HFpEF — Heart Failure with Preserved Ejection Fraction
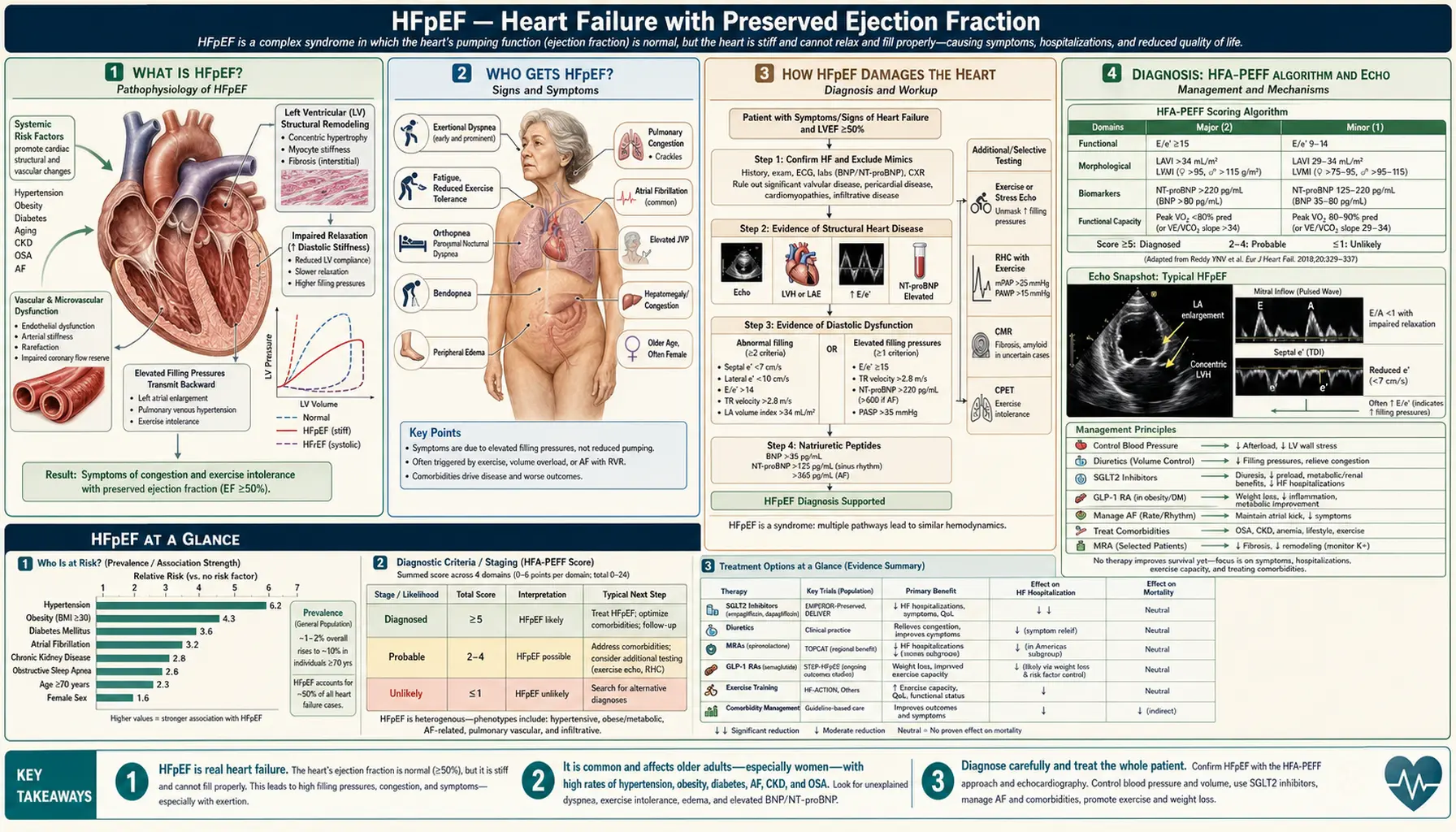
Table of Contents
- What Is HFpEF?
- Who Gets HFpEF?
- How HFpEF Damages the Heart
- Diagnosis: HFA-PEFF Algorithm and Echo
- Diastolic Dysfunction Grading
- Symptoms: Exercise Intolerance and Dyspnea
- Treatment: Landmark Trials and Approved Therapies
- Lifestyle: Weight Loss, Exercise, and Salt Restriction
- Prognosis and Hospitalizations
- Research Papers
- Connections
- Featured Videos
What Is HFpEF?
Heart failure with preserved ejection fraction (HFpEF) is a form of heart failure in which the left ventricle pumps normally — the ejection fraction (EF) is 50% or higher — but the heart muscle is abnormally stiff and cannot relax properly between beats. Because the ventricle fills poorly, less blood enters before each contraction, so total cardiac output falls short of what the body needs, especially during physical activity.
HFpEF now accounts for roughly 50% of all heart failure cases in the United States and its share is rising as the population ages. Unlike heart failure with reduced ejection fraction (HFrEF), where the pump is visibly weak, HFpEF can be deceptively "normal-looking" on a standard echocardiogram, making it historically under-diagnosed and under-treated.
Who Gets HFpEF?
HFpEF has a distinctive patient profile that differs sharply from HFrEF:
- Older women — women develop HFpEF more often than men, and incidence rises steeply after age 65.
- Hypertension — present in more than 80% of HFpEF patients; chronic pressure overload drives left ventricular hypertrophy and stiffening.
- Obesity — adipose tissue secretes pro-inflammatory cytokines (IL-6, TNF-α) that directly stiffen myocardial tissue; abdominal obesity also compresses the pericardium.
- Type 2 diabetes — advanced glycation end-products cross-link collagen in the myocardium, reducing compliance independent of blood pressure.
- Atrial fibrillation (AFib) — both a cause and consequence of HFpEF; loss of atrial "kick" worsens filling; the two conditions share the same risk-factor cluster.
- Chronic kidney disease — fluid overload and uremic inflammation accelerate myocardial fibrosis.
- Sleep apnea — intermittent hypoxia and nocturnal hypertension further impair diastolic function.
Cardiologists often refer to HFpEF as a "syndrome" rather than a single disease because so many comorbidities converge to produce it.
How HFpEF Damages the Heart
In HFpEF the primary problem is diastolic dysfunction — impaired relaxation and reduced compliance of the left ventricle. Several interconnected mechanisms drive this:
- Myocardial fibrosis — fibroblasts deposit excess collagen in response to hypertension, inflammation, and diabetes. Collagen is stiffer than normal myocardium, raising filling pressures.
- Cardiomyocyte hypertrophy — individual heart muscle cells grow larger but less efficient; the sarcomeric protein titin becomes less compliant (hypophosphorylation of the N2B isoform), directly increasing passive stiffness.
- Coronary microvascular dysfunction — small coronary vessels fail to dilate adequately during exertion, causing subendocardial ischemia that further impairs relaxation.
- Elevated left atrial pressure — the left atrium must work against the stiff ventricle; over time it dilates, predisposing to atrial fibrillation and pulmonary congestion.
- Pulmonary hypertension — chronically elevated left-sided filling pressures transmit backward into the pulmonary vasculature, eventually producing pulmonary arterial hypertension and right heart failure.
- Pericardial restraint — in obesity, visceral fat compresses the pericardium, raising pericardial pressure and reducing effective diastolic compliance.
Diagnosis: HFA-PEFF Algorithm and Echo
Diagnosing HFpEF requires proving that (1) symptoms of heart failure are present, (2) EF ≥50%, and (3) elevated filling pressures are the cause. The HFA-PEFF diagnostic algorithm, published by the Heart Failure Association of the European Society of Cardiology, provides a structured five-step framework:
- Pre-test probability — calculate the H2FPEF or HFA-PEFF score from clinical variables (BMI, hypertension, AFib, age, filling pressure markers).
- Echocardiography at rest — measure E/e' ratio, LA volume index (LAVI), tricuspid regurgitation velocity (TRV), and left ventricular mass index.
- Biomarkers — NT-proBNP or BNP. Note that obesity lowers natriuretic peptides, so the threshold is adjusted downward for BMI >35.
- Exercise testing — a negative resting echo does not rule out HFpEF. Exercise echocardiography or right-heart catheterization during exertion can unmask elevated pulmonary capillary wedge pressure (PCWP >15 mmHg at rest or >25 mmHg with exercise).
- Invasive hemodynamics — right-heart catheterization remains the gold standard when non-invasive tests are inconclusive.
Key echocardiographic findings in HFpEF include: E/e' >14, LAVI >34 mL/m², TRV >2.8 m/s, and LV mass index above sex-specific thresholds.
Diastolic Dysfunction Grading
The American Society of Echocardiography (ASE) 2016 guidelines grade diastolic dysfunction in four stages:
- Grade I (impaired relaxation) — E/A ratio <0.8 with normal filling pressures. The ventricle relaxes slowly but can still fill adequately at rest. Very common in older adults; often asymptomatic.
- Grade II (pseudonormal) — E/A ratio 0.8–2.0 with elevated filling pressures (E/e' 10–14, LAVI elevated). The pattern superficially resembles normal but invasive measurements reveal elevated PCWP. Patients may be symptomatic with exertion.
- Grade III (restrictive filling) — E/A ratio >2.0, short deceleration time (<160 ms), severely elevated filling pressures. Symptoms at minimal exertion or at rest.
- Grade IV (irreversible restrictive) — Grade III pattern that does not normalize (become "pseudonormal") with Valsalva maneuver. Associated with advanced myocardial fibrosis.
Grades I–II represent a spectrum from normal aging to early HFpEF; Grades III–IV carry substantially worse prognosis and indicate advanced structural disease.
Symptoms: Exercise Intolerance and Dyspnea
The hallmark symptom of HFpEF is exertional dyspnea — breathlessness with activities that the patient previously tolerated easily. Unlike HFrEF, patients with HFpEF often feel reasonably well at rest, which can lead both patients and doctors to underestimate the severity of the condition.
Common symptoms include:
- Exercise intolerance — reduced peak VO₂ on cardiopulmonary exercise testing (CPET) is the most objective marker; impaired chronotropic response (the heart cannot increase rate adequately with exercise) contributes independently.
- Orthopnea and paroxysmal nocturnal dyspnea — lying flat redistributes fluid from the legs to the lungs, raising pulmonary venous pressure at night.
- Leg swelling (peripheral edema) — fluid retention from elevated venous pressures; worsens through the day.
- Fatigue — low cardiac reserve means organs and muscles receive inadequate oxygen during activity.
- Rapid weight gain — a weight gain of 2 kg (4–5 lb) over 2–3 days signals acute fluid retention and impending decompensation.
- Palpitations — often due to associated atrial fibrillation or frequent atrial ectopy.
Because symptoms can mimic deconditioning, obesity hypoventilation, or lung disease, formal CPET with simultaneous echocardiography is increasingly used to confirm HFpEF as the cause of exertional symptoms.
Treatment: Landmark Trials and Approved Therapies
HFpEF was historically a "therapy desert" — every drug proven in HFrEF failed to show benefit in HFpEF trials. That changed with the SGLT2 inhibitor trials.
TOPCAT Trial — Spironolactone (Equivocal)
The TOPCAT trial (N=3,445, 2014) randomized HFpEF patients to spironolactone 15–45 mg/day vs placebo. The primary composite endpoint (cardiovascular death, aborted cardiac arrest, heart failure hospitalization) was not significantly reduced (HR 0.89, p=0.14), though hospitalization for heart failure was lower in the spironolactone arm. Post-hoc analyses revealed major geographic heterogeneity — patients enrolled in Russia/Georgia had unexpectedly low event rates suggesting enrollment of non-HFpEF patients. The Americas subgroup showed a significant benefit. Spironolactone remains commonly used to reduce hospitalizations despite the neutral overall result.
EMPEROR-Preserved — Empagliflozin (First Approved Therapy)
The EMPEROR-Preserved trial (N=5,988, NEJM 2021) was the pivotal trial that changed HFpEF treatment. Empagliflozin 10 mg/day reduced the composite of cardiovascular death or hospitalization for heart failure by 21% (HR 0.79, p<0.001) in patients with EF ≥40%. The benefit was consistent across the full EF spectrum and was driven primarily by fewer heart failure hospitalizations. Empagliflozin became the first drug FDA-approved specifically for HFpEF in 2023, when the indication was broadened to heart failure regardless of EF.
DELIVER Trial — Dapagliflozin
The DELIVER trial (N=6,263, NEJM 2022) tested dapagliflozin 10 mg/day in HFpEF (EF ≥40%). It reduced the primary composite (worsening heart failure or cardiovascular death) by 18% (HR 0.82, p<0.001). A pooled meta-analysis of EMPEROR-Preserved and DELIVER confirmed SGLT2 inhibitors reduce heart failure hospitalizations, cardiovascular death, and total symptom burden in HFpEF with high consistency.
STEP-HFpEF Trial — Semaglutide
The STEP-HFpEF trial (N=529, NEJM 2023) tested semaglutide 2.4 mg/week (the weight-loss dose) in obese HFpEF patients (BMI ≥30). At 52 weeks, semaglutide produced a 13.3-point improvement in Kansas City Cardiomyopathy Questionnaire (KCCQ) score vs 6.5 points for placebo (p<0.001), accompanied by 13.3% weight reduction and improved 6-minute walk distance. This was the first trial to show that treating obesity directly improves HFpEF symptoms, establishing weight loss as a therapeutic target — not merely a risk factor.
Other Therapies
- Diuretics (loop diuretics — furosemide, torsemide) — relieve congestion and reduce symptoms, but have not been shown to improve survival in HFpEF. The rule "start low, go slow" applies because over-diuresis causes hypotension and renal impairment in a heart that depends on adequate preload to fill.
- Blood pressure control — ACE inhibitors, ARBs, or beta-blockers to keep BP <130/80 mmHg reduce the hypertensive driver of myocardial stiffening.
- Rate control for AFib — maintaining a resting heart rate of 60–80 bpm allows more time for diastolic filling.
- Sacubitril/valsartan (neprilysin inhibitor) — the PARAGON-HF trial showed a trend toward benefit in women and those with EF 45–57%, leading some guidelines to suggest consideration in these subgroups.
Lifestyle: Weight Loss, Exercise, and Salt Restriction
Lifestyle modification is a cornerstone of HFpEF management because so many causal comorbidities respond to behavioral change:
- Weight loss — even modest 5–10% weight reduction reduces pericardial fat, lowers cardiac filling pressures, decreases systemic inflammation, and improves exercise capacity. The STEP-HFpEF data confirmed that pharmacologic weight loss with semaglutide produces clinically meaningful symptom benefit.
- Aerobic exercise training — the Ex-DHF and HF-ACTION subgroup data show that structured exercise improves peak VO₂, KCCQ score, and 6-minute walk distance without harm. Moderate-intensity exercise 150 minutes/week is recommended; cardiac rehabilitation referral is appropriate.
- Sodium restriction — limiting dietary sodium to 2,000–2,300 mg/day reduces fluid retention and daily weight fluctuations.
- Fluid restriction — in patients with recurrent fluid overload, limiting total fluid intake to 1.5–2 L/day reduces decompensation episodes.
- Sleep apnea treatment — CPAP therapy reduces nocturnal hypertensive episodes and sympathetic surges that worsen diastolic function.
- Daily weight monitoring — patients who weigh themselves every morning and call their care team for a 2 kg rise have significantly fewer emergency hospitalizations.
Prognosis and Hospitalizations
HFpEF carries a 5-year mortality of approximately 50%, comparable to HFrEF and many common cancers, yet it remains under-recognized as a serious illness. Most deaths are from cardiovascular causes (sudden death, progressive heart failure, stroke), but non-cardiovascular deaths from comorbidities (cancer, renal failure, infection) are proportionally higher in HFpEF than in HFrEF.
Heart failure hospitalizations are both common and costly — patients with HFpEF have a 30-day readmission rate of 20–25%. Each hospitalization accelerates disease progression. Poor prognostic markers include: LAVI >40 mL/m², pulmonary arterial hypertension, right ventricular dysfunction, persistent NT-proBNP elevation above 1000 pg/mL, and low peak VO₂ (<14 mL/kg/min) on exercise testing.
Frailty, sarcopenia, and poor nutritional status independently worsen outcomes in the predominantly elderly HFpEF population, underscoring the need for multidisciplinary care that addresses skeletal muscle health alongside cardiac function.
Research Papers
The following citations are from published peer-reviewed literature on HFpEF diagnosis and treatment. PubMed links open the specific article or a targeted search.
- Search PubMed (EMPEROR-Preserved: empagliflozin in HFpEF)
- Search PubMed (DELIVER: dapagliflozin in HFpEF)
- Search PubMed (STEP-HFpEF: semaglutide in obese HFpEF)
- Pitt B et al., 2014 — PMID: 24716680 (TOPCAT: spironolactone in HFpEF)
- Search PubMed (HFA-PEFF diagnostic algorithm)
- Search PubMed (ASE diastolic dysfunction grading guidelines)
- Search PubMed (HFpEF phenotyping and comorbidity clusters)
- Search PubMed (H2FPEF score for HFpEF diagnosis)
- Search PubMed (Pathophysiology of HFpEF — diastolic dysfunction mechanisms)
- Search PubMed (SGLT2 inhibitor pooled meta-analysis HFpEF)
- Search PubMed (Exercise training in HFpEF — Ex-DHF trial)
- Search PubMed (ESC 2021 Heart Failure Guidelines)
Connections
- Cardiology
- Heart Failure
- Hypertension
- Atrial Fibrillation
- Cardiomyopathy
- Coronary Artery Disease
- Cardiovascular Disease
- Valvular Heart Disease
- Diabetes
- Pulmonary Embolism
- Shortness of Breath
- Edema
- Fatigue
- Magnesium
- Potassium
- Omega-3 Fatty Acids
- Chronic Kidney Disease