Coenzyme Q10 (CoQ10 / Ubiquinone / Ubiquinol)
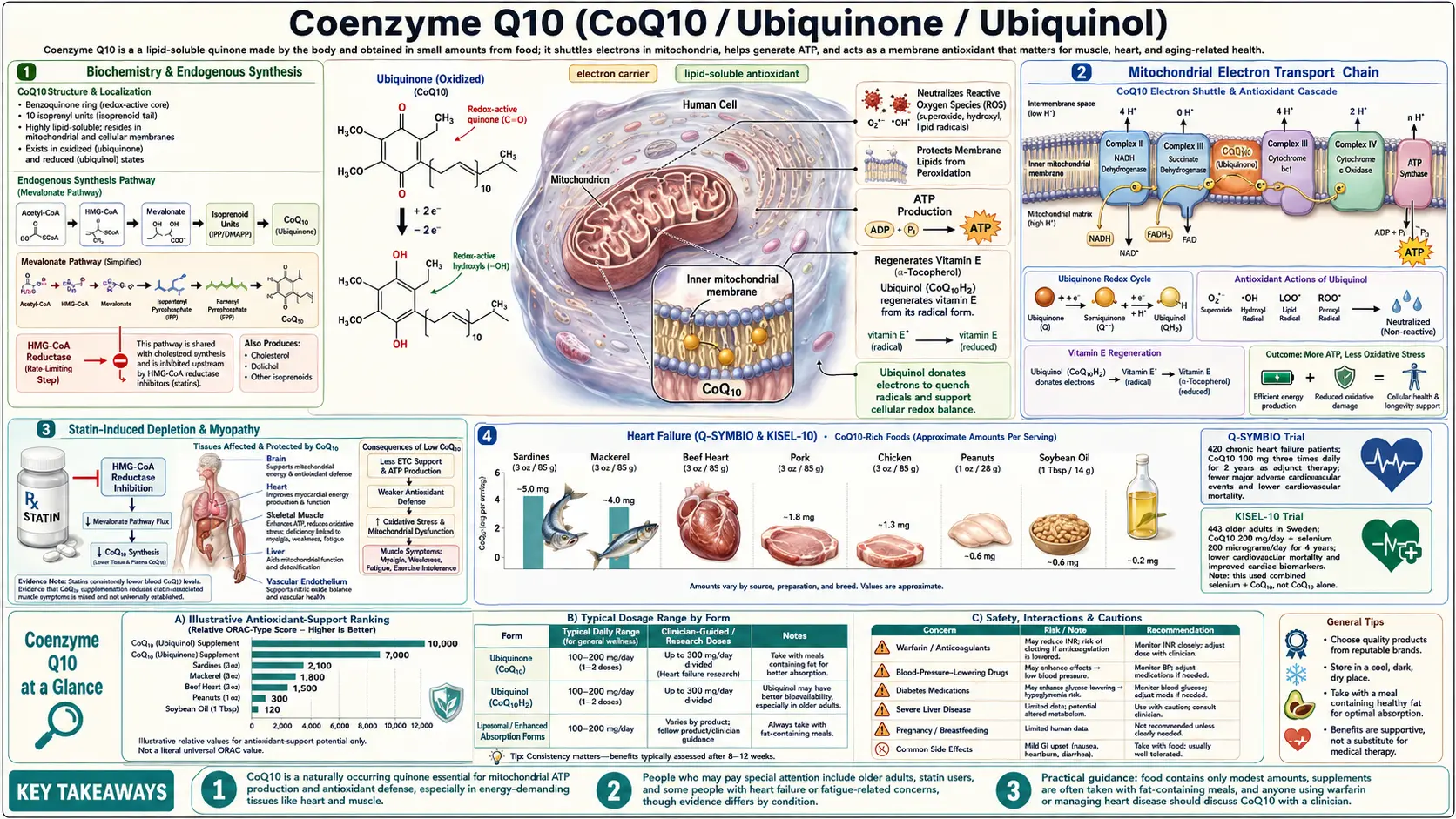
Coenzyme Q10 (CoQ10) is a fat-soluble benzoquinone that lives in the inner mitochondrial membrane and shuttles electrons between Complex I/II and Complex III of the electron transport chain — the single most important step in cellular ATP production. The body synthesizes its own CoQ10 via the same biochemical pathway that statins block, so statin therapy reliably lowers blood CoQ10 levels. Tissue concentrations also fall sharply after age 40. The strongest clinical evidence is in heart failure (Q-SYMBIO trial: 43% reduction in cardiovascular mortality), statin-induced myopathy, migraine prevention, and mitochondrial disease.
Interactive Visualization Mitochondria & ATP — watch your cells make energy Follow electrons through the transport chain and watch the ATP-synthase motor spin — then block Complex IV and see the chain stall. Launch → Interactive Visualization Free Radicals & Your Antioxidant Network Follow one superoxide radical down the whole relay — SOD, catalase, glutathione, vitamin E, vitamin C, NADPH — then release free iron and watch a membrane tear itself apart. Launch →
Table of Contents
- Biochemistry & Endogenous Synthesis
- Mitochondrial Electron Transport Chain
- Statin-Induced Depletion & Myopathy
- Heart Failure (Q-SYMBIO & KISEL-10)
- Hypertension & Endothelial Function
- Migraine Prevention
- Mitochondrial Diseases & Primary CoQ10 Deficiency
- Fertility, Sperm & Egg Quality
- Parkinson's Disease & Neurodegeneration
- Periodontal Disease & Gum Health
- Skin Health & Anti-Aging
- Forms: Ubiquinone vs Ubiquinol vs Liposomal
- Recommended Dosage
- Cautions and Contraindications
- Research Papers and References
- Connections
- Featured Videos
Biochemistry & Endogenous Synthesis
Coenzyme Q10 (also called ubiquinone, ubidecarenone, or coenzyme Q) is a fat-soluble quinone with a benzoquinone head and an isoprenoid tail of 10 isoprene units (hence "Q10"). The benzoquinone ring is the redox-active center, accepting and donating electrons in a two-step cycle; the long lipophilic tail anchors the molecule in the inner mitochondrial membrane and allows it to diffuse laterally to shuttle electrons between membrane-bound enzyme complexes.
CoQ10 exists in three interconvertible redox states:
- Ubiquinone (CoQ) — the fully oxidized form; can accept one electron to become the semiquinone radical, or two electrons plus two protons to become ubiquinol
- Semiquinone (CoQH·) — the partially reduced one-electron intermediate; key in the Q-cycle at Complex III
- Ubiquinol (CoQH&sub2;) — the fully reduced form; the antioxidant-active form that quenches lipid peroxyl radicals in membranes and lipoproteins
The body synthesizes CoQ10 through a long biochemical pathway that begins with acetyl-CoA, runs through HMG-CoA and the mevalonate pathway (the same pathway that makes cholesterol), and ends with the assembly of the benzoquinone head and the 10-isoprene tail. The benzoquinone ring is derived from tyrosine; the methyl groups come from S-adenosylmethionine (SAMe). Multiple cofactors are required — B vitamins (B2, B3, B6, B12, folate), tyrosine, and trace minerals. Any deficiency in this pathway, or any drug that inhibits it, reduces CoQ10 synthesis.
Tissue concentrations of CoQ10 are highest in the heart, kidneys, liver, and brain — tissues with the largest mitochondrial demand. Heart muscle in particular has the highest per-gram concentration in the body. Levels rise from birth through young adulthood, peak in the 20s, and then decline steadily — by age 80, heart CoQ10 levels are roughly half of peak. This age-related decline is one of the proposed mechanisms of mitochondrial aging.
Dietary CoQ10 is modest. The richest sources are organ meats (heart, liver, kidney), fatty fish (mackerel, sardines, herring, salmon), and to a lesser extent beef, chicken, eggs, and certain plant oils. Typical Western diets supply 3-6 mg/day — far below the 100-300 mg/day used in supplementation studies.
Mitochondrial Electron Transport Chain
CoQ10's primary function is electron transport. The inner mitochondrial membrane houses five protein complexes (I through V) that together transfer electrons from food-derived NADH and FADH&sub2; to molecular oxygen, generating the proton gradient that drives ATP synthesis. CoQ10 sits between the first stages and the later ones — it is the membrane-soluble electron carrier that connects them.
- Complex I (NADH:ubiquinone oxidoreductase) — oxidizes NADH from glycolysis and the TCA cycle, passing two electrons to ubiquinone to make ubiquinol
- Complex II (succinate dehydrogenase) — oxidizes succinate (from the TCA cycle), passing electrons via FADH&sub2; to ubiquinone
- Complex III (cytochrome bc1) — takes electrons from ubiquinol and passes them to cytochrome c; this is where the famous "Q-cycle" runs
- Complex IV (cytochrome c oxidase) — transfers electrons from cytochrome c to molecular oxygen, generating water
- Complex V (ATP synthase) — uses the proton gradient to synthesize ATP
Without CoQ10, electrons cannot flow from Complexes I/II to Complex III. The result is impaired ATP synthesis, accumulated NADH (which feeds back to inhibit the TCA cycle), increased lactate production, and increased mitochondrial superoxide leak from the stalled complexes — a vicious cycle of falling energy production and rising oxidative damage. Tissues with high energy demand — the heart, brain, kidneys, and muscle — suffer first when CoQ10 supply is inadequate.
Beyond electron transport, CoQ10 has secondary mitochondrial roles. It stabilizes the mitochondrial permeability transition pore, helping protect against apoptosis triggered by calcium overload. It serves as a cofactor for the mitochondrial uncoupling proteins (UCP1-3), supporting thermogenesis and metabolic flexibility. And as ubiquinol it directly scavenges the superoxide and lipid peroxyl radicals generated within the inner mitochondrial membrane.
This is the conceptual overlap with alpha lipoic acid: both molecules support mitochondrial bioenergetics, both act as antioxidants in the lipid phase, and ALA in its reduced DHLA form regenerates oxidized CoQ10 back to active ubiquinol. The two are complementary supplements for any mitochondrial-aging or metabolic-recovery protocol.
Statin-Induced Depletion & Myopathy
Statin drugs (atorvastatin, simvastatin, rosuvastatin, pravastatin, etc.) lower LDL cholesterol by inhibiting HMG-CoA reductase — the rate-limiting enzyme of the mevalonate pathway. Because CoQ10 synthesis branches off the same mevalonate pathway downstream of HMG-CoA reductase, statins inhibit CoQ10 synthesis as an unavoidable consequence of their mechanism.
Multiple studies have measured the effect:
- Statin therapy reduces serum CoQ10 levels by 30-50% within 2-4 weeks of initiation, with the degree of depletion correlated to statin potency (rosuvastatin and atorvastatin produce the largest decreases)
- Muscle biopsy studies show 30-40% reductions in intramuscular CoQ10 in statin users compared to controls, particularly in patients with statin-associated muscle symptoms
- Liver, heart, and brain CoQ10 levels also decline, though the clinical significance of these tissue-level changes remains debated
Statin-Associated Muscle Symptoms (SAMS) — pain, weakness, cramping, exercise intolerance — affect 10-25% of statin users in real-world observational studies (lower in randomized trials, which exclude muscle-prone patients). The mitochondrial-dysfunction hypothesis, supported by muscle-biopsy data showing reduced respiratory chain capacity, is the leading mechanism.
Whether CoQ10 supplementation reliably prevents or reverses statin myopathy remains contested. Meta-analyses of randomized trials have produced mixed results — some (Banach et al. 2015; Skarlovnik et al. 2014) showing significant reductions in muscle pain at 100-200 mg/day, others (Taylor et al. 2015) showing no benefit. The discrepancy likely reflects heterogeneity in baseline deficiency, study duration, and outcome measures. In clinical practice, a trial of 100-300 mg/day CoQ10 for 4-12 weeks is a reasonable, low-risk first step for patients with statin-associated muscle symptoms before considering statin switch or discontinuation.
Functional medicine practitioners frequently recommend prophylactic CoQ10 (100-200 mg/day) for anyone on long-term statin therapy, regardless of symptoms, on the rationale that subclinical mitochondrial depletion is biologically certain even if pain is not.
Heart Failure (Q-SYMBIO & KISEL-10)
Heart failure is the indication for which CoQ10 has the strongest evidence base. The heart muscle has the highest mitochondrial density of any tissue in the body and the highest CoQ10 concentration. In heart failure — particularly the systolic form (reduced ejection fraction, HFrEF) — myocardial CoQ10 levels fall by 30-50% below age-matched controls, and the degree of deficiency correlates with disease severity.
Q-SYMBIO trial (Mortensen et al., 2014, JACC Heart Failure)
The landmark trial. 420 patients with NYHA Class III-IV (moderate-to-severe) heart failure on standard therapy, randomized to CoQ10 100 mg three times daily (300 mg/day total) or placebo for 2 years. Results:
- 43% reduction in major adverse cardiovascular events (MACE) — the primary endpoint (hazard ratio 0.50, p = 0.003)
- 43% reduction in cardiovascular mortality
- 42% reduction in all-cause mortality
- Significant improvement in NYHA functional class at the 16-week interim analysis
- No safety concerns; tolerability comparable to placebo
The mortality reduction was larger than that produced by most pharmaceutical heart failure agents (beta-blockers, ACE inhibitors, ARBs) added to standard therapy in landmark drug trials. The fact that CoQ10 is a regulated nutraceutical without patent protection explains why it has never been promoted commercially to cardiologists at the scale of pharmaceuticals.
KISEL-10 trial (Alehagen et al., 2013, International Journal of Cardiology)
443 elderly Swedish adults (ages 70-88) without known heart disease, randomized to CoQ10 200 mg/day + selenium 200 mcg/day, or placebo, for 4 years. At 5-year follow-up: 54% reduction in cardiovascular mortality in the CoQ10 + selenium group. The protective effect persisted at 10-year and 12-year follow-ups, suggesting a durable mortality benefit that outlasted the active treatment period — a striking finding consistent with reversal of underlying mitochondrial dysfunction rather than mere symptom suppression.
Both trials used CoQ10 in combination with standard medical therapy, not as a replacement. The most clinically useful framing is that CoQ10 is an evidence-based adjunct to guideline-directed heart failure therapy — one of the few nutraceuticals with double-blind randomized mortality data supporting its use.
For patients with heart failure, the typical protocol is 100 mg three times daily of ubiquinol (the reduced form, better absorbed in older patients with reduced enterohepatic conversion capacity), taken with fatty meals.
Hypertension & Endothelial Function
Multiple small trials and meta-analyses have shown that CoQ10 produces modest but consistent reductions in blood pressure — approximately 11 mmHg systolic and 7 mmHg diastolic in pooled analyses of 12 clinical trials (Rosenfeldt et al., 2007, Journal of Human Hypertension). The effect is most pronounced in patients with documented essential hypertension; minimal change is seen in normotensive subjects.
Mechanisms include improved endothelial nitric oxide bioavailability (CoQ10 protects NO from oxidative destruction by superoxide), reduced peripheral vascular resistance through improved mitochondrial function in vascular smooth muscle, and reduced aldosterone-driven sodium retention. The blood-pressure-lowering effect is typically visible after 4-12 weeks of 100-200 mg/day CoQ10.
CoQ10 also reduces oxidative damage to LDL particles, an early step in atherosclerotic plaque formation. Ubiquinol is the first antioxidant consumed when LDL is exposed to oxidative stress — it protects LDL from peroxidation before vitamin E is engaged. This positions CoQ10 as a relevant supplement for anyone with elevated ApoB or Lipoprotein(a) who is trying to slow vascular oxidative damage.
Migraine Prevention
CoQ10 is one of the better-studied nutraceutical interventions for migraine prevention. Two pivotal randomized trials established the evidence base:
- Sandor et al. (2005, Neurology) — 42 patients with episodic migraine randomized to CoQ10 300 mg/day or placebo for 3 months. The CoQ10 group experienced a 27% reduction in attack frequency at month 3 versus 15% for placebo, and a near-doubling of patients achieving >50% reduction in attack frequency (47% vs 14%).
- Hershey et al. (2007, Headache) — Pediatric study in children with frequent migraine. After 3 months of CoQ10 supplementation, mean attack frequency fell from 19 to 8 per month, with corresponding reductions in attack severity and disability.
Subsequent meta-analyses (Parohan et al. 2020, Sazali et al. 2021) have confirmed a moderate, statistically significant reduction in attack frequency, headache duration, and severity. CoQ10 has earned a "Level C" (possibly effective) recommendation in the American Academy of Neurology and American Headache Society 2012 guidelines for migraine prevention, alongside other nutraceutical options including riboflavin (vitamin B2), magnesium, and butterbur.
The proposed mechanism is restoration of mitochondrial function in cortical neurons — migraine is increasingly understood as a disorder of cortical mitochondrial energy reserve, with attacks triggered when neuronal energy demand exceeds supply (cortical spreading depression). CoQ10 alongside riboflavin (the FMN/FAD cofactor for Complex II) and magnesium (calcium-channel modulator) forms the standard "mitochondrial migraine prevention stack" used in integrative neurology.
Typical dose: 100 mg three times daily (300 mg/day total) for at least 3 months before assessing response.
Mitochondrial Diseases & Primary CoQ10 Deficiency
Primary CoQ10 deficiency is a rare group of inherited disorders caused by mutations in genes encoding CoQ10 biosynthesis enzymes (PDSS1, PDSS2, COQ2, COQ4-9, ADCK3/4). Presentations vary from infantile multisystem disease to adult-onset cerebellar ataxia, encephalopathy, or steroid-resistant nephrotic syndrome.
Primary CoQ10 deficiency is one of the few mitochondrial diseases for which supplementation produces dramatic, sometimes life-saving clinical improvement — particularly when started early. Doses for primary deficiency are very high: 30-50 mg/kg/day in children, often 1,200-3,000 mg/day in adults, typically of ubiquinol for absorption.
For secondary mitochondrial disorders — MELAS (mitochondrial encephalopathy, lactic acidosis, stroke-like episodes), Leigh syndrome, Kearns-Sayre syndrome, MERRF, and chronic progressive external ophthalmoplegia — CoQ10 is a routine component of the "mitochondrial cocktail" along with creatine, L-carnitine, alpha lipoic acid, B-vitamins, and vitamin E. Clinical response varies but mortality and progression slow in most case series.
Acquired secondary mitochondrial dysfunction — the type that accompanies chronic fatigue syndrome, fibromyalgia, long-COVID, chemotherapy-induced fatigue, and aging itself — is the much more common clinical scenario, and CoQ10 at 200-600 mg/day is a reasonable evidence-informed intervention.
Fertility, Sperm & Egg Quality
Both sperm and oocytes are exceptionally mitochondria-rich cells, and both decline in fertility with age in part because of accumulated mitochondrial dysfunction. CoQ10 has been studied in both contexts.
Male fertility
The Italian Balercia trials (2004, 2009) randomized men with idiopathic asthenozoospermia (low sperm motility) to CoQ10 200-300 mg/day or placebo for 6 months. CoQ10 treatment significantly improved sperm motility, sperm density, and seminal antioxidant capacity, with subsequent improvements in clinical pregnancy rates. Several follow-up trials and a 2013 meta-analysis (Lafuente et al.) confirmed the effect.
Female fertility
The Bentov & Casper trials at the University of Toronto (Bentov 2014) tested CoQ10 supplementation in women undergoing IVF, particularly those of advanced reproductive age (35+). Pretreatment with 200 mg ubiquinol three times daily for 60 days before IVF cycle start improved ovarian response, increased the number of high-quality embryos, and increased fertilization rates. The mechanism appears to be restoration of mitochondrial ATP production in aging oocytes during the energy-intensive meiotic spindle formation that decides chromosomal segregation.
CoQ10 is now a standard component of fertility supplementation protocols in many reproductive endocrinology clinics, alongside DHEA, vitamin D, omega-3 fatty acids, and folate.
Parkinson's Disease & Neurodegeneration
Parkinson's disease involves dysfunction of mitochondrial Complex I in dopaminergic neurons of the substantia nigra. CoQ10 was therefore a biologically plausible neuroprotective intervention.
The Shults trial (2002, Archives of Neurology) randomized 80 early-stage Parkinson's patients to CoQ10 300, 600, or 1,200 mg/day or placebo for 16 months. The high-dose group showed a 44% slower progression of disability on the UPDRS scale — a striking signal that generated significant excitement.
However, the larger and longer QE3 trial (2014, JAMA Neurology) of 600 patients on CoQ10 1,200 or 2,400 mg/day for 16 months was terminated early for futility — no significant difference from placebo on any clinical outcome. The disappointing replication suggests the original signal was likely a chance finding or population-specific effect.
The current consensus is that CoQ10 does not meaningfully slow Parkinson's progression at standard or high doses. It remains a reasonable component of broader mitochondrial-supportive regimens but should not be recommended as disease-modifying therapy. Similar negative results have emerged for amyotrophic lateral sclerosis (ALS) trials and Huntington's disease.
For age-related cognitive decline outside specific neurodegenerative diseases, CoQ10 may contribute to broader mitochondrial protection but does not have strong stand-alone evidence for cognition.
Periodontal Disease & Gum Health
The original 1976 work of Karl Folkers and Edward Wilkinson demonstrated CoQ10 deficiency in gingival tissue from patients with periodontitis, and topical or systemic CoQ10 supplementation improved bleeding scores, pocket depth, and gum-tissue regeneration. Subsequent trials have been smaller and less consistent, but several modern dental clinics use CoQ10 (50-100 mg/day oral, sometimes with topical gel) as adjunctive therapy after scaling and root planing.
The mechanism is local mitochondrial support in rapidly turning over gingival epithelium and connective tissue, plus reduced oxidative damage from neutrophil respiratory burst during periodontal inflammation.
Skin Health & Anti-Aging
CoQ10 levels in the epidermis fall sharply with age and UV exposure. Topical CoQ10 (0.3-3%) penetrates the stratum corneum and has been shown in vehicle-controlled split-face studies to reduce periorbital wrinkle depth, improve skin smoothness, and reduce visible photodamage over 6-8 weeks. The mechanism is reduced lipid peroxidation in skin cell membranes and protection of mitochondrial function in keratinocytes and fibroblasts.
Oral CoQ10 also contributes — serum levels are correlated with epidermal levels, and 6 months of 60-150 mg/day oral CoQ10 has been shown to reduce wrinkles around the eyes and improve skin smoothness in placebo-controlled trials.
CoQ10 is a common ingredient in mid- and high-end skincare products, often combined with vitamin E, vitamin C, and niacinamide for combined antioxidant + barrier-repair effect.
Forms: Ubiquinone vs Ubiquinol vs Liposomal
- Ubiquinone (oxidized CoQ10) — the standard, lower-cost form available since the 1970s. Crystalline solid; must be converted to ubiquinol in the body before serving as antioxidant. Most cells perform this conversion efficiently when young and healthy, but elderly patients, those with chronic disease, and statin users show reduced conversion capacity.
- Ubiquinol (reduced CoQ10) — the antioxidant-active reduced form, commercially available since 2006. Approximately 3-4× more bioavailable than ubiquinone in patients over 50 or with absorption challenges. More expensive, but the preferred form for older adults, heart failure patients, statin users, and anyone with documented absorption problems. Best evidence form for serious clinical indications.
- Solubilized ubiquinone (with vitamin E, lecithin, or proprietary delivery systems like Q-Gel, Q-SorB, or BioActive Q) — standard ubiquinone in a fat-soluble carrier matrix. Bridges some of the bioavailability gap with ubiquinol at lower cost.
- Liposomal CoQ10 — phospholipid-encapsulated for enhanced absorption. Useful for patients with bile-flow or fat-absorption problems.
- MitoQ (mitoquinone) — a synthetic mitochondrial-targeted CoQ10 analog with a triphenylphosphonium cation attached. Concentrates inside mitochondria at 100-1,000× cytoplasmic levels. Used in research and high-end longevity protocols; expensive.
- Topical CoQ10 — 0.3-3% in serums and creams for dermatological use.
Practical guidance: For healthy adults under 50 doing general antioxidant or preventive supplementation, ubiquinone 100-200 mg/day with a fatty meal is the cost-effective choice. For patients over 50, statin users, heart failure, mitochondrial disease, or any setting where the clinical stakes are high, ubiquinol at 100-200 mg/day is the preferred form. Always take with fat for absorption — CoQ10 absorption increases roughly 3× when taken with a meal containing 10+ grams of fat versus on an empty stomach.
Recommended Dosage
- General antioxidant support / preventive — 100 mg/day ubiquinone (or 50-100 mg/day ubiquinol) with a fatty meal
- Statin myopathy prevention or treatment — 100-300 mg/day ubiquinol, divided doses, taken with meals; 4-12 week trial before assessing
- Heart failure (Q-SYMBIO protocol) — 100 mg three times daily ubiquinol (300 mg/day total) with meals, indefinitely
- Hypertension — 100-200 mg/day ubiquinone or ubiquinol, expecting 4-12 weeks for visible effect
- Migraine prevention — 100 mg three times daily (300 mg/day total) for at least 3 months, often combined with riboflavin 400 mg/day and magnesium 400-600 mg/day
- Fertility (male or female) — 200-300 mg/day ubiquinol for 3-6 months before conception attempts or IVF cycle
- Mitochondrial disease (acquired secondary) — 200-600 mg/day ubiquinol, often as part of a broader mitochondrial cocktail
- Primary CoQ10 deficiency (inherited) — 30-50 mg/kg/day in children, 1,200-3,000 mg/day in adults, ubiquinol, under specialist supervision
- Periodontal support — 50-100 mg/day systemic, often with topical CoQ10 gel applied to gums
- Topical anti-aging — 0.3-3% in a stable serum or cream, applied once or twice daily
Timing matters. CoQ10 is fat-soluble and absorption increases 3-4× when taken with a meal containing dietary fat. Plasma half-life is approximately 33 hours, so once-daily dosing is acceptable for most indications — but divided dosing (2-3 times per day with fatty meals) is preferred for higher therapeutic doses (300+ mg/day) to maximize absorption.
Cautions and Contraindications
CoQ10 is one of the safest supplements in routine use, with millions of patient-years of clinical experience and an excellent tolerability profile. Important considerations:
- Warfarin interaction — CoQ10 has a quinone structure similar to vitamin K and may modestly reduce the anticoagulant effect of warfarin (Coumadin), resulting in a 10-15% reduction in INR. Patients on warfarin who start CoQ10 should have INR monitored more frequently for 4-6 weeks until stable. The interaction is not relevant to direct oral anticoagulants (DOACs: apixaban, rivaroxaban, dabigatran, edoxaban).
- Blood pressure medications — CoQ10's mild antihypertensive effect can add to ACE inhibitors, ARBs, calcium channel blockers, beta-blockers, and diuretics. Monitor blood pressure and consider downward dose adjustment of antihypertensives if CoQ10 produces >5-10 mmHg reduction.
- Diabetes medications — CoQ10 has mild glucose-lowering effects in some patients. Monitor blood glucose when starting; rarely requires medication adjustment.
- Cancer chemotherapy — theoretical concern that antioxidants might interfere with chemotherapy regimens whose mechanism depends on oxidative damage (anthracyclines, platinum agents). The clinical data are reassuring — CoQ10 has actually been studied as a cardioprotectant against anthracycline cardiotoxicity (doxorubicin/Adriamycin) with positive results — but coordinate with the oncology team before adding CoQ10 during active cancer treatment.
- GI side effects — nausea, upper abdominal discomfort, and loose stools occur in less than 1% of users, almost always at doses >300 mg/day. Usually resolves with divided dosing and taking with food.
- Skin rash — rare; idiosyncratic
- Insomnia — uncommon at higher doses (>300 mg/day); take morning and midday rather than evening if affected
- Pregnancy and breastfeeding — CoQ10 is occasionally used during pregnancy for pre-eclampsia prevention (small trials suggest benefit) and for migraine that worsens in pregnancy; safety data are reassuring but not extensive. Discuss with obstetrician.
Research Papers and References
The following PubMed search links provide curated entry points into the published clinical and mechanistic literature on Coenzyme Q10.
- Q-SYMBIO heart failure trial — PubMed: Q-SYMBIO Coenzyme Q10 heart failure Mortensen
- KISEL-10 trial (CoQ10 + selenium long-term mortality) — PubMed: KISEL-10 Coenzyme Q10 selenium Alehagen
- CoQ10 and statin-associated muscle symptoms — PubMed: Coenzyme Q10 statin myopathy
- CoQ10 hypertension and blood pressure (Rosenfeldt meta-analysis) — PubMed: Coenzyme Q10 hypertension blood pressure
- CoQ10 migraine prevention (Sandor, Hershey, Parohan) — PubMed: Coenzyme Q10 migraine prevention
- CoQ10 male fertility, sperm motility (Balercia) — PubMed: Coenzyme Q10 male fertility sperm motility
- CoQ10 and IVF, female fertility, egg quality (Bentov) — PubMed: Coenzyme Q10 IVF oocyte quality
- CoQ10 and Parkinson's disease (Shults, QE3 trial) — PubMed: Coenzyme Q10 Parkinson disease QE3
- Primary and secondary CoQ10 deficiency — PubMed: Primary Coenzyme Q10 deficiency
- CoQ10 and chronic fatigue syndrome / fibromyalgia — PubMed: Coenzyme Q10 chronic fatigue fibromyalgia
- Ubiquinol vs ubiquinone bioavailability — PubMed: Ubiquinol ubiquinone bioavailability
- CoQ10 cardioprotection during anthracycline chemotherapy — PubMed: Coenzyme Q10 doxorubicin cardiotoxicity
- CoQ10 periodontal disease (Folkers / Wilkinson) — PubMed: Coenzyme Q10 periodontal disease
- CoQ10 topical and skin antioxidant — PubMed: Coenzyme Q10 topical skin
- MitoQ (mitoquinone) targeted antioxidant research — PubMed: MitoQ mitochondrial-targeted antioxidant
External Authoritative Resources
- Linus Pauling Institute — Coenzyme Q10 Micronutrient Information Center
- NCCIH — Herbs and Supplements at a Glance
- MedlinePlus — Coenzyme Q10
- PubMed — All research on coenzyme Q10
Connections
- Free Radicals & Your Antioxidant Network — interactive animation
- Mitochondria & ATP — interactive animation
- All Antioxidants
- Alpha Lipoic Acid
- Heart Failure
- Cardiovascular Disease
- Fatigue
- Headache & Migraine
- Chronic Fatigue Syndrome
- Fibromyalgia
- Reproductive Medicine
- Parkinson's Disease
- Oxidative Stress
- NAC (Glutathione Precursor)
- NAD+ & NMN
- Methylene Blue
- Longevity Protocols
- Vitamin E
- Vitamin K2
- Vitamin B2 (Riboflavin)
- Vitamin B3 (Niacin)
- Selenium
- Magnesium
- Cysteine
- Methionine
- Tyrosine
- Creatine
- Omega-3 Fatty Acids
- Organ Meats
- Sardines
- Salmon
- Lipid Panel
- Apolipoprotein B
- Coronary Calcium Score
- Statins & CAC