Melatonin: The Master Mitochondrial Antioxidant
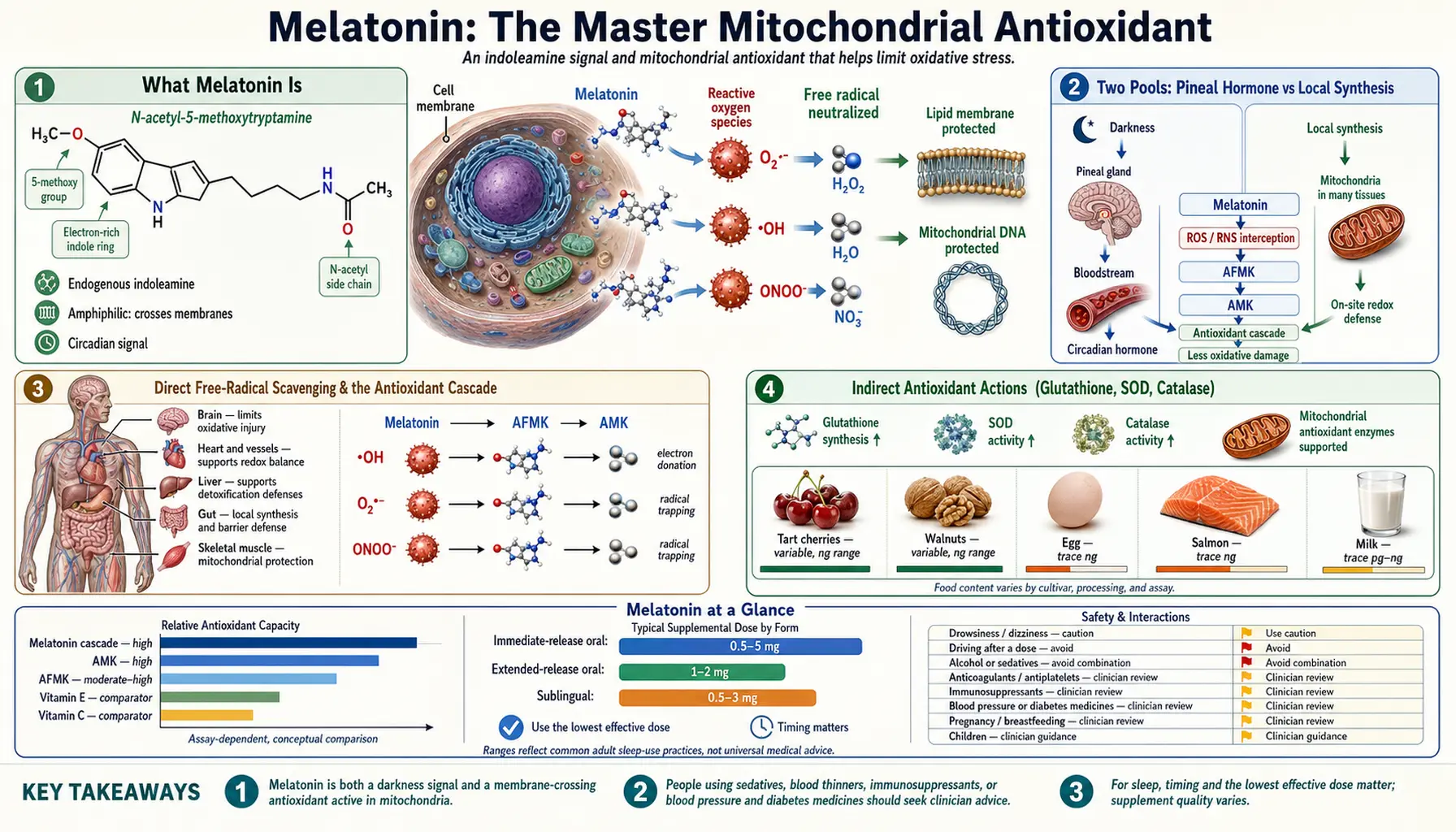
Melatonin (N-acetyl-5-methoxytryptamine) is best known as the hormone that signals darkness and times sleep, but its older and arguably more important job is chemical defense. It is a small, amphiphilic molecule that crosses every membrane and barrier in the body, concentrates inside mitochondria — the very place where most free radicals are born — and neutralizes them through a remarkable antioxidant cascade in which each of its breakdown products is itself a radical scavenger. Melatonin also recharges the cell's other defenses by raising glutathione and the activity of superoxide dismutase, catalase, and glutathione peroxidase. Endogenous production falls sharply with age, which is one reason melatonin has been studied not only for sleep and circadian rhythm but for mitochondrial protection, neuroprotection, cardiovascular and immune support, and as an adjunct in oncology research.
Interactive Visualization Sleep Stages & Your Body Clock — run a whole night Watch deep sleep and REM cycle through the night — then add late-night light, an afternoon coffee, or a nightcap and see what breaks. Launch → Interactive Visualization Caffeine, Adenosine & Why Coffee Stops Working Caffeine doesn’t give you energy — it blocks the tiredness signal while adenosine keeps piling up behind the blockade. Move your coffee to 2 p.m. and watch your deep sleep vanish. Launch →
Table of Contents
- What Melatonin Is
- Two Pools: Pineal Hormone vs Local Synthesis
- Direct Free-Radical Scavenging & the Antioxidant Cascade
- Indirect Antioxidant Actions (Glutathione, SOD, Catalase)
- Why Melatonin Concentrates in Mitochondria
- Sleep & Circadian Rhythm
- Mitochondrial & Neuroprotection
- Cardiovascular Effects
- Immune Modulation
- Adjunct Oncology Research
- Dietary Factors & Age-Related Decline
- Forms, Low-Dose vs High-Dose & Timing
- Safety, Side Effects & Interactions
- Key Research Papers
- Connections
- Featured Videos
What Melatonin Is
Melatonin is an indoleamine — a small molecule built from the amino acid tryptophan. The biosynthetic route is direct and worth knowing because it explains both melatonin's daily rhythm and its overlap with mood chemistry: tryptophan is hydroxylated to 5-hydroxytryptophan (5-HTP), decarboxylated to serotonin, then N-acetylated by the rate-limiting enzyme arylalkylamine N-acetyltransferase (AANAT), and finally O-methylated by ASMT (HIOMT) to yield melatonin. AANAT activity rises at night and falls in light, which is why melatonin is a faithful chemical readout of darkness.
Structurally, melatonin is unusual among biological antioxidants because it is amphiphilic — soluble enough in both water and lipid to move freely through cytoplasm, lipid membranes, the blood-brain barrier, and the placenta. It needs no membrane transporter and reaches essentially every subcellular compartment. That ubiquity, combined with its electron-rich indole ring, is the physical basis for its broad antioxidant reach.
Melatonin is also evolutionarily ancient. It is found in bacteria, single-celled eukaryotes, fungi, plants, invertebrates, and all vertebrates. In organisms that have no pineal gland and no sleep as we know it, melatonin's only plausible function is protection against oxidative stress — strong evidence that its original role was as an antioxidant and that the sleep/circadian signaling role was added later in evolution.
Two Pools: Pineal Hormone vs Local Synthesis
It is a common misconception that the pineal gland is the body's main source of melatonin. In fact there are two largely independent pools.
- Pineal (circulating) melatonin — produced rhythmically by the pineal gland in response to signals from the suprachiasmatic nucleus (the master clock), released into the bloodstream and cerebrospinal fluid at night, and responsible for circadian and sleep signaling through MT1 and MT2 receptors. This pool is measured in picograms per milliliter of plasma and is what most people mean by "melatonin levels."
- Extrapineal (local) melatonin — synthesized inside individual cells throughout the body: the gut (which contains far more melatonin than the pineal), the retina, skin, bone marrow, lymphocytes, and — importantly — the mitochondria of most cell types. This pool is not released into blood in large quantities, does not follow a strong day-night rhythm, and acts locally as a tissue antioxidant and cytoprotectant. Tissue concentrations here can exceed circulating levels by orders of magnitude.
The discovery that mitochondria themselves contain the enzymes to make melatonin (and have receptors that respond to it) reframed the molecule entirely. The local pool is not about telling the body what time it is — it is an on-site antioxidant manufactured exactly where reactive oxygen species are generated. This is why oral melatonin's antioxidant effects do not depend solely on raising blood levels, and why the local system is thought to matter as much as, or more than, the pineal hormone for tissue protection.
Direct Free-Radical Scavenging & the Antioxidant Cascade
Melatonin directly neutralizes a broad range of reactive oxygen and nitrogen species: the hydroxyl radical (·OH, the most damaging radical in biology), peroxyl radicals, singlet oxygen, superoxide, hydrogen peroxide, nitric oxide, and peroxynitrite. Its electron-rich indole ring readily donates electrons or hydrogen atoms to quench these species. It is particularly effective against the hydroxyl radical, for which the body has no dedicated enzyme.
What sets melatonin apart from most antioxidants is the free-radical scavenging cascade. Vitamin C or vitamin E typically neutralizes one radical and is then either regenerated or spent. Melatonin instead reacts with radicals to form a series of metabolites — and each metabolite is itself an effective scavenger. A single melatonin molecule can therefore deactivate multiple radicals through a relay of its own breakdown products:
- Cyclic 3-hydroxymelatonin (c3OHM) — formed when melatonin scavenges two hydroxyl radicals; an early, characteristic footprint of melatonin’s antioxidant action.
- N1-acetyl-N2-formyl-5-methoxykynuramine (AFMK) — a major downstream metabolite that retains potent radical-scavenging and anti-inflammatory activity.
- N1-acetyl-5-methoxykynuramine (AMK) — derived from AFMK; an even more efficient scavenger that also inhibits inducible nitric oxide synthase and quenches reactive nitrogen species.
Because the parent molecule and its metabolites all participate, this is sometimes described as melatonin’s "antioxidant cascade" or "radical-scavenging cascade," and it is the mechanistic reason a relatively small amount of melatonin can have an outsized protective effect. Crucially, the reactions are not readily reversible into pro-oxidant intermediates, so melatonin does not show the pro-oxidant "switch" that can complicate high-dose vitamin C or iron-loaded systems.
Indirect Antioxidant Actions (Glutathione, SOD, Catalase)
Beyond directly scavenging radicals, melatonin strengthens the cell’s own enzymatic defense network — it is both an antioxidant and an antioxidant-system regulator.
- Glutathione — melatonin stimulates gamma-glutamylcysteine synthetase, the rate-limiting enzyme of glutathione synthesis, raising intracellular reduced glutathione (GSH), the cell’s primary thiol antioxidant. This dovetails with thiol-based defenses supported by N-acetylcysteine.
- Superoxide dismutase (SOD) — melatonin upregulates both the mitochondrial (MnSOD/SOD2) and cytosolic (CuZnSOD/SOD1) isoforms, accelerating conversion of superoxide to hydrogen peroxide.
- Catalase and glutathione peroxidase (GPx) — melatonin increases the activity of these enzymes, which detoxify the hydrogen peroxide produced by SOD into water, closing the loop and preventing peroxide from generating new hydroxyl radicals.
- Pro-oxidant enzyme suppression — melatonin downregulates inducible nitric oxide synthase (iNOS) and pro-oxidant signaling, reducing the upstream production of reactive nitrogen species.
- Nrf2 pathway — melatonin activates the Nrf2 transcription factor, the master switch that turns on dozens of antioxidant and phase-II detoxification genes.
The combination is synergistic: melatonin mops up radicals directly, raises glutathione to handle the rest, and tunes the enzymatic machinery (SOD → catalase/GPx) so the superoxide-to-water detox chain runs cleanly. This dual action — chemical scavenger plus enzyme inducer — is why melatonin is sometimes called a "master" antioxidant.
Why Melatonin Concentrates in Mitochondria
Mitochondria are the cell’s power plants, and the price of generating ATP through the electron transport chain is a constant leak of superoxide and other reactive oxygen species — the great majority of the cell’s radical burden originates here. A molecule that can protect the mitochondrion protects the cell.
Several converging lines of evidence explain melatonin’s mitochondrial focus:
- Accumulation: Melatonin reaches markedly higher concentrations inside mitochondria than in blood or cytosol. Its amphiphilic nature lets it pass the outer and inner mitochondrial membranes, and there is evidence of active uptake via the oligopeptide transporters PEPT1/PEPT2 — so it is delivered to the precise site of radical production rather than diluted through the body.
- On-site synthesis: Mitochondria contain AANAT and ASMT and can synthesize melatonin internally, making them self-supplying for their own antioxidant.
- Membrane-bound receptors: Functional MT1 receptors sit on the mitochondrial membrane, allowing melatonin to signal locally — stabilizing membrane potential and inhibiting the mitochondrial permeability transition pore (mPTP), a key trigger of cell death.
- Bioenergetic protection: By limiting electron leak and oxidative damage to electron-transport-chain complexes, melatonin helps preserve efficient ATP production and reduces the chance of the mitochondrion tipping into apoptosis.
This places melatonin alongside other mitochondria-targeted protectants such as CoQ10, alpha lipoic acid, and PQQ — but melatonin is distinctive in being water- and lipid-soluble, internally synthesized, and active as both a direct scavenger and a receptor-mediated regulator within the organelle.
Sleep & Circadian Rhythm
The role most people associate with melatonin is timing sleep. Released by the pineal gland after dark, circulating melatonin acts on MT1 and MT2 receptors in the suprachiasmatic nucleus to lower alertness and shift the circadian phase. It is best understood as a chronobiotic — a signal that tells the body it is night — rather than a sedative or sleeping pill. It nudges the timing of the sleep-wake cycle more than it forces sleep.
Clinically, the strongest evidence is for circadian problems rather than ordinary insomnia:
- Circadian rhythm disorders — delayed sleep-wake phase disorder, non-24-hour sleep-wake disorder (common in totally blind people), and shift-work disorder respond to correctly timed low-dose melatonin.
- Jet lag — melatonin taken at the destination’s bedtime helps re-entrain the clock, with the effect strongest crossing five or more time zones eastward.
- Sleep-onset insomnia — modest reductions in the time to fall asleep; effect sizes are smaller than prescription hypnotics but with a far better safety profile.
- Older adults — because endogenous production declines with age, supplementation can partially restore a flagging nighttime signal, particularly for sleep onset.
Timing and dose matter more than potency: small physiological doses taken at the right hour outperform large doses taken at the wrong hour. Bright light at night (especially blue-wavelength screen light) suppresses pineal melatonin, so light hygiene is part of any melatonin strategy. See Insomnia for the broader clinical picture.
Mitochondrial & Neuroprotection
The brain is uniquely vulnerable to oxidative stress: it consumes a large share of the body’s oxygen, is rich in easily oxidized lipids, and has comparatively modest antioxidant enzyme reserves. Melatonin’s ability to cross the blood-brain barrier, concentrate in neuronal mitochondria, and quench the hydroxyl radical makes it a natural candidate for neuroprotection.
Preclinical and early clinical research has examined melatonin in:
- Neurodegenerative disease — in models of Alzheimer’s and Parkinson’s disease, melatonin reduces oxidative damage, limits amyloid-beta and tau-related toxicity, and protects dopaminergic neurons. Human evidence is still preliminary and mostly directed at the sleep and circadian disruption that accompany these conditions.
- Ischemia-reperfusion and brain injury — in stroke and traumatic-brain-injury models, melatonin limits the oxidative burst that occurs when blood flow is restored and stabilizes mitochondria against the permeability transition.
- Neuroinflammation — by suppressing iNOS, lowering peroxynitrite, and damping inflammatory signaling, melatonin reduces the self-amplifying loop of oxidative stress and microglial activation.
The unifying theme is mitochondrial: melatonin defends neuronal mitochondria, the loss of which underlies much age-related and disease-related neurodegeneration. This overlaps conceptually with the broader topic of oxidative stress and with longevity protocols.
Cardiovascular Effects
The heart and blood vessels are heavily mitochondria-dependent and sensitive to oxidative injury, and melatonin has measurable cardiovascular actions. Pineal melatonin contributes to the normal nighttime dip in blood pressure; loss of that dip ("non-dipping") is itself a cardiovascular risk marker.
- Blood pressure — controlled-release melatonin at night has lowered nocturnal blood pressure in several small trials, partly by improving endothelial nitric-oxide availability and reducing sympathetic tone.
- Endothelial & lipid protection — as a lipid-phase antioxidant, melatonin limits oxidation of LDL particles, an early step in atherosclerosis, and protects the endothelium from oxidative injury.
- Ischemia-reperfusion — in experimental myocardial infarction and cardiac surgery models, melatonin reduces infarct size and protects against the oxidative damage that occurs on reperfusion, again by stabilizing mitochondria and limiting the permeability transition.
- Metabolic links — disrupted melatonin signaling (from shift work or chronic light-at-night) is epidemiologically associated with metabolic syndrome, and melatonin influences insulin secretion through pancreatic MT receptors.
The clinical cardiovascular evidence is still developing and trials are generally small, but the mechanistic case — antioxidant protection of cardiac mitochondria and the vascular endothelium — is consistent. See Cardiology for related conditions.
Immune Modulation
Melatonin is an immune regulator as well as an antioxidant, and the two roles are linked: much immune-mediated tissue damage is oxidative, and melatonin both restrains it and supports a balanced response. Immune cells themselves synthesize melatonin, and melatonin receptors are present on lymphocytes.
- Immunostimulatory at rest — melatonin can enhance T-helper cell activity, natural killer cell function, and cytokine production under normal conditions, supporting host defense.
- Anti-inflammatory under stress — in the setting of excessive or acute inflammation, melatonin damps the production of pro-inflammatory cytokines and reactive species, behaving as an immunomodulator that pushes toward balance rather than simply "boosting" immunity.
- Inflammasome and redox signaling — melatonin inhibits NLRP3 inflammasome activation and NF-κB signaling, two central drivers of chronic inflammation, largely by lowering the oxidative tone that activates them.
This context-dependent behavior — supportive when the system is quiet, restraining when it is overactive — is characteristic of regulators rather than blunt stimulants, and is one reason melatonin is studied in inflammatory and age-related immune decline ("immunosenescence").
Adjunct Oncology Research
Melatonin has been studied as an adjunct in cancer research — alongside standard treatment, never as a replacement for it. Interest stems from several observations: melatonin has oncostatic and antioxidant properties in laboratory models, its production is suppressed by light-at-night, and epidemiological work has linked long-term night-shift work and circadian disruption to higher rates of certain cancers (which led the IARC to classify shift work involving circadian disruption as a probable carcinogen).
Lines of investigation include:
- Laboratory oncostatic effects — melatonin slows proliferation, promotes apoptosis in tumor cells, has anti-angiogenic effects, and is notably anti-estrogenic in hormone-sensitive (e.g., breast) cancer models.
- Adjunct trials — in supportive-care studies melatonin has been added to chemotherapy or radiotherapy, where meta-analyses report associations with improved tumor response and one-year survival and reduced treatment toxicity (fatigue, low blood counts, neuropathy). These trials are mostly small and heterogeneous, so the findings are considered promising but not definitive.
- Symptom and sleep support — melatonin is also used in oncology simply to improve the disrupted sleep and circadian rhythm that are common during treatment.
The honest summary is that melatonin is an active area of supportive-oncology research with encouraging but not yet conclusive evidence; any use during cancer treatment must be coordinated with the treating oncology team. See Oncology.
Dietary Factors & Age-Related Decline
Because melatonin is made from tryptophan via serotonin, the raw materials and cofactors of that pathway influence production. Adequate dietary tryptophan (from eggs, dairy, poultry, fish, legumes, seeds) supplies the starting material, and cofactors such as vitamin B6, folate, magnesium, and zinc support the enzymes that convert it. Some foods — tart cherries, pistachios, certain grains, grapes, and tomatoes — contain measurable phytomelatonin and have modestly raised circulating levels in small studies.
The dominant influences in practice, however, are light and age:
- Light exposure — bright and especially blue-wavelength light at night suppresses pineal melatonin; morning daylight and evening darkness reinforce a healthy rhythm. Evening screen use is the most common modern disruptor.
- Age-related decline — nocturnal melatonin production peaks in childhood and then falls progressively; by older adulthood, peak nighttime levels are a fraction of youthful values. The pineal gland calcifies and AANAT activity declines. This drop parallels the decline of glutathione and other defenses and is one proposed contributor to the rising oxidative burden of aging — the rationale for studying melatonin within longevity protocols.
- Medications & lifestyle — beta-blockers (which block the pineal’s adrenergic drive), NSAIDs, caffeine and alcohol near bedtime, and chronic stress can all blunt endogenous melatonin.
Forms, Low-Dose vs High-Dose & Timing
Melatonin is sold as immediate-release tablets, sublingual and liquid forms (faster onset), and prolonged/controlled-release tablets (designed to mimic the overnight curve and help with sleep maintenance). A prescription prolonged-release 2 mg formulation is licensed in parts of Europe for short-term insomnia in adults over 55. In the United States it is an over-the-counter supplement, and independent testing has repeatedly found large discrepancies between the labeled and actual melatonin content of consumer products — reputable, third-party-tested brands matter.
Dose is best thought of in two regimes:
- Low (physiological) dose — roughly 0.3 to 1 mg — approximates the amount the pineal gland releases at night and is generally the most appropriate dose for sleep and circadian re-timing. Studies suggest 0.3–0.5 mg is often as effective as higher doses for sleep onset, with fewer next-day effects and less risk of receptor desensitization. Common retail doses of 3–10 mg are well above physiological need for sleep.
- High (pharmacological) dose — tens to hundreds of milligrams — used in the research settings where melatonin’s antioxidant and cytoprotective properties are the target (neuroprotection, critical illness, adjunct oncology). Such doses should only be used under medical supervision; they are not necessary, and not advisable, for ordinary sleep complaints.
Timing for sleep and circadian use: for sleep onset, take a low dose about 30–60 minutes before the desired bedtime. For phase-shifting (jet lag, delayed sleep phase), the time relative to your own rhythm matters more than the dose — a small evening dose advances the clock; the wrong timing can shift it the wrong way. Start low, keep light dim afterward, and avoid daytime dosing unless a clinician is deliberately resetting an inverted rhythm.
Safety, Side Effects & Interactions
Melatonin has a wide safety margin and low acute toxicity, and short-term use in adults is generally well tolerated. Important considerations:
- Common side effects — daytime drowsiness or grogginess (especially at higher doses), headache, dizziness, nausea, and unusually vivid dreams. These usually resolve at lower doses.
- Next-day impairment & driving — because it can cause drowsiness, avoid driving or operating machinery for several hours after a dose, particularly with controlled-release forms or higher amounts.
- Anticoagulants & antiplatelets — melatonin may modestly increase bleeding risk and can interact with warfarin; monitor when combining and discuss with a clinician.
- Sedatives & CNS depressants — additive sedation with benzodiazepines, "Z-drugs," alcohol, opioids, and antihistamines.
- Blood pressure & diabetes medications — melatonin can lower nighttime blood pressure (occasionally interacting with antihypertensives) and may affect glucose tolerance and insulin secretion; people with diabetes should monitor blood sugar.
- Immunosuppressants — given its immune-modulating activity, caution is advised in transplant recipients or those on immunosuppressive therapy.
- Drug metabolism — melatonin is cleared mainly by CYP1A2; strong CYP1A2 inhibitors (e.g., fluvoxamine) can raise melatonin levels substantially, while smoking induces CYP1A2 and lowers them.
- Pregnancy, breastfeeding & children — data are limited; routine use is not established and should be guided by a clinician. Pediatric use (e.g., in autism-related sleep problems) is studied but should be supervised, and accidental pediatric ingestions of gummy products have risen sharply — store securely.
- Hormonal & mood effects — very high doses may influence reproductive hormones; melatonin can also lower mood or worsen depressive symptoms in some individuals.
None of this is medical advice. Melatonin is a hormone, not merely a sleep aid, and the lowest effective dose for the shortest necessary time is the prudent default; discuss higher "antioxidant-dose" use with a qualified clinician.
Key Research Papers
The following peer-reviewed papers cover melatonin’s antioxidant chemistry, mitochondrial role, and clinical applications. Russel J. Reiter is the central figure in melatonin-antioxidant research and appears in several entries below.
- Reiter RJ, Mayo JC, Tan DX, Sainz RM, Alatorre-Jimenez M, Qin L. Melatonin as an antioxidant: under promises but over delivers. Journal of Pineal Research. 2016;61(3):253–278. doi:10.1111/jpi.12360
- Tan DX, Manchester LC, Esteban-Zubero E, Zhou Z, Reiter RJ. Melatonin as a potent and inducible endogenous antioxidant: synthesis and metabolism. Molecules. 2015;20(10):18886–18906. doi:10.3390/molecules201018886
- Reiter RJ, Tan DX, Rosales-Corral S, Galano A, Zhou XJ, Xu B. Mitochondria: central organelles for melatonin’s antioxidant and anti-aging actions. Molecules. 2018;23(2):509. doi:10.3390/molecules23020509
- Galano A, Tan DX, Reiter RJ. Melatonin as a natural ally against oxidative stress: a physicochemical examination. Journal of Pineal Research. 2011;51(1):1–16. doi:10.1111/j.1600-079X.2011.00916.x
- Tan DX, Manchester LC, Liu X, Rosales-Corral SA, Acuna-Castroviejo D, Reiter RJ. Mitochondria and chloroplasts as the original sites of melatonin synthesis. Journal of Pineal Research. 2013;54(2):127–138. doi:10.1111/jpi.12026
- Reiter RJ, Mayo JC, Tan DX, et al. Melatonin and the theory of free radicals and oxidative damage. (overview of the antioxidant cascade and AFMK/AMK). Journal of Pineal Research. — Search PubMed
- Hardeland R. Antioxidative protection by melatonin: multiplicity of mechanisms from radical detoxification to radical avoidance. Endocrine. 2005;27(2):119–130. doi:10.1385/ENDO:27:2:119
- Rodriguez C, Mayo JC, Sainz RM, et al. Regulation of antioxidant enzymes: a significant role for melatonin. Journal of Pineal Research. 2004;36(1):1–9. doi:10.1111/j.1600-079X.2003.00092.x
- Ferracioli-Oda E, Qawasmi A, Bloch MH. Meta-analysis: melatonin for the treatment of primary sleep disorders. PLoS One. 2013;8(5):e63773. doi:10.1371/journal.pone.0063773
- Auld F, Maschauer EL, Morrison I, Skene DJ, Riha RL. Evidence for the efficacy of melatonin in the treatment of primary adult sleep disorders. Sleep Medicine Reviews. 2017;34:10–22. doi:10.1016/j.smrv.2016.06.005
- Wang YM, Jin BZ, Ai F, et al. The efficacy and safety of melatonin in concurrent chemotherapy or radiotherapy for solid tumors: a meta-analysis of randomized controlled trials. Cancer Chemotherapy and Pharmacology. 2012;69(5):1213–1220. doi:10.1007/s00280-012-1902-2
- Tordjman S, Chokron S, Delorme R, et al. Melatonin: pharmacology, functions and therapeutic benefits. Current Neuropharmacology. 2017;15(3):434–443. doi:10.2174/1570159X14666161228122115
Live PubMed Searches
- PubMed: Melatonin antioxidant & oxidative stress
- PubMed: Melatonin, mitochondria & free radicals
- PubMed: Melatonin cascade metabolites (AFMK / AMK)
- PubMed: Melatonin, glutathione & SOD
- PubMed: Melatonin, sleep & circadian rhythm
- PubMed: Melatonin neuroprotection
- PubMed: Melatonin & cardiovascular health
- PubMed: Melatonin as oncology adjunct
External Authoritative Resources
- NIH Office of Dietary Supplements — Melatonin
- NCCIH — Melatonin: What You Need To Know
- MedlinePlus — Melatonin
- PubMed — All research on melatonin
Connections
- Caffeine, Adenosine & Why Coffee Stops Working — interactive animation
- Sleep Stages & Your Body Clock — interactive animation
- Apigenin
- All Antioxidants
- Glutathione
- CoQ10
- NAC (Glutathione Precursor)
- Alpha Lipoic Acid
- PQQ
- NAD+ & NMN
- Astaxanthin
- Curcumin
- Methylene Blue
- Tryptophan (Melatonin Precursor)
- Oxidative Stress
- Longevity Protocols
- Insomnia
- Neurology
- Alzheimer's Disease
- Parkinson's Disease
- Cardiology
- Oncology
- Endocrinology
- Psychiatry
- Magnesium
- Selenium
- Vitamin E