(Suppl 1):S1–S321.
- Bode BW, McGill JB, Lorber DL, et al. Inhaled Technosphere Insulin Compared with Injected Prandial Insulin in Type 1 Diabetes: A Randomized 24-Week Trial. Journal of Diabetes Science and Technology. 2013;9(2):260–270.
Live PubMed Searches
Each link opens a live PubMed query so results stay current as new papers are indexed.
- Insulin analog pharmacokinetics
- Basal-bolus therapy in type 1 diabetes
- Insulin degludec and nocturnal hypoglycemia
- Automated insulin delivery and hybrid closed-loop systems
- Insulin-to-carbohydrate ratio methodology
- Dawn phenomenon in diabetes
- Hypoglycemia unawareness in type 1 diabetes
- Inhaled insulin (Afrezza) clinical outcomes
- Insulin biosimilars and interchangeability
Connections
- Blood Sugar & Insulin — interactive animation
- Diabetes Overview
- Type 1 vs Type 2 vs LADA and MODY
- Cardio-Renal Protection: SGLT2 and GLP-1
- Hypoglycemia Awareness and Prevention
- Remission and Reversal Strategies
- CGM and Time-in-Range
- A1c, Fructosamine, and Glycation Markers
- Complications: Retinopathy, Nephropathy, Neuropathy
- Diabetic Foot Care and Ulcer Prevention
- Insulin Resistance
- Obesity
- Metabolic Syndrome
- Hashimoto's Thyroiditis
- Gestational Diabetes
- Continuous Glucose Monitor
- Peripheral Neuropathy
- GLP-1 Receptor Agonists
- Fasting