Glutathione for Lung Disease (Cystic Fibrosis, COPD, ARDS)
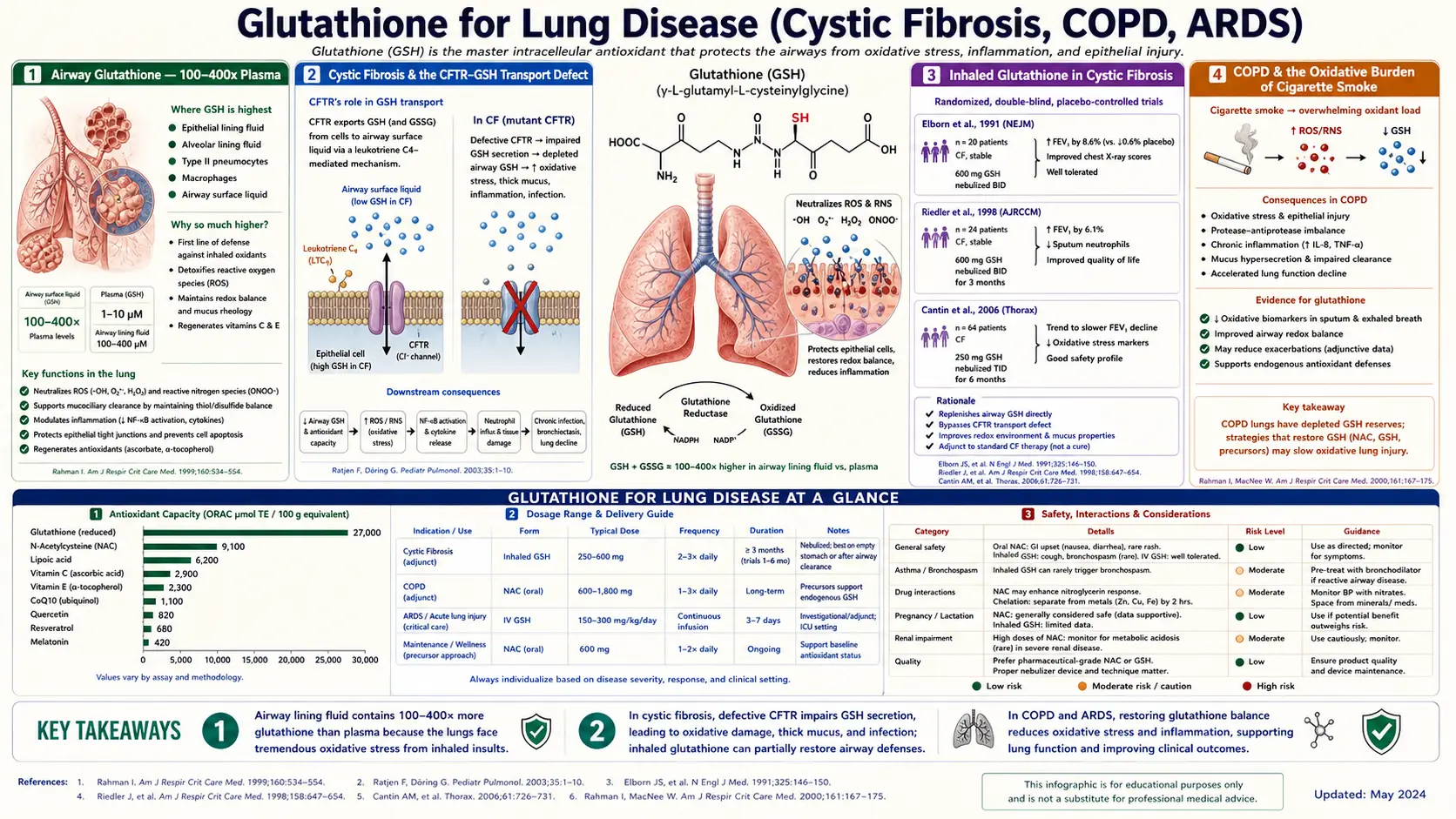
The lungs are uniquely exposed to oxidative stress — they are the only organ in continuous direct contact with 21% atmospheric oxygen, they receive the entire cardiac output, and they handle inhaled pollutants, allergens, infectious agents, and (in some patients) cigarette smoke. To cope with this constant oxidative burden, the airway maintains glutathione in alveolar lining fluid at concentrations 100-400× higher than plasma — the highest extracellular GSH concentration anywhere in the body. In cystic fibrosis, mutant CFTR cannot transport glutathione into the airway lumen, leaving CF patients with airway GSH levels under 10% of normal and accelerated neutrophil-mediated airway destruction. In COPD, cigarette smoke depletes bronchial glutathione and oxidatively damages the airway epithelium. The PANTHEON trial (Zheng 2014, Lancet Respiratory Medicine) showed N-acetylcysteine 600 mg twice daily reduced COPD exacerbations by 22% in moderate-to-severe disease. Inhaled glutathione for CF, oral NAC for COPD, and adjunctive NAC/GSH in ARDS together form the major glutathione-targeted interventions in pulmonary medicine.
Interactive Visualization Free Radicals & Your Antioxidant Network Follow one superoxide radical down the whole relay — SOD, catalase, glutathione, vitamin E, vitamin C, NADPH — then release free iron and watch a membrane tear itself apart. Launch →
Table of Contents
- Airway Glutathione — 100-400× Plasma
- Cystic Fibrosis & the CFTR-GSH Transport Defect
- Inhaled Glutathione in Cystic Fibrosis
- COPD & the Oxidative Burden of Cigarette Smoke
- The PANTHEON Trial & BRONCUS
- NAC as Mucolytic — Disulfide Bond Disruption
- ARDS & Ventilator-Associated Lung Injury
- Idiopathic Pulmonary Fibrosis (IFIGENIA, PANTHER)
- Chronic Sinusitis & Nebulized GSH
- Asthma & the NAC Paradox
- Practical Patient Protocols by Condition
- Cautions Specific to Pulmonary Patients
- Key Research Papers
- Connections
- Featured Videos
Airway Glutathione — 100-400× Plasma
The respiratory epithelium maintains the most concentrated extracellular glutathione environment anywhere in the body. Alveolar lining fluid (the thin liquid film coating the alveolar surface) contains glutathione at concentrations of 100-400 micromolar, compared to plasma levels of 1-3 micromolar — roughly a 100-400-fold concentration gradient. The total airway glutathione pool (including the bronchial epithelial cell intracellular GSH and the airway surface fluid) represents one of the largest organ-system GSH stores in the body.
This concentration is maintained by active transport of intracellular glutathione (synthesized in alveolar type II cells and bronchial epithelial cells) into the airway lumen via the CFTR chloride channel and the MRP family of efflux transporters. The high airway GSH is the front-line chemical defense against:
- Inhaled oxidant pollutants — ozone, nitrogen dioxide, sulfur dioxide, particulate matter (PM2.5), and other air pollutants directly react with airway GSH, being neutralized before they can damage the underlying epithelium.
- Reactive oxygen species from immune cells — alveolar macrophages and recruited neutrophils generate large amounts of superoxide, hydrogen peroxide, and hypochlorous acid as part of their bactericidal respiratory burst. Airway GSH buffers this oxidative output, limiting collateral damage to the airway epithelium.
- Cigarette smoke oxidants — cigarette smoke contains approximately 1015 free radicals per puff in the gas phase alone, plus quinones, semiquinones, and aldehydes in the particulate phase. Airway GSH is depleted within minutes of smoking and takes hours to replenish.
- Inhaled microorganism virulence factors — many bacterial and fungal toxins generate ROS as part of their pathogenicity; airway GSH buffers this damage.
When airway GSH is depleted — whether through CFTR dysfunction, chronic cigarette smoke exposure, severe acute respiratory inflammation, or systemic GSH deficiency — the airway epithelium becomes vulnerable to oxidative damage from these same agents. Chronic depletion accelerates airway remodeling, mucus hypersecretion, fibrosis, and progressive airflow obstruction. This is the unifying mechanism underlying CF airway disease, COPD, ARDS, and progressive interstitial lung diseases.
Cystic Fibrosis & the CFTR-GSH Transport Defect
Cystic fibrosis is the genetic disease that most clearly illustrates the role of glutathione in lung biology. CF is caused by mutations in the CFTR gene encoding the cystic fibrosis transmembrane conductance regulator — an apical-membrane chloride channel expressed in airway, intestinal, biliary, pancreatic, and reproductive epithelia.
The dominant CF mutation (F508del, accounting for ~70% of CF alleles) and other major mutations produce dysfunctional CFTR that cannot transport chloride properly. The downstream consequences are well-known: thick, dehydrated airway mucus that impairs mucociliary clearance, leading to chronic bacterial colonization (Pseudomonas, Staphylococcus, Burkholderia), persistent neutrophilic inflammation, progressive bronchiectasis, and ultimately respiratory failure.
A less widely appreciated function of CFTR is that it also transports glutathione (in addition to chloride). When CFTR is non-functional, glutathione cannot be transported from airway epithelial cells into the airway lumen. The consequence is dramatic:
- CF airway surface fluid GSH is reduced to ~10% of normal in the airways of CF patients
- The remaining GSH is largely oxidized (GSSG), so functional reducing capacity is even more reduced
- Inflammatory neutrophils continue to generate oxidative mediators (myeloperoxidase, neutrophil elastase, ROS) without the normal GSH-mediated buffer
- The result is amplified oxidative damage to airway epithelium, accelerated airway remodeling, and a vicious cycle of inflammation and damage
This GSH-transport defect is partly independent of the chloride-transport defect. Even with effective mucus clearance and bacterial control, the airway antioxidant deficiency persists and contributes to disease progression. This is the biological rationale for direct airway glutathione delivery in CF: bypass the broken transport mechanism by inhaling glutathione directly into the airway lumen.
For the broader picture of CF management, see our Cystic Fibrosis page.
Inhaled Glutathione in Cystic Fibrosis
Multiple clinical trials have studied inhaled (nebulized) glutathione as antioxidant therapy in CF. The intervention rationale is straightforward: nebulized GSH delivers reduced glutathione directly to the airway surface, bypassing the broken CFTR-mediated transport mechanism.
Bishop trial (2005)
A pivotal early trial enrolled 19 CF patients to inhaled reduced glutathione 600 mg twice daily for 8 weeks vs placebo. The glutathione group showed:
- Significant increase in airway surface fluid GSH (measured by sputum induction)
- Modest but statistically significant improvement in FEV1
- Reduction in markers of oxidative damage (8-isoprostane in exhaled breath condensate)
- Good tolerability with minimal adverse events
Griese trial (2013)
A larger German trial of 153 CF patients tested inhaled glutathione 600 mg twice daily for 6 months. Results were mixed: the glutathione arm did not show statistically significant FEV1 improvement at 6 months, but did show measurable improvement in some secondary outcomes (BMI, modest sputum biomarker changes). Heterogeneity in baseline severity, antibiotic use, and CFTR genotype likely contributed to the diluted effect.
Cochrane review (Calabrese 2015 update)
The Cochrane systematic review of inhaled glutathione in CF concluded that modest evidence supports improvements in FEV1 and reduced exacerbations, but called for larger trials with standardized protocols. The Cochrane authors noted the high quality of the underlying biological rationale and the safety of the intervention, recommending continued investigation.
Practical use
In current CF practice, inhaled glutathione is not standard of care but is used in some specialized centers as adjunctive therapy. Typical regimen: reduced glutathione 300-600 mg in 3-4 mL saline, nebulized twice daily, prepared by a compounding pharmacy (glutathione must be reduced form, not oxidized, and is air-sensitive). Many CF clinicians prefer oral NAC 600-1200 mg twice daily as a simpler systemic alternative that has shown similar though smaller benefits in some trials.
The arrival of CFTR modulator therapy (elexacaftor/tezacaftor/ivacaftor, marketed as Trikafta) has transformed the CF clinical landscape and reduced the relative importance of antioxidant adjuncts. With effective modulator therapy restoring partial CFTR function, airway GSH transport is partially restored. However, modulators are not curative, and antioxidant adjuncts may still have a role — particularly for the ~10% of CF patients with mutations not addressed by current modulators.
COPD & the Oxidative Burden of Cigarette Smoke
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide, responsible for over 3 million deaths annually. The disease encompasses chronic bronchitis (airway mucus hypersecretion and inflammation), emphysema (destruction of alveolar walls and loss of elastic recoil), and small airway disease — usually overlapping in any given patient.
The primary causal mechanism is cigarette smoke exposure. Each cigarette puff contains approximately 1015-1017 free radicals in the gas phase (semiquinones, peroxyl radicals, nitric oxide) plus quinones, semiquinones, aldehydes (acrolein, formaldehyde), and reactive aromatic compounds in the particulate phase. This oxidative burden:
- Depletes airway and intracellular glutathione within minutes; full replenishment takes 12-24 hours
- Recruits neutrophils that release additional ROS, elastase, and matrix metalloproteinases
- Inactivates alpha-1-antitrypsin (the major elastase inhibitor) through oxidation of its critical methionine residue, permitting unchecked elastase damage to alveolar walls
- Damages alveolar type II cells, impairing surfactant production
- Activates NF-κB and the inflammatory cytokine cascade
- Promotes goblet cell hyperplasia and mucus hypersecretion
- Drives epigenetic and gene expression changes that persist long after smoking cessation
Even decades after smoking cessation, ex-smokers show persistent reductions in glutathione/cysteine status, ongoing oxidative airway damage markers, and progressive airflow obstruction. The "memory" of cigarette smoke exposure includes a sustained antioxidant deficiency that contributes to continued COPD progression.
This is the conceptual basis for the long-running interest in antioxidant supplementation (particularly NAC) as adjunctive therapy in COPD. The hypothesis: restore the cellular GSH pool that smoking has depleted, reduce ongoing oxidative damage, and slow the rate of FEV1 decline.
For the full picture of COPD management, see our COPD page.
The PANTHEON Trial & BRONCUS
BRONCUS (Decramer et al., 2005, The Lancet)
The Bronchitis Randomized On NAC Cost-Utility Study was a 3-year randomized double-blind placebo-controlled trial of NAC 600 mg daily vs placebo in 523 COPD patients in Europe. The trial had mixed results:
- Failed primary endpoint: No significant difference in annual FEV1 decline rate (~50 mL/year in both arms)
- Failed secondary endpoint: No significant difference in COPD exacerbation rate overall
- Subgroup signal: Patients not taking inhaled corticosteroids did show reduced exacerbations with NAC, suggesting the active treatment was being masked by inhaled steroid effects
BRONCUS was widely interpreted as a negative trial that dampened enthusiasm for NAC in COPD throughout the late 2000s. However, the subgroup signal kept investigator interest alive, and a key insight emerged: the 600 mg/day NAC dose used in BRONCUS may have been too low to produce meaningful airway antioxidant effects.
PANTHEON (Zheng et al., 2014, Lancet Respiratory Medicine)
The Chinese PANTHEON trial (Prevention of Acute exacerbations of chronic bronchitis with NAC randomized HEterogeneity ON) tested NAC at twice the BRONCUS dose: 600 mg twice daily (1200 mg total/day) vs placebo for 1 year, in 1006 moderate-to-severe COPD patients:
- Primary endpoint MET: 22% reduction in annual exacerbation rate (1.16 vs 1.49 exacerbations/year; p<0.001)
- Significant reduction in moderate and severe exacerbations specifically
- Reduced time to first exacerbation
- Similar safety profile between NAC and placebo
- Benefit was independent of inhaled corticosteroid use
PANTHEON established 600 mg twice daily as the standard NAC dose for COPD and reversed the negative reading of BRONCUS. The mechanism is most likely a combination of:
- Restoration of bronchial epithelial intracellular glutathione
- Reduction of neutrophil-mediated oxidative damage
- Mucolytic effect (NAC cleaves mucin disulfide bonds, see next section)
- Modest anti-inflammatory effect through GSH-mediated NF-κB suppression
Following PANTHEON, the GOLD (Global Initiative for Chronic Obstructive Lung Disease) guidelines updated their recommendations to include NAC 600 mg twice daily as adjunctive therapy for patients with frequent exacerbations, particularly those not on inhaled corticosteroids or with phenotypes suggesting predominant oxidative stress mechanisms.
NAC as Mucolytic — Disulfide Bond Disruption
Beyond its glutathione-precursor role, NAC has direct mucolytic activity that is mechanistically independent of the antioxidant pathway. Airway mucus contains mucin glycoproteins (predominantly MUC5AC and MUC5B in healthy airways; MUC5AC dominates in disease states like chronic bronchitis and asthma) cross-linked by disulfide bonds between cysteine residues. The cross-linking is what creates the viscoelastic gel structure of mucus.
The free sulfhydryl group on N-acetylcysteine can directly attack and cleave these mucin disulfide bonds, reducing mucus viscosity and improving the rheological properties. The effect is dose-dependent and dose-related: higher local concentrations produce more mucolysis. This is why nebulized NAC (10-20% solution) is used acutely in cystic fibrosis exacerbations, bronchiectasis with thick secretions, and intubated ICU patients with impaired airway clearance.
Oral NAC at the PANTHEON dose (600 mg BID) produces measurable but modest mucolytic effect — some patients report reduced sputum viscosity and easier expectoration. The clinical benefit in COPD likely combines this mucolytic effect with the antioxidant effect, with the relative contributions varying by patient phenotype.
Other mucolytic strategies that complement NAC include:
- Hypertonic saline (3-7%) — osmotically draws water into the airway, hydrating mucus; standard adjunct in CF and bronchiectasis
- Dornase alfa (Pulmozyme) — recombinant DNase that cleaves DNA from neutrophil debris in CF mucus; CF-specific therapy
- Carbocisteine — a cysteine derivative used in Europe for chronic bronchitis with claimed mucolytic and antioxidant effects
- Erdosteine and ambroxol — mucolytics used in some European countries
For chronic bronchitis patients with productive cough and thick sputum, the combination of oral NAC 600 mg BID + adequate hydration + regular airway clearance maneuvers (huff coughing, oscillatory PEP, postural drainage) often substantially reduces sputum burden and improves quality of life.
ARDS & Ventilator-Associated Lung Injury
Acute respiratory distress syndrome (ARDS) is acute, severe, diffuse alveolar injury from sepsis, pneumonia, aspiration, trauma, or other systemic insults, resulting in non-cardiogenic pulmonary edema, severe hypoxemia, and reduced lung compliance. ICU mortality remains 30-40% even with optimal supportive care including low-tidal-volume ventilation and prone positioning.
The pathophysiology of ARDS involves massive oxidative damage to the alveolar-capillary barrier. Activated neutrophils release ROS, proteases, and inflammatory mediators that disrupt endothelial and epithelial integrity, allowing protein-rich edema fluid to flood the alveolar space. Alveolar lining fluid GSH is depleted within hours of ARDS onset, removing the primary chemical defense against further oxidative damage.
Multiple small ICU trials have tested IV NAC and IV glutathione as adjunctive ARDS therapy:
- Bernard 1997 trial — 48 ARDS patients randomized to IV NAC 70 mg/kg every 8 hours for 10 days. NAC group showed faster resolution of ARDS, improved oxygenation index, and a trend toward reduced mortality (NS due to small N)
- Domenighetti 1997 trial — IV NAC in 32 patients with septic ARDS; improvements in oxygenation but no mortality benefit
- Suter 1994 trial — high-dose NAC in ARDS; modest improvements in pulmonary function
- Meta-analyses (Adhikari 2007, others) — pooled NAC data suggest reduction in mechanical ventilation days but no clear mortality benefit
The clinical synthesis: IV NAC has biological plausibility and shows some signal of benefit in ARDS, but the effect size is modest and most studies are small. NAC is not standard of care for ARDS but is used in some intensive care units, particularly for sepsis-related ARDS where the additional anti-inflammatory effects may help. Standard dosing is 100-150 mg/kg IV initially, then 50-100 mg/kg every 6-8 hours.
For ventilator-associated lung injury more broadly, the antioxidant rationale extends to all critically ill ventilated patients, but the evidence is even weaker than for ARDS specifically. NAC adjunctive use remains a clinician-by-clinician decision.
Idiopathic Pulmonary Fibrosis (IFIGENIA, PANTHER)
Idiopathic pulmonary fibrosis (IPF) is a progressive scarring lung disease of unknown cause, with median survival of 3-5 years from diagnosis. Oxidative stress is implicated in the pathobiology: lower airway GSH is depleted, oxidative damage markers are elevated, and aberrant epithelial-mesenchymal transition (driving fibroblast activation) is partly redox-mediated.
IFIGENIA (Demedts et al., 2005, NEJM)
The first major NAC trial in IPF. 155 patients randomized to NAC 600 mg three times daily plus standard prednisone + azathioprine therapy, versus standard therapy alone, for 12 months. The NAC arm showed:
- Slower decline in FVC
- Slower decline in DLCO
- Better preservation of quality of life
IFIGENIA produced enthusiasm for NAC as part of standard IPF therapy.
PANTHER-IPF (2012, NEJM)
The follow-up PANTHER trial randomized IPF patients to three arms: triple therapy (prednisone + azathioprine + NAC), NAC alone, or placebo. The triple therapy arm was stopped early due to increased mortality and hospitalization in the active treatment group — an unexpected and concerning finding that overturned the prior practice of triple therapy for IPF.
The NAC-monotherapy vs placebo arms continued. Final analysis (2014) showed:
- No significant difference in FVC decline between NAC and placebo
- No significant difference in mortality
- No significant difference in acute exacerbations
- NAC monotherapy was disappointingly negative
Subgroup analyses
Post-hoc analyses of PANTHER suggested that patients with the TT genotype of the TOLLIP rs3750920 polymorphism may benefit from NAC monotherapy while patients with other genotypes do not. This pharmacogenomic finding has not yet been prospectively validated but is being explored in ongoing IPF research.
Current standard of care for IPF is now nintedanib or pirfenidone (anti-fibrotic agents) rather than NAC. NAC is not recommended as standard IPF therapy. Some integrative pulmonologists continue to use NAC adjunctively for patients with documented antioxidant deficiency or with the TOLLIP TT genotype, but this remains exploratory.
Chronic Sinusitis & Nebulized GSH
Chronic rhinosinusitis (CRS) is persistent inflammation of the paranasal sinus mucosa, often with biofilm formation, fungal colonization, and oxidative damage to the sinus epithelium. Standard treatment combines saline irrigation, intranasal corticosteroids, occasional courses of antibiotics, and (in refractory cases) functional endoscopic sinus surgery.
Nebulized glutathione has been used as adjunctive therapy in chronic sinusitis, typically delivered via specialized sinus nebulizers (e.g., RinoFlow) that produce particle sizes appropriate for sinus penetration rather than alveolar deposition. Small studies and clinical experience suggest:
- Reduced symptom burden (nasal congestion, post-nasal drip, headache)
- Reduced reliance on antibiotics for sinus exacerbations
- Improved tolerance of saline irrigation
- Possible reduction in biofilm burden through disulfide bond disruption (parallel to mucin-disrupting mechanism in airway mucus)
Typical regimen: reduced glutathione 100-200 mg in 3-5 mL saline, nebulized via sinus nebulizer once or twice daily. Often combined with topical lactoferrin or xylitol for synergistic antimicrobial effects. The intervention requires compounding pharmacy preparation of fresh reduced glutathione solution (oxidizes within days even refrigerated).
Evidence base is limited (mostly observational and small case series) but the safety profile is excellent and clinical experience favorable. Best used as adjunct in patients failing standard therapy or wanting to reduce antibiotic exposure.
Asthma & the NAC Paradox
Asthma shares pathophysiological features with COPD — airway inflammation, oxidative stress, and mucus production — and might therefore seem like a natural target for NAC therapy. However, the asthma situation is more complex.
- Some asthmatic patients have reduced bronchial GSH and might theoretically benefit from precursor supplementation
- Small trials of oral NAC in asthma have shown modest reductions in symptom scores and inhaled bronchodilator use
- The paradoxical bronchospasm risk — nebulized NAC at high concentrations can trigger bronchospasm in some asthmatic patients, particularly those with sulfite sensitivity. The same risk exists at lower frequency with oral NAC.
- Sulfa allergy is not a true contraindication — NAC's sulfhydryl group is chemically distinct from sulfonamide-containing "sulfa drugs", but some patients with sulfa sensitivity tolerate NAC poorly
- The clinical recommendation: NAC may be considered in carefully selected asthmatic patients with refractory disease, after supervised initial dose to verify tolerability
For most asthma patients, the standard of care remains inhaled corticosteroids, long-acting beta-agonists, leukotriene modifiers, and (for severe disease) biologic agents targeting IgE (omalizumab), IL-5 (mepolizumab, reslizumab), or IL-4/IL-13 (dupilumab). NAC is at most an adjunctive consideration.
Practical Patient Protocols by Condition
COPD (moderate-to-severe, frequent exacerbations)
- NAC 600 mg twice daily — PANTHEON-validated dose for exacerbation reduction
- Continue indefinitely — benefits depend on continued use
- Add glycine 3-5 g/day if pursuing comprehensive GSH support
- Selenium 100-200 mcg/day
- Maintain inhaled bronchodilators and inhaled corticosteroids per pulmonologist
- Smoking cessation if applicable (the single most important intervention)
- Pneumococcal and influenza vaccination
Cystic fibrosis
- CFTR modulator therapy (Trikafta) per CF specialist — primary therapy for amenable mutations
- Oral NAC 600 mg twice daily — systemic GSH support
- Inhaled glutathione 300-600 mg twice daily via nebulizer (compounding pharmacy preparation) — consider in specialized centers
- Inhaled hypertonic saline 7% twice daily — standard mucus hydration
- Dornase alfa per CF protocol
- Airway clearance therapy daily
- Selenium 100-200 mcg/day
- Pancreatic enzyme replacement, vitamin ADEK supplementation per CF protocol
ARDS (ICU setting, by clinician decision)
- Standard ARDS care: lung-protective ventilation (low tidal volume, low plateau pressure), prone positioning for severe cases, conservative fluid management
- IV NAC 70-100 mg/kg every 6-8 hours as adjunctive antioxidant therapy — not standard of care but biological rationale supports trial use
- Identification and treatment of underlying cause (sepsis, pneumonia, aspiration)
Chronic sinusitis (refractory)
- Standard care: saline irrigation, intranasal corticosteroids, treatment of underlying allergies or biofilm
- Nebulized glutathione 100-200 mg once or twice daily via sinus nebulizer (compounding pharmacy preparation)
- Consider oral NAC 600 mg twice daily for systemic support
- ENT evaluation if not responding to medical management
Asthma (selected patients)
- Standard of care: inhaled corticosteroid + long-acting beta-agonist, biologic agents for severe asthma
- Oral NAC 600 mg twice daily in carefully selected patients with refractory symptoms after supervised initial dose
- Avoid nebulized NAC due to bronchospasm risk
Idiopathic pulmonary fibrosis
- Standard of care: nintedanib or pirfenidone
- NAC not routinely recommended (PANTHER negative result)
- Consider in patients with TOLLIP TT genotype after specialist consultation
- Pulmonary rehabilitation, supplemental oxygen, lung transplant evaluation for advanced disease
Cautions Specific to Pulmonary Patients
- NAC paradoxical bronchospasm in asthmatics — the most important pulmonary-specific NAC caution. Some asthmatic patients develop bronchospasm with oral or particularly nebulized NAC. Perform supervised first dose in any known reactive airway patient, with bronchodilator available. Avoid nebulized NAC in asthmatic patients unless specifically indicated and monitored.
- Inhaled glutathione preparation — must be reduced (not oxidized) glutathione; air-sensitive and oxidizes within days even refrigerated. Requires compounding pharmacy with experience preparing GSH for inhalation. Use within 1-2 weeks of preparation.
- Sulfite sensitivity — some patients with sulfite-sensitive asthma have cross-reactivity with NAC and inhaled glutathione. Use cautiously and monitor closely.
- Drug interactions in pulmonary patients — NAC may modestly enhance nitroglycerin effects (relevant for patients with CAD comorbidity); no significant interactions with bronchodilators or inhaled corticosteroids.
- Acetylcysteine-tetracycline interaction — theoretical concern that NAC chelates tetracycline; separate dosing by 2+ hours if both are needed.
- Sulfurous breath odor — common with chronic NAC; can be socially limiting; reduce dose or take with food.
- GI side effects — nausea, indigestion, occasional diarrhea, particularly with high doses; usually resolves with food.
- Renal function — reduce NAC dose with significant CKD.
- Mucus over-clearance — rare paradoxical concern with high-dose mucolytic NAC: in patients with impaired cough or swallow function, very fluid mucus can pool in airways. Adequate airway clearance technique is essential.
- Pregnancy — chronic NAC use in pregnancy lacks safety data; avoid except for specific indication (acetaminophen overdose).
Key Research Papers
- Zheng JP, Wen FQ, Bai CX, Wan HY, Kang J, Chen P, Yao WZ, Ma LJ, Xia X, Raiteri L, Sardina M, Gao Y, Wang BS, Zhong NS (2014). Twice daily N-acetylcysteine 600 mg for exacerbations of chronic obstructive pulmonary disease (PANTHEON): a randomised, double-blind placebo-controlled trial. Lancet Respiratory Medicine. — PubMed
- Decramer M, Rutten-van Mölken M, Dekhuijzen PNR, et al. (2005). Effects of N-acetylcysteine on outcomes in chronic obstructive pulmonary disease (BRONCUS): a randomised placebo-controlled trial. The Lancet. — PubMed
- Demedts M, Behr J, Buhl R, et al. (2005). High-dose acetylcysteine in idiopathic pulmonary fibrosis (IFIGENIA). NEJM. — PubMed
- Idiopathic Pulmonary Fibrosis Clinical Research Network (2012, 2014). Randomized trial of N-acetylcysteine in idiopathic pulmonary fibrosis (PANTHER-IPF). NEJM. — PubMed
- Bishop C, Hudson VM, Hilton SC, Wilde C (2005). A pilot study of the effect of inhaled buffered reduced glutathione on the clinical status of patients with cystic fibrosis. Chest. — PubMed
- Griese M, Kappler M, Eismann C, Ballmann M, Junge S, Rietschel E, van Koningsbruggen-Rietschel S, Staab D, Rolinck-Werninghaus C, Mellies U, Kohnlein T, Wagner T, Konig S, Teschler H, Hanrahan JW, Heuer HE, Sciuto C, Cesetti V, Andrieux A, Wengert M, Dippold W (2013). Inhalation treatment with glutathione in patients with cystic fibrosis: a randomized clinical trial. American Journal of Respiratory and Critical Care Medicine. — PubMed
- Calabrese C, Tosco A, Abete P, Carnovale V, Basile C, Magliocca A, Quattrucci S, De Sanctis S, Alatri F, Mazzarella G, De Pietro C, Turino C, Melck D, Maniscalco M, Bianco A (2015). Randomized, single blind, controlled trial of inhaled glutathione vs placebo in patients with cystic fibrosis. Journal of Cystic Fibrosis. — PubMed
- Bernard GR, Wheeler AP, Arons MM, et al. (1997). A trial of antioxidants N-acetylcysteine and procysteine in ARDS. Chest. — PubMed
- Cantin AM, North SL, Hubbard RC, Crystal RG (1987). Normal alveolar epithelial lining fluid contains high levels of glutathione. Journal of Applied Physiology. — PubMed
- Gao L, Kim KJ, Yankaskas JR, Forman HJ (1999). Abnormal glutathione transport in cystic fibrosis airway epithelia. American Journal of Physiology — Lung Cellular and Molecular Physiology. — PubMed
- Rahman I, MacNee W (2000). Oxidative stress and regulation of glutathione in lung inflammation. European Respiratory Journal. — PubMed
- Sadowska AM, Manuel-Y-Keenoy B, De Backer WA (2007). Antioxidant and anti-inflammatory efficacy of NAC in the treatment of COPD: discordant in vitro and in vivo dose-effects: a review. Pulmonary Pharmacology & Therapeutics. — PubMed
PubMed Topic Searches
- PubMed: glutathione lung disease
- PubMed: NAC COPD trials
- PubMed: inhaled glutathione CF
- PubMed: CFTR glutathione transport
- PubMed: NAC mucolytic mechanism
- PubMed: ARDS NAC oxidative
- PubMed: IPF NAC trials
Connections
- Free Radicals & Your Antioxidant Network — interactive animation
- Glutathione Overview
- GSH Benefits Hub
- GSH for Liver Detoxification
- GSH for Aging (GlyNAC)
- GSH for Parkinson's
- NAC (Primary Precursor)
- Alpha Lipoic Acid
- CoQ10
- Cysteine
- Glycine
- Methionine
- Selenium
- Zinc
- Vitamin C
- Vitamin D
- Vitamin E
- Cystic Fibrosis
- COPD
- Asthma
- Chronic Bronchitis
- Pulmonary Fibrosis
- Chronic Sinusitis
- Cigarette Smoke
- Air Pollution
- Oxidative Stress
- All Antioxidants