Hypoglycemia Awareness and Prevention
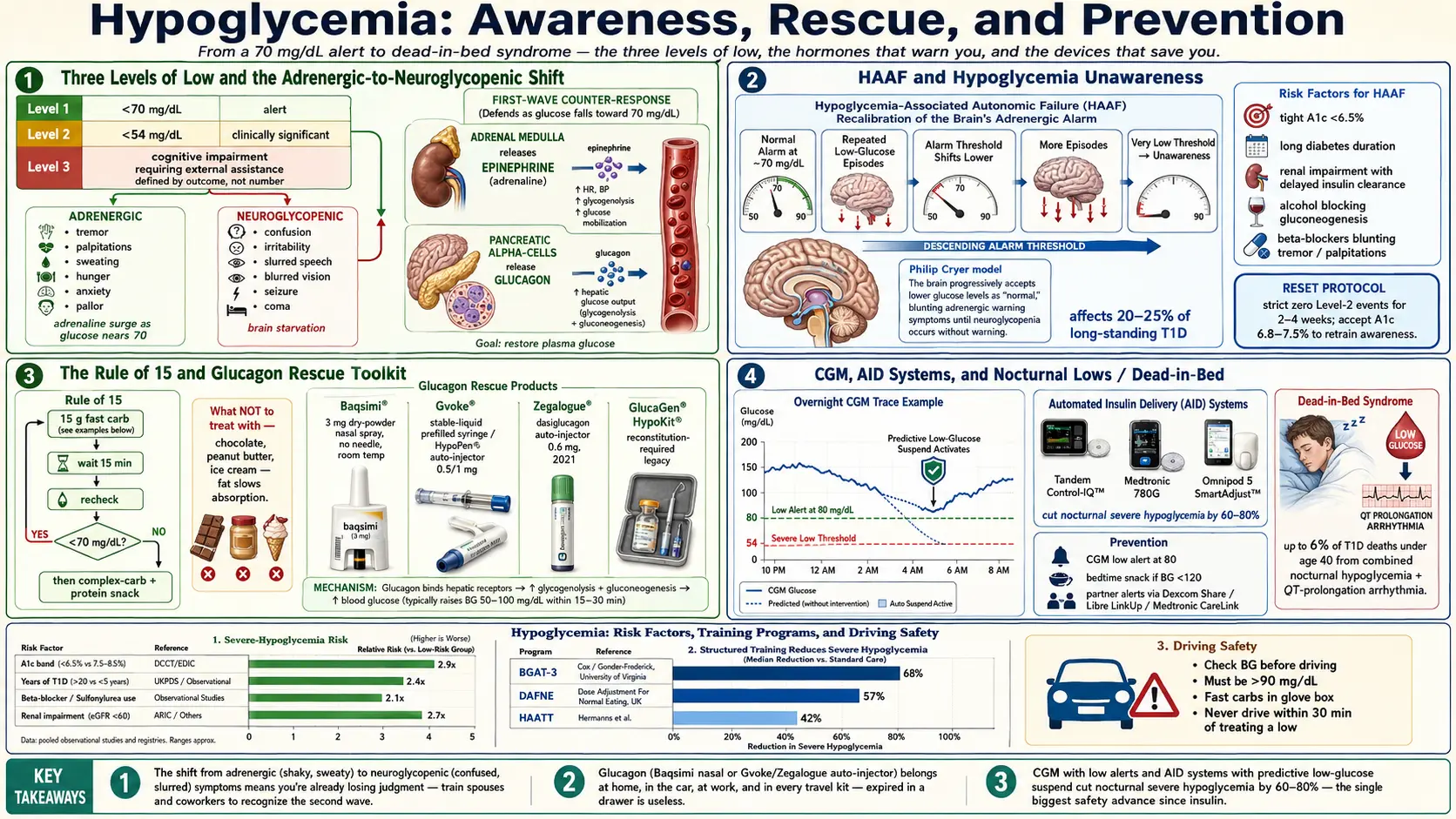
Table of Contents
- Definitions — Three Levels of Low
- Symptoms — Early vs. Late
- Hypoglycemia Unawareness and HAAF
- Risk Factors
- The Rule of 15
- Glucagon Rescue for Severe Hypoglycemia
- CGM and Automated Insulin Delivery
- Restoring Awareness
- Nocturnal Hypoglycemia and Dead-in-Bed
- Alcohol, Exercise, and Sick Days
- Special Populations
- Driving Safety
- Spouse and Partner Impact
- Rare Differentials — Insulinoma and Post-Bariatric
- Key Research Papers
- Connections
- Featured Videos
Definitions — Three Levels of Low
In 2018 the American Diabetes Association and the International Hypoglycaemia Study Group agreed on a single three-tier system that is now used in every clinical trial, every guideline, and every CGM readout. Knowing which level you are in tells you how fast to move and how seriously to treat it.
- Level 1 — Glucose alert value. Blood glucose <70 mg/dL (3.9 mmol/L) but ≥54. This is the "get some sugar now" threshold. You may or may not feel symptoms. It is not yet dangerous but it is the warning light on the dashboard.
- Level 2 — Clinically significant hypoglycemia. Blood glucose <54 mg/dL (3.0 mmol/L). At this level the brain is measurably impaired and the counterregulatory hormone response is fully activated. Research trials count Level 2 events as meaningful adverse outcomes.
- Level 3 — Severe hypoglycemia. Any low glucose event that causes cognitive impairment severe enough to require external assistance — another person feeding you juice, injecting glucagon, or calling 911. Level 3 is defined by the outcome, not a specific number. A reading of 45 mg/dL you treated yourself is Level 2; a reading of 58 that left you confused and needing help is Level 3.
The jump from Level 1 to Level 3 can take minutes in an insulin-using patient, which is why the 70 mg/dL alert matters so much. It is the only level you can still treat with a juice box and no help.
Symptoms — Early vs. Late
Low blood sugar produces two distinct waves of symptoms, and they tell you different things about what is happening in your body.
Adrenergic symptoms (early). As glucose falls toward 70, the adrenal glands dump epinephrine and the pancreas dumps glucagon. You feel the adrenaline:
- Tremor — shaky hands
- Palpitations — fast or pounding heart
- Sweating — cold, clammy, often on the forehead and chest
- Hunger — sudden, urgent
- Anxiety — a wash of dread that feels out of proportion
- Pallor and goosebumps
These are the "treat it now" symptoms. Pay attention to them. They are your early warning system.
Neuroglycopenic symptoms (late). If glucose keeps falling, the brain itself starts to fail because it cannot make its own glucose. The symptoms shift from adrenaline-driven to brain-starvation:
- Confusion, difficulty concentrating
- Irritability, unreasonable behavior, crying or anger that feels out of character
- Slurred speech
- Blurred or double vision
- Incoordination — bumping into walls, dropping things
- Seizure
- Coma
By the time neuroglycopenic symptoms appear, judgment is already impaired. You may not realize you are low. You may refuse juice that a spouse is offering you. This is why training the people around you — and carrying glucagon — matters more than any personal willpower.
Hypoglycemia Unawareness and HAAF
After repeated low glucose events, the body's alarm system gets quieter. This is called hypoglycemia-associated autonomic failure (HAAF), first described in detail by Philip Cryer. Every low teaches the brain to expect lows, and the adrenergic release that used to fire at 70 now fires at 55, or 50, or not at all. The first warning you get is no longer shakiness — it is confusion.
Roughly 20–25% of people with long-standing type 1 diabetes develop some degree of hypoglycemia unawareness. The rate is lower but still meaningful in insulin-treated type 2. It is the single strongest predictor of severe hypoglycemia, car accidents, and hypoglycemia-related hospitalization.
The cruel part of HAAF is that it is caused by the thing you are trying to avoid. Every Level 2 low raises the bar for the next one. A tight A1c target achieved through frequent lows is a setup for eventual unawareness. Restoring awareness (covered below) requires deliberately accepting higher glucose for a few weeks to let the alarm system reset.
Risk Factors
Hypoglycemia does not strike randomly. The risk factors are well mapped, and knowing yours is the first step in prevention:
- Tight A1c targets. An A1c below 6.5% in an insulin user usually means frequent lows. The benefit of an ultra-low A1c has to be balanced against the cost of hypoglycemia — especially in older adults.
- Long diabetes duration. Counterregulatory responses weaken over years. A 40-year type 1 has a very different risk profile than a five-year type 1.
- Renal impairment. The kidneys clear insulin. As eGFR drops, insulin lingers, and doses that used to work now overshoot.
- Alcohol. Ethanol blocks the liver from producing glucose (gluconeogenesis) for 8–12 hours. This is why overnight lows after evening drinks are so dangerous.
- Missed or delayed meals. Bolus insulin already injected + no carbs arriving = a predictable crash.
- Exercise without adjustment. Muscles pull glucose without needing insulin during and after exercise. Lows can appear up to 24 hours later.
- Insulin dosing errors. Mixing up basal and bolus pens is one of the most common causes of ER-level severe hypoglycemia.
- Sulfonylureas in the elderly. Glyburide and glipizide cause prolonged lows that can last 24–72 hours in older patients with renal decline. The ADA specifically recommends avoiding them in adults over 65.
- Beta-blockers. These blunt the tremor and palpitations of adrenergic warning, leaving only sweating. If you are on a beta-blocker and diabetic, you need a CGM.
- Sleep deprivation and irregular schedules. Poor sleep impairs counterregulation and raises variability.
The Rule of 15
The standard protocol for treating a Level 1 low is simple enough to remember at 3 a.m. with a blood glucose of 58:
- 15 grams of fast-acting carbohydrate. Pure glucose is best because it raises blood sugar within 10–15 minutes without fat or fiber to slow it down.
- Wait 15 minutes.
- Recheck. If still <70, repeat. If >70 and the next meal is more than an hour away, follow with a complex carb + protein snack (crackers with peanut butter, half a turkey sandwich, a glass of milk) to keep you stable.
What counts as 15 grams of fast-acting carb:
- 4 ounces (120 mL) of juice or regular soda
- 3 glucose tabs (most tabs are 4–5 g each)
- 1 tablespoon of honey or table sugar
- 1 tube of glucose gel
- 8–10 Lifesavers or jelly beans (check the label)
What does not count and will betray you at 3 a.m.:
- Chocolate. The fat slows glucose absorption by 30–60 minutes. You will over-treat waiting for a response.
- Nut butter, ice cream, cookies. Same reason — fat is the enemy of fast correction.
- Bread or crackers alone. Too slow as a rescue, though fine as the follow-up snack.
Avoid over-treatment. The most common hypoglycemia mistake is panic-eating the entire pantry. A properly dosed 15 g will raise blood glucose by about 40–50 mg/dL. Inhaling 60 g of carbs at 3 a.m. leaves you at 250 by breakfast and triggers a correction bolus that causes the next low. Count the carbs. Wait the 15 minutes. Recheck.
Glucagon Rescue for Severe Hypoglycemia
When a person with diabetes cannot swallow, is seizing, or is unconscious, you cannot give oral sugar — it will go into the lungs. You need glucagon, the counter-hormone to insulin, which tells the liver to dump stored glucose into the bloodstream. Every insulin-using household should have glucagon, and every close contact should know how to use it.
The choice of glucagon matters because the old kit is intimidating in an actual emergency. Four products are available in 2026:
- Baqsimi (nasal glucagon). A single-use nasal device containing 3 mg of dry-powder glucagon. No needle, no reconstitution. Stored at room temperature up to 30 months. You pull off the cap, insert the tip into one nostril, and press the plunger. Works even if the person is not breathing through their nose. Approved 2019 (Lane et al.) This is the easiest rescue for a panicked spouse, teacher, or coworker.
- Gvoke (prefilled syringe or HypoPen auto-injector). Stable liquid glucagon in 0.5 mg (pediatric) or 1 mg (adult) doses. The HypoPen works like an EpiPen — uncap, press against the thigh, hold for 5 seconds. The prefilled syringe is cheaper but requires exposing a needle. Approved 2019 (Rickels et al.)
- Zegalogue (dasiglucagon auto-injector). A stable-liquid glucagon analog, 0.6 mg auto-injector. Rapid onset, comparable to Gvoke. Approved 2021.
- GlucaGen Hypokit. The old reconstitution kit — a vial of powder, a syringe of diluent, mix and inject. Still on the market and sometimes cheaper, but studies consistently show bystanders fumble it under stress. If you have a choice, pick a ready-to-use option.
Training the people around you. Glucagon is useless in a drawer if your spouse, roommate, adult children, or coworkers don't know it exists. Show them the device. Have them practice with an expired trainer. Put a sticky note on the fridge: "Baqsimi in the nightstand — nasal tip in either nostril — then call 911."
Multiple locations. One kit at home is not enough. Keep glucagon in your car, at work, in the gym bag, and in every travel kit. Severe lows do not check your location first.
Expiration management. Ready-to-use glucagon expires in 24–30 months. Put a calendar reminder the day you fill it. Pharmacies will not automatically remind you. An expired glucagon at the moment you need it is a disaster.
Cost and coverage. Retail cash prices in 2024–2026 run $300–$400 per device. GoodRx and manufacturer coupons typically bring that to $100–$250. Commercial insurance and Medicare Part D generally cover glucagon with prior authorization — if denied, ask your endocrinologist to submit a medical-necessity letter citing your insulin regimen and any prior severe hypoglycemia. Most plans approve on appeal.
CGM and Automated Insulin Delivery
The single biggest change in hypoglycemia safety in the past decade is not a new drug — it is the continuous glucose monitor paired with an insulin pump that can turn itself off.
Predictive low-glucose suspend is a feature in all three major automated insulin delivery (AID) systems:
- Tandem Control-IQ — with a Dexcom G6 or G7, the t:slim X2 pump predicts glucose 30 minutes ahead and reduces or stops basal insulin when a low is projected.
- Medtronic 780G — with the Guardian 4 or Simplera sensor, the pump suspends basal when glucose trends low and auto-corrects when trending high.
- Omnipod 5 SmartAdjust — the tubeless pod pairs with Dexcom and adjusts every five minutes.
Randomized trials show these systems cut nocturnal severe hypoglycemia by 60–80% compared with traditional pump therapy. For a type 1 patient with a history of overnight lows, AID is arguably more life-saving than any single drug. See the CGM and AID article for the full comparison.
Restoring Awareness
Hypoglycemia unawareness is not permanent. The counterregulatory response can be retrained, but it requires a deliberate, uncomfortable choice: strictly avoid lows for 2–4 weeks. That usually means accepting a higher A1c (6.8–7.5% instead of 6.2%) and running glucose targets of 80–180 instead of 70–140 during the reset. Studies out of Yale and the Joslin show adrenergic symptoms return in most patients within two to three weeks of zero Level 2 events.
Patient-facing structured programs take this further:
- Blood Glucose Awareness Training (BGAT-3) — developed by Daniel Cox and Linda Gonder-Frederick at the University of Virginia. A seven-session course teaching patients to detect early adrenergic cues, predict glucose from context (meals, insulin, exercise), and prevent the cascade to Level 3. Randomized trials show meaningful reductions in severe hypoglycemia.
- DAFNE (Dose Adjustment For Normal Eating) — a five-day structured program widespread in the UK and increasingly available internationally. Teaches carb counting, insulin-to-carb ratios, correction factors, and hypoglycemia management. Attending DAFNE reduces severe hypo rates and improves quality of life.
- Hypoglycemia Anticipation, Awareness and Treatment Training (HAATT) — another structured option, often available through endocrinology practices.
Ask your endocrinologist for a referral. If none are available locally, the online BGAT materials and DAFNE Online are reasonable starting points.
Nocturnal Hypoglycemia and Dead-in-Bed
Nighttime is the most dangerous window. You are asleep, you cannot feel adrenergic symptoms, and if a low is severe enough to cause seizure or arrhythmia, no one may find you in time. Dead-in-bed syndrome — a rare but real event in young type 1 patients who go to sleep apparently well and are found dead with no structural cause at autopsy — is thought to involve a combination of severe nocturnal hypoglycemia and a QT-prolongation-driven arrhythmia. Estimates attribute up to 6% of deaths in type 1 patients under age 40 to this pattern.
Preventing nocturnal lows:
- Use a CGM with low alerts. This is non-negotiable for anyone on insulin who has had a nighttime low. Set the alert at 80 mg/dL so you have runway.
- Bedtime snack if BG <120. A small complex-carb + protein snack (Greek yogurt, cheese and crackers, half a peanut-butter sandwich) blunts the overnight drift.
- Avoid heavy insulin doses within 2–3 hours of bed. Late corrections stack with basal and cause the classic 2 a.m. low.
- AID systems with low-glucose suspend. The single most effective prevention.
- Partner alerts. Dexcom Share, Libre LinkUp, and Medtronic CareLink can push CGM alerts to a spouse's or parent's phone — sometimes literally waking the person who needs to wake you.
Alcohol, Exercise, and Sick Days
Alcohol. Ethanol suppresses hepatic gluconeogenesis for 8–12 hours. The result is a predictable late-night or early-morning low, often at 3–5 a.m., after evening drinking. Rules:
- Drink with food, never on an empty stomach.
- Check blood glucose before bed. If <120, eat a snack.
- Do not "correct" slightly high pre-bed glucose with extra insulin after drinking — the alcohol will amplify the overnight drop.
- Tell whoever you are with that you have diabetes. Alcohol intoxication and severe hypoglycemia look identical to bystanders, and delayed glucagon is a common cause of hospitalization.
Exercise. Muscles pull glucose during and after activity, and the effect lasts up to 24 hours post-workout. "Delayed hypoglycemia" the night after a long run is extremely common. Mitigations: reduce basal by 10–25% for 12–18 hours after strenuous exercise, eat a mixed snack before bed, and set the CGM low alert higher than usual.
Sick days. Illness is a paradox. Infection raises insulin needs, but nausea and poor intake cut carb load. Patients often bolus for food they plan to eat, then can't keep it down, and crash. Reduce bolus for actually-consumed carbs only, keep sipping fluids with sugar if glucose is trending low, and check ketones in parallel — concurrent hypoglycemia and DKA can coexist and confuse the picture.
Special Populations
Pregnancy with type 1 diabetes. Guidelines push glucose targets tighter (fasting <95, post-meal <140) precisely when insulin sensitivity shifts week to week. Hypoglycemia rates in the first trimester are often 3–5x baseline. AID systems with pregnancy-specific algorithms (CamAPS FX in the UK, off-label Control-IQ adjustments in the US) are game-changers. Glucagon use in pregnancy is safe and should not be withheld.
Elderly with cognitive impairment. The ADA explicitly recommends relaxing A1c targets to 7.5–8.5% in older adults with dementia or significant comorbidities. Tight control in this population causes more harm than it prevents. Replace sulfonylureas with DPP-4 inhibitors or low-dose metformin where possible. See GLP-1 and SGLT2 medications for safer alternatives.
Children and teens. Schools in the US are required under Section 504 to accommodate diabetes management. A Diabetes Medical Management Plan (DMMP) and a 504 plan should specify who checks glucose, who administers insulin, where glucagon is stored, and which staff are trained to use it. Nasal glucagon (Baqsimi) has transformed school emergency response because any adult can give it without needle training.
Driving Safety
The ADA's longstanding guidance is the "Check Before You Drive" rule. If your glucose is under 100 mg/dL before driving, treat it first — do not start the car. A low at 55 mph has killed patients and bystanders.
Practical rules:
- Check glucose within 30 minutes of driving.
- Keep fast-acting carbs (glucose tabs, juice box) within arm's reach — not in the trunk.
- On long drives, recheck every two hours.
- If you feel low, pull over immediately, treat, wait 15 minutes, recheck before driving again.
Reporting requirements. In the UK, the DVLA requires drivers with insulin-treated diabetes to report their condition and to meet a minimum of one episode of severe hypoglycemia per 12 months (Group 1 license). In the US, state DMV rules vary. California, for example, does not require routine reporting but physicians may report drivers with repeated hypoglycemic episodes causing loss of consciousness. Know your state's rule before a first ER visit for severe hypo creates a paperwork surprise.
Spouse and Partner Impact
The person sleeping next to you carries an invisible load. Partner surveys consistently show elevated rates of sleep disruption, anxiety, hypervigilance, and depression in spouses of type 1 patients with severe hypoglycemia history. They wake to check you breathing. They learn to interpret CGM alarms in their sleep. They give glucagon at 4 a.m. and then go to work.
Ways to share the load:
- Use CGM share features so the partner gets the alerts, not just you.
- Practice the glucagon device together, yearly.
- Acknowledge it directly — partners rarely bring it up.
- Consider couples support groups through JDRF or Beyond Type 1.
- For AID users, the reduction in nocturnal lows is as much a gift to the partner as to the patient.
Rare Differentials — Insulinoma and Post-Bariatric
Not every hypoglycemia is diabetes-related. Two important differentials:
Insulinoma. A rare insulin-secreting pancreatic tumor. Presents with fasting hypoglycemia in a non-diabetic patient, often with neuroglycopenic symptoms that improve dramatically after eating. Diagnosed with a supervised 72-hour fast showing inappropriately high insulin and C-peptide at the time of documented low glucose. Curable by surgical resection in most cases.
Reactive (postprandial) hypoglycemia after bariatric surgery. After Roux-en-Y gastric bypass, a subset of patients develop "late dumping" — rapid glucose absorption, exaggerated insulin release, and a crash 1–3 hours after meals. Managed with low-glycemic-index diet, acarbose, sometimes diazoxide. Worth flagging if a post-bariatric patient describes shakiness an hour or two after eating.
Insulin pump failure + DKA masking hypoglycemia. A stuck insulin pump that over-delivers can cause both hypoglycemia (from excess insulin) and, if mechanical failure then cuts delivery, rapid swing into DKA. Unusual, but worth knowing.
The classic severe-hypo combination. Emergency-department data identify one scenario repeatedly: alcohol + sulfonylurea + nighttime in an elderly type 2 patient. The alcohol suppresses hepatic glucose output, the sulfonylurea stimulates insulin release for 24–72 hours, and nighttime removes the meal-based carbohydrate floor. If you are over 65 and still on glyburide or glipizide, ask your physician about switching.
Key Research Papers
Foundational peer-reviewed work on hypoglycemia classification, hypoglycemia-associated autonomic failure (HAAF), and the rescue therapies that protect against severe events. Each citation links to the full text via DOI.
- International Hypoglycaemia Study Group. Glucose Concentrations of Less Than 3.0 mmol/L (54 mg/dL) Should Be Reported in Clinical Trials: A Joint Position Statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care. 2017;40(1):155–157.
- Cryer PE. Mechanisms of Hypoglycemia-Associated Autonomic Failure in Diabetes. New England Journal of Medicine. 2013;369(4):362–372.
- Seaquist ER, Anderson J, Childs B, et al. Hypoglycemia and Diabetes: A Report of a Workgroup of the American Diabetes Association and The Endocrine Society. Diabetes Care. 2013;36(5):1384–1395.
- Rickels MR, Ruedy KJ, Foster NC, et al. Intranasal Glucagon for Treatment of Insulin-Induced Hypoglycemia in Adults with Type 1 Diabetes. Diabetes Care. 2016;39(2):264–270.
- The DCCT Research Group. Epidemiology of Severe Hypoglycemia in the Diabetes Control and Complications Trial. American Journal of Medicine. 1991;90(4):450–459.
- Choudhary P, Rickels MR, Senior PA, et al. Evidence-Informed Clinical Practice Recommendations for Treatment of Type 1 Diabetes Complicated by Problematic Hypoglycemia. Diabetes Care. 2015;38(6):1016–1029.
- The Diabetes Control and Complications Trial Research Group. The Effect of Intensive Treatment of Diabetes on the Development and Progression of Long-Term Complications in Insulin-Dependent Diabetes Mellitus (DCCT). New England Journal of Medicine. 1993;329(14):977–986.
- UK Prospective Diabetes Study (UKPDS) Group. Intensive Blood-Glucose Control with Sulphonylureas or Insulin Compared with Conventional Treatment and Risk of Complications in Patients with Type 2 Diabetes (UKPDS 33). Lancet. 1998;352(9131):837–853.
- American Diabetes Association Professional Practice Committee. Standards of Care in Diabetes—2024. Diabetes Care. 2024;47(Suppl 1):S1–S321.
- Brown SA, Kovatchev BP, Raghinaru D, et al. Six-Month Randomized, Multicenter Trial of Closed-Loop Control in Type 1 Diabetes (iDCL). New England Journal of Medicine. 2019;381(18):1707–1717.
Live PubMed Searches
Each link opens a live PubMed query so results stay current as new papers are indexed.
- Hypoglycemia unawareness and HAAF
- Nasal glucagon (Baqsimi) for severe hypoglycemia
- Dasiglucagon (Zegalogue) clinical trials
- Automated insulin delivery and nocturnal hypoglycemia
- Blood Glucose Awareness Training (BGAT)
- Dead-in-bed syndrome in type 1 diabetes
- Sulfonylurea-induced hypoglycemia in the elderly
- Post-bariatric reactive hypoglycemia
- Insulinoma diagnosis and fasting test
- Hypoglycemia and driving safety
Connections
- Blood Sugar & Insulin — interactive animation
- Diabetes Overview
- Cardio-Renal Protection: SGLT2 and GLP-1
- CGM and Time-in-Range
- Insulin Types and Dosing Strategies
- Remission and Reversal Strategies
- A1c, Fructosamine, and Glycation Markers
- Complications: Retinopathy, Nephropathy, Neuropathy
- Type 1 vs Type 2 vs LADA and MODY
- Diabetic Foot Care and Ulcer Prevention
- Insulin Resistance
- Hashimoto's Thyroiditis
- Continuous Glucose Monitor
- Blood Sugar
- Anxiety
- Kidney Disease
- Fasting